





Abstract
Updating to corrected GLI TLCO reference equations from the original GLI equations in a clinical population results in small changes in the lower limit of normal that are more pronounced in females, but there is minimal effect on test interpretation https://bit.ly/2MTdErd
To the Editor:
The carbon monoxide transfer factor (TLCO) reference equations published by the Global Lung Function Initiative (GLI) in 2017 [1] have a number of advantages compared to previously published equations [2–8], including that they are derived from a large dataset (9710 subjects), use modern equipment, cover a wide age range (5–85 years) obviating the need for separate paediatric and adult equations, and use more sophisticated statistical techniques to account for variation and skewness across the age range. Following the publication of the GLI equations there were a number of studies, such as ours, that examined the impact of changing to the new equations in clinical and research settings [9–12]. Our study [9] analysed a large clinical dataset of adult and paediatric TLCO results. It showed that adoption of GLI TLCO reference equations in adults would lead to altered interpretation depending on the equations previously used, with larger effects seen when changing from Crapo [3] and Roca [5] equations, and to a greater extent in adult females. The effect on interpretation in children was less significant.
The 2017 TLCO reference equations from the GLI were recently updated to correct an error [13] caused by inclusion of a dataset that had likely incorrectly assigned the sex of participants. The correction was reported to impact adult females more than males with a mean±sd change in the percent predicted value of 1.02±2.0% for females and 0.6±0.4% for males. We aimed to document the impact of changing to the corrected GLI reference equations from the original 2017 equations, on predicted values, lower limits of normal (LLN), test interpretation and severity classification, in a predominately adult clinical population. Such an analysis is important, as it allows laboratories and clinicians to understand how updating to the corrected predicted values may impact test interpretation and, ultimately, patient diagnosis and management.
TLCO results over a 5-month period (June–October 2020) from our clinical pulmonary function laboratory at Austin Health, Victoria, Australia, were included for analysis. For each result, predicted values and LLN were calculated using the original and corrected GLI reference equations. Bland–Altman plots [14] were used to assess agreement between equations with results reported as median (5th, 95th percentiles). Changes in test interpretation were reported, defined as instances where haemoglobin corrected TLCO changed from either above to below the LLN, or below to above the LLN. As the error in the GLI TLCO reference equations was first noted in those with low TLCO values [13], we also reported changes in severity category in those with TLCO below the LLN, where we considered a measured TLCO of >60% predicted as a mildly reduced TLCO, 40–60% as a moderate reduction, and <40% as a severe reduction [15]. Additionally, we also assessed changes in clinical trial eligibility based on a threshold of TLCO ≥30% predicted [11].
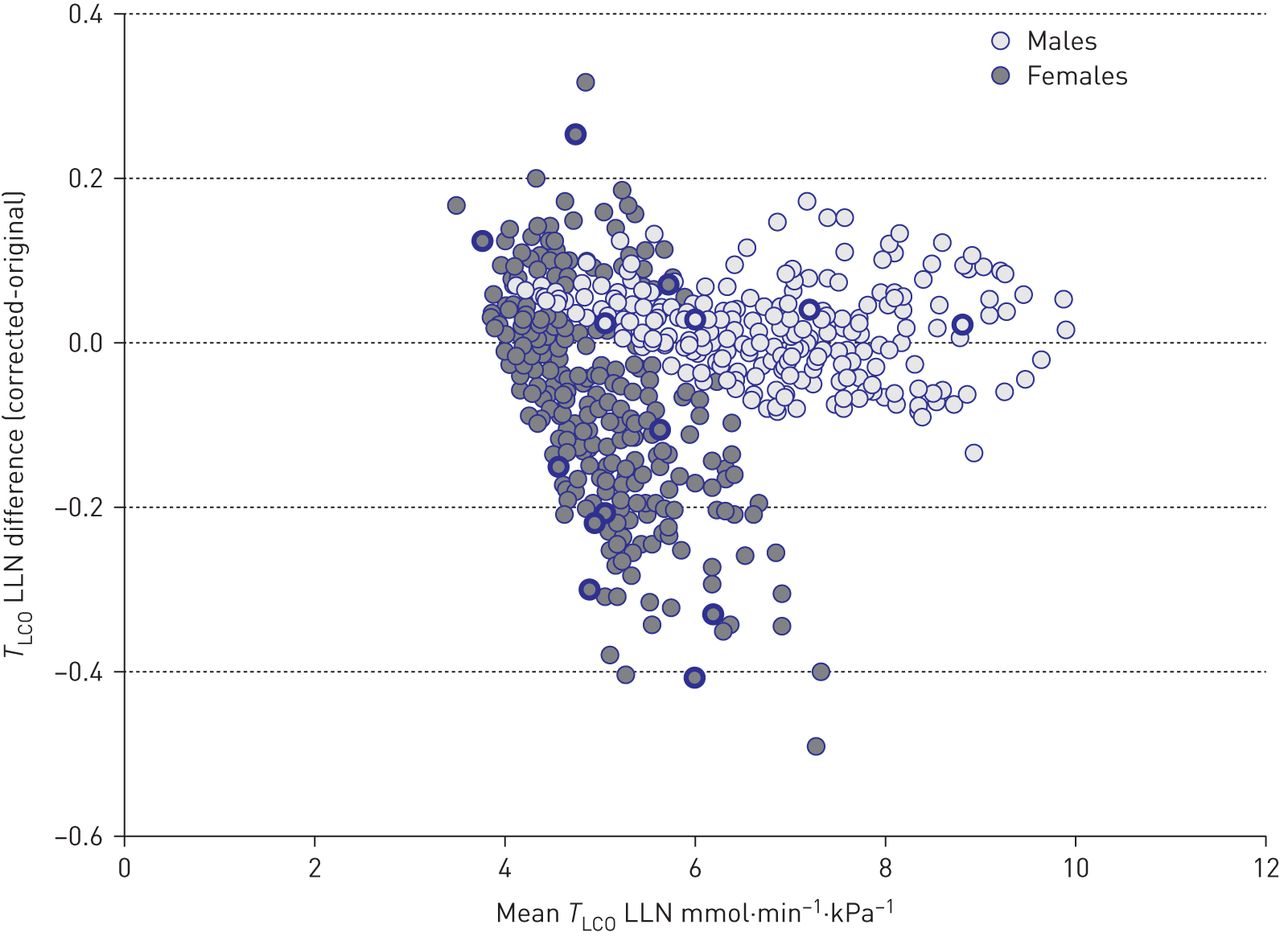
Our analysis included 864 TLCO results (42% female; age 64 years (33, 84 years); height 168 cm (152, 194 cm); body mass index 28.3 kg·m−2 (20.4, 42.6 kg·m−2); TLCO 6.21 mmol·min−1·kPa−1 (3.10, 11.14 mmol·min−1·kPa−1); forced expiratory volume in 1 s (n=833) 85% pred (43, 120% pred); largest of forced vital capacity/vital capacity (n=837) 94% pred (54, 127% pred); forced expiratory ratio 0.73 (0.44, 0.86)). The median change in predicted values for females was −0.10 mmol·min−1·kPa−1 (−0.44, 0.11 mmol·min−1·kPa−1), equating to −1.6% (−5.4, 1.9%), and for males was 0.02 mmol·min−1·kPa−1 (−0.08, 0.10 mmol·min−1·kPa−1), equating to 0.3% (−0.8, 1.4%). The median change in LLN for females