





Abstract
Thoracic ultrasound is increasingly considered to be an essential tool for the pulmonologist. It is used in diverse clinical scenarios, including as an adjunct to clinical decision making for diagnosis, a real-time guide to procedures and a predictor or measurement of treatment response. The aim of this European Respiratory Society task force was to produce a statement on thoracic ultrasound for pulmonologists using thoracic ultrasound within the field of respiratory medicine. The multidisciplinary panel performed a review of the literature, addressing major areas of thoracic ultrasound practice and application. The selected major areas include equipment and technique, assessment of the chest wall, parietal pleura, pleural effusion, pneumothorax, interstitial syndrome, lung consolidation, diaphragm assessment, intervention guidance, training and the patient perspective. Despite the growing evidence supporting the use of thoracic ultrasound, the published literature still contains a paucity of data in some important fields. Key research questions for each of the major areas were identified, which serve to facilitate future multicentre collaborations and research to further consolidate an evidence-based use of thoracic ultrasound, for the benefit of the many patients being exposed to clinicians using thoracic ultrasound.
Abstract
Continued clinical use and research has established thoracic ultrasound as a key tool and skill for the modern pulmonologist https://bit.ly/3cCL6KS
Introduction
Thoracic ultrasound (TUS) is increasingly considered an essential tool for the pulmonologist [1–3]. Although this technique was for many years considered “of no use” in the lung, many decades of research have demonstrated high clinical utility in a number of areas of pulmonary disease. While the technique of TUS originated with radiologists, it is increasingly being used by pulmonologists “at the bedside”, and in this context is used with several potential aims. These include as an adjunct to clinical decision making for diagnosis, as a real-time guide to procedures and as a predictor or measurement of treatment response [1, 2, 4–6].
This European Respiratory Society (ERS) statement has been written in light of the growing evidence behind the use of TUS across a broad range of respiratory disease areas, as a summary of the evidence to clinicians who wish to understand the current rationale and state of the art of this technique. An evidence-based approach has been used throughout, addressing major areas of TUS practice and application. These include sections on required equipment and technique, assessment of the chest wall, parietal pleura, pleural effusion, pneumothorax, the utility of ultrasound in diffuse lung parenchymal diseases, diaphragm assessment, intervention guidance and suitable training in TUS.
We have highlighted areas of potential future research, as suggested by the current state of the evidence, at the end of each topic, and hope that this will lead to further definitive studies that will further improve our diagnostic and treatment armamentarium and benefit our patients.
Methods
The task force was comprised of clinicians with internationally recognised expertise in TUS. In order to reflect the multidisciplinary use of TUS, the expert group included pulmonologists and relevant experts from other specialties (e.g. radiology, emergency medicine, intensive care, thoracic surgery, paediatrics). This group was supplemented with young ERS members with TUS experience, and representatives of the European Lung Foundation (ELF). An ERS methodologist provided feedback on research strategy, evidence and statement synthesis, and oversight of the task force process.
The task force was initiated in December 2018 and comprised one face-to-face meeting, regular telephone conferences and e-mail correspondence. Initially, the task force established the overall scope and aim of the statement. It was agreed to limit the statement to the general use of TUS in the context of the clinical use by a pulmonologist. The members then agreed on a list of core topics to be addressed in the final statement.
A group of task force members with a designated topic leader was assigned to each topic and was responsible for development of a search strategy, evidence synthesis, and writing of an initial topic section for the statement. MEDLINE and Scopus databases were used for the literature searches, with inclusion of additional studies identified by individual task force members. An ELF representative was assigned to the write a section on the topic “patient perspectives”. The search terms for each topic are provided in the supplementary material. The topic leader identified and used relevant studies and knowledge of current clinical practice to make an initial topic draft, which the topic group then reviewed until a proposed final topic section had been completed. In addition to evidence synthesis, each group was given the task of identifying major gaps in the current evidence and provide key areas for future TUS research. The findings from the literature regarding the patient perspectives topic were shared with patients who had experience of TUS to identify additional perspectives.
