





Abstract
This retrospective cohort study showed that both persistent postoperative pulmonary hypertension and systemic inflammation were associated with previous exposure to air pollutants in CTEPH patients https://bit.ly/39tUy2l
To the Editor:
Chronic thromboembolic pulmonary hypertension (CTEPH) is a life-threatening condition and a rare complication of pulmonary embolism [1]. It is characterised by increased pulmonary vascular resistance (PVR), due to unresolved fibro-thrombotic material obstructing large pulmonary arteries, and secondary microvasculopathy. Various factors are suspected to be involved in the pathogenesis and progression of CTEPH, including inflammatory thrombosis, dysregulated fibrinolysis and deficient angiogenesis [2]. The gold standard therapy is a surgical approach, namely pulmonary endarterectomy (PEA), consisting of removal of obstructing fibro-thrombotic material. Although long-term exposure to air pollution might influence several factors potentially contributing to the pathogenesis of CTEPH, including pulmonary and systemic inflammation, pro-thrombotic changes, oxidative stress, endothelial dysfunction and vasoconstriction [3, 4], no study so far has investigated the relationship between air pollution and CTEPH. Interestingly, epidemiological and translational data supports the plausibility of a link between air pollution exposure, right ventricle failure and pulmonary hypertension (PH) [5–7]. Moreover, exposure to traffic-related air pollution was recently demonstrated to be associated with disease severity and impaired survival in pulmonary arterial hypertension (PAH), characterised by progressive occlusion of precapillary arteries [8]. Eventually, a potential role of air pollution as a risk factor for developing venous thromboembolism has been suggested [9]. We consequently hypothesised that exposure to common air pollutants, including particles with an aerodynamic diameter less than 2.5 or 10 µm (PM2.5, PM10), nitrogen dioxide (NO2), black carbon (BC) and traffic-related air pollution, could influence the progression of CTEPH and interfere with disease outcomes.
Thus, we investigated the association between exposure to residential air pollution and clinical parameters related to prognosis, pathophysiology, progression and survival in a cohort of CTEPH patients. Clinical parameters included predictors of mortality at diagnosis (New York Heart Association functional class (NYHA FC), 6-min walk distance (6MWD); haemodynamic parameters: right atrial pressure, mean pulmonary arterial pressure (mPAP), cardiac index and PVR; and these prognosticators combined in the European Society of Cardiology/European Respiratory Society risk score); the systemic inflammatory mediator circulating levels of C-reactive protein (CRP) at diagnosis; eligibility for PEA; persistent post-operative PH; occurrence of a PH-related hospitalisation; start of parenteral prostanoid treatment; lung transplantation; and death. Death was assessed separately for PEA-related in-hospital mortality, post-hospital discharge mortality (operated patients), and all-cause mortality (not operated and all patients). Eligibility for PEA was based on consensus by a multidisciplinary CTEPH team. Persistent post-operative PH was defined by a mPAP ≥38 mmHg and PVR ≥425 dyn·s·cm−5 measured 6 months after PEA, previously shown to affect long-term survival [10]. All adult patients with a haemodynamically proven diagnosis of CTEPH between January 1995 and September 2018 (n=335) and long-term follow-up (at least two follow-up visits after diagnosis) at University Hospitals of Leuven (median follow-up: 3.7 years) were included. To assess exposure to air pollution, each residential address at the baseline visit was geocoded and annual average exposure to PM2.5, PM10, NO2 and BC (year 2015), estimated with land-use regression models, was assigned to each address. In fact, three separate studies have demonstrated that the distribution of particulate air pollution is stable over a decade and that existing land-use regression models are good predictors of historical spatial contrasts [11–13]. In our cohort, data from hospital files revealed that only 19% of patients moved between diagnosis and data extraction. A sensitivity analysis, including exposure levels at the new address of patients who moved, showed similar significant associations. In addition, traffic-related air pollution was characterised by calculating the residence distance to major roads, defined as highways, national roads or large local roads, with a precision of at least 5 m. All analyses were performed with Geographic Information System (ArcGIS 10) software. To examine the association between residential air pollution and clinical parameters, we used multivariate logistic regression modelling for binary dependent health parameters, including eligibility for PEA and persistent PH after PEA, and independent air pollution parameters. Multivariate linear regression was used for continuous dependent parameters such as 6MWD, haemodynamic parameters and CRP levels. Multivariate Cox regression was applied to model end-points related to disease progression and survival, PH-related hospitalisation, start of parenteral prostanoid treatment, transplantation and mortality. The survival curve was performed using Kaplan–Meier survival function. We adjusted for age, gender, body mass index, smoking habits and level of obtained education. Additional adjustment for lung function parameters or treatment with parenteral prostanoid did not modify our results. In addition, patient population was stratified by age (younger than 65 years, or 65 years and older at diagnosis).