was −0.05 mmol·min−1·kPa−1 (−0.29, 0.12 mmol·min−1·kPa−1), equating to −1.0% (−5.0, 2.7%) and for males was 0.01 mmol·min−1·kPa−1 (−0.06, 0.08 mmol·min−1·kPa−1), equating to 0.2% (−0.8, 1.3%). Bland–Altman plots showed that larger reductions in TLCO LLN were generally observed in females with larger TLCO LLN values (figure 1), but this was not the case for males. With regard to test interpretation, only females changed classification from abnormal to normal (n=7/367; 2%), whereas males (n=4/497, 1%) and females (n=3/367, 1%) changed classification from normal to abnormal to a similar degree (figure 1). Of note, all interpretation changes in males were in individuals that had small differences between the two LLN calculations, suggesting that they were already very close to the LLN, and therefore the change is less likely to influence clinical management. In terms of severity change for a reduced TLCO, only one of 72 (1%) females changed from a mild to moderate, whereas two of 50 (4%) females and one of 89 (1%) males changed from moderate to mild. There were no other severity category changes. Additionally, there were no changes in clinical trial eligibility; the same six patients had a TLCO below 30% predicted using both equations.

{kind=link}
Bland–Altman plot showing carbon monoxide transfer factor (TLCO) lower limit of normal (LLN) difference between corrected and original TLCO equations for each individual (n=864). Dark symbols represent females (n=367) and light symbols represent males (n=497). Individuals with altered interpretation of TLCO results, based on being above or below the LLN, are highlighted with bold symbol borders.
There are some inherent limitations to our analysis. In particular, our analysis involves data from a single centre and so it is possible that results could differ depending on the patient population. Additionally, the analysis was conducted during a period where our laboratory testing was impacted by the coronavirus disease 2019 pandemic and so the sample is likely to include a higher proportion of individuals for whom testing was considered clinically essential for patient management, compared to our usual patient cohort. Nevertheless, our laboratory is situated in a large metropolitan, university-affiliated, teaching hospital and is involved in the management of a broad range of respiratory diseases, which is likely to improve the generalisability of our findings. One must also recognise that patient management decisions are not only based on test results and hard LLN cut-off points for test interpretation; however, the LLN underpins interpretative strategies [15] and so is important in describing likely effects of reference equation changes.
Our analysis of a clinical dataset shows that adoption of corrected GLI TLCO reference equations effects females more than males, in that: 1) there was a small median reduction in predicted values and LLN for females, with minimal changes observed for males; 2) there were wider limits of agreement for females, so that it is also more likely that larger differences will be encountered, particularly for those with a larger calculated LLN, compared to males; and 3) there was a larger number of changes in test interpretation and severity grading for females. However, as the total number of changes in test interpretation and severity grading were small, and there were no changes in clinical trial eligibility, there is likely to be minimal impact on patient management overall.
Shareable PDF
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-04459-2020.Shareable
Footnotes
Conflict of Interest: W.R. Ruehland has nothing to disclose.
Conflict of Interest: C.J. Lanteri has nothing to disclose.
Conflict of Interest: P. Matsas has nothing to disclose.
Conflict of Interest: D.J. Brazzale has nothing to disclose.
- Received December 9, 2020.
- Accepted February 4, 2021.
- Copyright ©The authors 2021. For reproduction rights and permissions contact permissions{at}ersnet.org
References