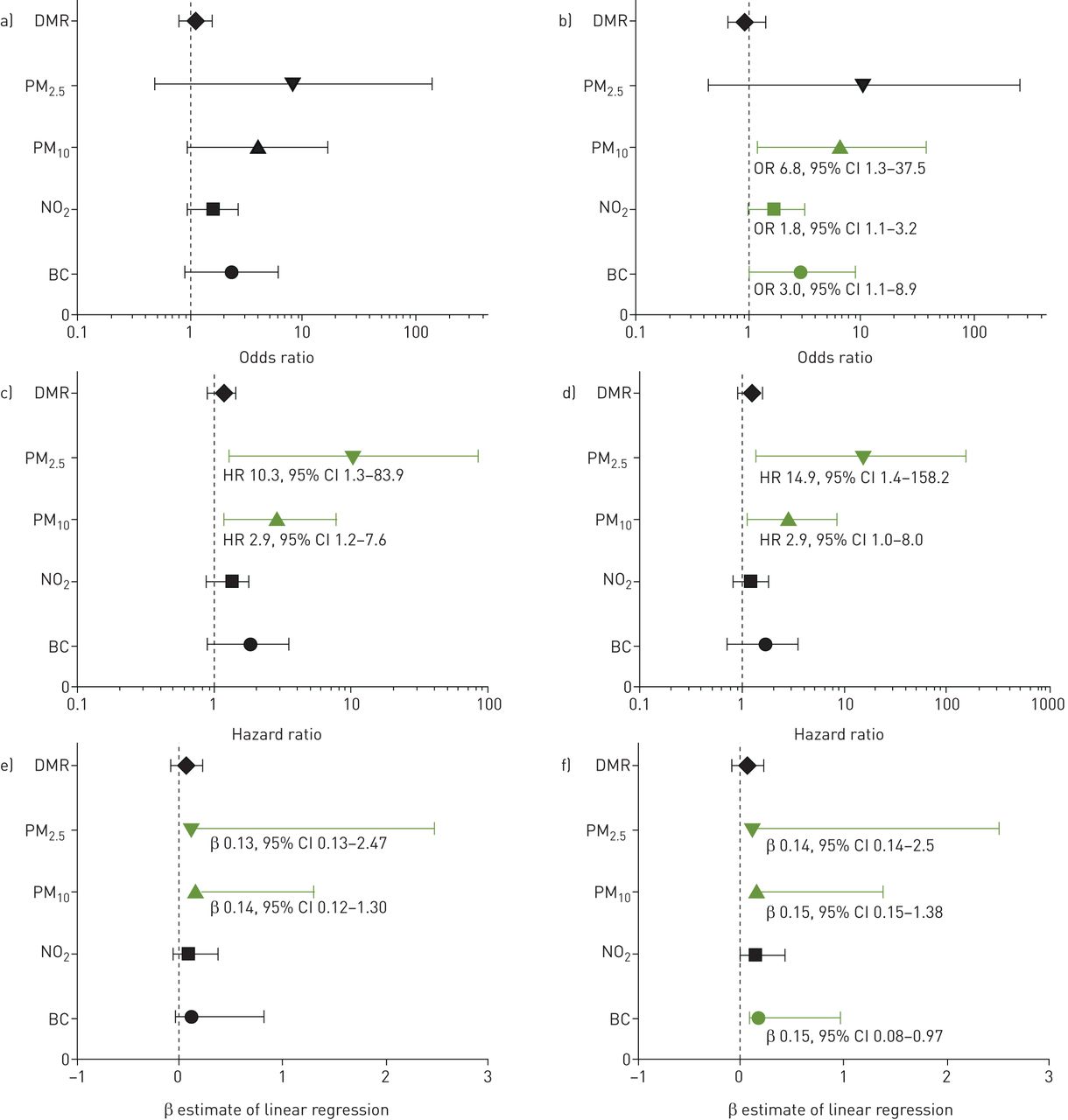
A total of 335 CTEPH patients (58% female) were studied with median age of 65 years (range 23–92 years). Patients displayed a severe haemodynamic profile (mean±sd cardiac index 2.2±0.6 L·min−1·m−2 and PVR 815±423 dyn·s·cm−5) and reduced exercise capacity (62% NYHA FC III–IV; 6MWD 330±203 m). 37% of the population died, with a 3-year survival of 84% (95% CI 79–88%). 66% of the patients were eligible for surgery and persistent post-operative PH was observed in 24% of the 151 operated patients who had an invasive haemodynamic evaluation 6 months after surgery. 15 of the operated patients died before the invasive haemodynamic evaluation for persistent post-operative PH, 6 months after PEA. Eight (53%) of them had a PVR higher than 500 dyn·s·cm−5 in the intensive care unit. Median (interquartile range (IQR)) concentration of residential PM2.5, PM10, NO2 and BC was 12 (2), 19 (3), 18 (9) and 1 (0.4) µg·m−3, respectively, in the total cohort. The median distance to major road was 637 m (IQR 1198 m). There were no differences in median (IQR) exposure levels of residential PM2.5, PM10, NO2, BC and distance to major road in patients with persistent post-operative PH compared with patients without persistent post-operative PH; 13 (1) versus 12 (2) µg·m−3; 20 (3) versus 19 (3) µg·m−3; 22 (14) versus 19 (9) µg·m−3; 1 (0.7) versus 1 (0.4) µg·m−3; 773 (1250) versus 607 (878) m, respectively. However, exposure to PM10, NO2 and BC was significantly associated with increased occurrence of persistent post-operative PH in the adjusted model (figure 1b). Inclusion of the early deceased patients with post-operative PH confirmed that post-operative PH is related to air pollution, except for BC. In the group of patients older than 65 years, we also observed a significant association of all-cause mortality with PM2.5 and PM10 both in crude and adjusted models (figure 1c and d). In addition, we identified a significant association between circulating CRP at diagnosis and PM2.5, PM10 and BC (figure 1e and f). Unfortunately, we were not able to find any statistically significant association between other clinical parameters and exposure to ambient air pollution.

{kind=link}
Association of post-operative pulmonary hypertension (PH) and C-reactive protein (CRP) with residential air pollution and distance to major road (DMR) in chronic thromboembolic pulmonary hypertension (CTEPH) patients. a) Crude and b) adjusted odds ratios for post-operative pulmonary hypertension and air pollutants and DMR in CTEPH patients (n=151). c) Crude and d) adjusted hazard ratios for all-cause mortality in CTEPH patients older than 65 years (n=165). Associations are adjusted for age, gender, body mass index (BMI), smoking and level of obtained education. Results are expressed as odds/hazard ratios with 95% confidence intervals per increase of 10 µg·m−3 for PM2.5 (particulate matter with diameter ≤2.5 µm), PM10 (particulate matter with diameter ≤10 µm) and nitrogen dioxide (NO2), per increase of 1 µg·m−3 for black carbon (BC) and per interquartile range increase (1198 m) for DMR. e) Crude and f) adjusted association of circulating CRP levels with air pollutants and DMR in CTEPH patients (n=258). Values are transformed to natural logarithms to reduce skewness. Associations are adjusted for age, gender, BMI, smoking and level of obtained education. Results are expressed as estimate of linear regression β with 95% confidence interval per increase of 10 µg·m−3 for PM2.5, PM10 and NO2, per increase of 1 µg·m−3 for BC and per interquartile range increase (1198 m) for DMR.
To our knowledge, this is the first study reporting an association between exposure to air pollution and outcome in CTEPH patients, namely post-surgery persistent PH in operated patients and all-cause mortality in patients older than 65 years. A mPAP ≥38 mmHg and a PVR ≥425 dyn·s·cm−5 was associated with increased in-hospital death and decreased quality of life in a large UK cohort [10]. According to expert opinion, it can be ascribed to incomplete endarterectomy, to limited operable proximal vessel chronic thromboembolic disease or to secondary microvasculopathy, resembling that observed in PAH [2, 14]. Given the limited pre-clinical findings and the wide confidence intervals, these associations should be cautiously interpreted. However, considering that exposure to air pollution was recently suggested to contribute to pulmonary microvascular remodelling in PAH [6–8] and the potential particulate matter effects on endothelial dysfunction [15], we may speculate that air pollution could also influence/exacerbate microvasculopathy in CTEPH. Besides, enhanced susceptibility to pollution may explain the exacerbated association between mortality and air pollution exposure in older patients [4].
In addition, we showed that air pollution was significantly associated with elevated circulating CRP levels at diagnosis, consistent with previous observations in other chronic respiratory and cardiovascular conditions, and therefore to be expected [4, 16]. However, this sounds relevant since there is accumulating evidence supporting the involvement of inflammation in the pathogenesis of CTEPH [17]. Interestingly, we previously showed that CRP-mediated inflammation contributes to the pathogenesis of CTEPH [18] and that levels of circulating CRP are elevated in patients with CTEPH compared with healthy controls, with a significant decrease after successful PEA along with improved haemodynamic profile and exercise capacity [19]. In the present study, CRP levels were also correlated with all-cause mortality (R=0.24; p<0.001). Exposure to air pollution resulting in systemic inflammation may enhance susceptibility among subjects with CTEPH, suggesting a potential role of air pollution in the progression of CTEPH. Further studies are required to explore whether these findings are related to exacerbated inflammatory-mediated microvasculopathy.
Limitations of this study are that exposure estimation according to residential address does not consider individual differences in the time spent at home, work or other environments, although CTEPH patients may spend more time at home than the general population. Finally, as multiple comparisons increase the possibility for type I error in statistical analyses, we cannot exclude any false-positive finding, although Bonferroni corrections were applied. Considering these limitations, multicentric studies including larger cohorts of patients need to be carried out to confirm our current findings. The strengths of our study include the relatively large CTEPH sample from a single centre, representative for the Belgian CTEPH population and the use of valid outcome measures according to PH guidelines.
In conclusion, this study provides new insights into the effects of air pollution in CTEPH. Our findings suggest that previous exposure to air pollutants is associated with persistent post-operative PH in CTEPH patients. In addition, we showed that increased circulating CRP levels at diagnosis are significantly associated with past exposure to air pollutants and with all-cause mortality of CTEPH patients.
Shareable PDF
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-02680-2020.Shareable
Acknowledgements
The University Hospitals of Leuven is member of the European Reference Network for rare lung diseases (ERN-LUNG). The authors would like to thank the Belgian Association of Patients for Pulmonary Hypertension (Belgische Pulmonale Hypertensie Patiëntenvereniging) for its support.
Footnotes
Conflict of interest: K. Swinnen has nothing to disclose.
Conflict of interest: E. Bijnens has nothing to disclose.
Conflict of interest: L. Casas reports grants from Research Foundation Flanders (FWO; a post-doctoral fellowship, grant number 12I1517N), outside the submitted work.
Conflict of interest: T.S. Nawrot has nothing to disclose.
Conflict of interest: M. Delcroix reports grants and personal fees for investigation work, lectures and consultancy from Actelion/J&J, personal fees for investigation work, lectures and consultancy from Bayer, personal fees for lectures and consultancy from MSD, personal fees for investigation work from Reata, personal fees for investigation work and consultancy from Bellerophon, personal fees for consultancy from Acceleron, outside the submitted work.
Conflict of interest: R. Quarck has nothing to disclose.
Conflict of interest: C. Belge reports personal fees from Actelion/Janssen and MSD/Bayer, outside the submitted work.
- Received April 7, 2020.
- Accepted January 2, 2021.
- Copyright ©The authors 2021. For reproduction rights and permissions contact permissions{at}ersnet.org
References