Using the proposed topic sections, the task force chairmen composed a first draft of the statement manuscript. Task force members then provided comments and suggestions in the making of the final manuscript based on the draft. The final version of the manuscript was reviewed and approved by all task force members. The statement provides an overview of the evidence and current clinical practice for general TUS performed by pulmonologists, but does not provide recommendations for clinical practice.
According to ERS policies, task force members disclosed potential conflict of interests at the beginning of the task force process and prior to the publication of the statement.
Results
Equipment and technique
Overview of the evidence and current practice
When compared to other forms of clinical ultrasound with an established clinical tradition or more narrow clinical indication, international consensus publications regarding the equipment and technique used for TUS are scarce [1, 3, 7]. The first international consensus paper on point-of-care lung ultrasound provides some essential basic definitions and terminology [1]. However, when compared to recommendations on point-of-care cardiac ultrasound, a general recommendation regarding equipment and technique is not provided [8]. This reflects current clinical practice, in which choice of TUS scanning protocol, equipment and technique varies between specialties and countries. Numerous different protocols, techniques and use of different equipment have been assessed and validated in prospective diagnostic accuracy studies [6, 9–29]. Studies directly assessing or comparing different TUS equipment or techniques are fairly limited. However, these studies have demonstrated that factors such as choice of ultrasound machine (e.g. high-end, hand-held), protocol, transducer and patient positioning have a potential clinical impact [30–39]. Even though studies have addressed important factors, it is not possible to derive a universal and evidence-based TUS approach for any given clinical scenario. Apart from the examination itself, the coronavirus disease 2019 (COVID-19) pandemic has increased awareness of ultrasound operators in ensuring necessary safety precautions, specifically regarding cleansing of equipment and appropriate infection control [40].
Conclusions
Many different approaches and techniques have been described and validated. Comparative studies directly comparing different TUS approaches are limited. Given the many clinical settings and indications, a one-size-fits-all TUS approach is not feasible or meaningful. There remains a need to reach consensus on a general TUS principles and to determine the optimal approach for more specific clinical problems or settings (table 1).
Recommendations for future research: equipment and technique
Chest wall and parietal pleura
Chest wall soft tissues
On TUS, the intercostal muscle and fascia are visualised as echogenic layers under the subcutaneous tissue (figure 1). TUS can be used to identify and characterise superficial chest wall lesions, although generally cross-sectional imaging modalities, such as computed tomography (CT) and magnetic resonance imaging are more accurate [41].

Normal findings and chest wall. a) Normal findings: the muscles, fascia and other soft tissues of the chest wall (CW) are located in the upper part of the image. The surfaces of the ribs (R) can be seen as two horizontal hyperechoic, white, lines with posterior “shadowing” (*). The pleural line (P) is located just below the ribs. The lung tissue is filled with air and can therefore not be seen; therefore, the area (“L”) which can be seen below the pleural line is not the lung tissue, but artefacts. b) V rib fracture: the surface of the rib (R) can be seen as a horizontal, hyperechoic white line. A rib fracture (F) is present. c) Subcutaneous emphysema: air in the chest wall is typically seen as hyperechoic lines or dots with posterior shadowing (*). When the air is placed along a fascia it can be mistaken for the pleural line. However, when compared to (a), the ribs cannot be visualised and the hyperechoic white line caused by the subcutaneous emphysema is much more superficially located (∼1 cm) than the pleural line seen in (a) (∼2.5 cm). d) Benign pleural tumour: a parietal pleural tumour (T) is present. It is seen as a hypoechoic, black, well demarcated structure located above the pleural line (P).
Visceral and parietal pleura
Below the intercostal muscle, the visceral and parietal pleura are visualised as an echogenic “pleural line” visible between and deep to the ribs (figure 1). In healthy individuals, the pleural line slides parallel to the chest wall during respiration generating a “sparkling” appearance (“lung sliding”) and may move in synchrony with cardiac pulsation (“lung pulse”). Lung sliding can be confirmed using M-mode, which gives a characteristic “seashore” sign [1].
Hypoechoic parietal pleural thickening may mimic a pleural effusion on ultrasound and use of colour Doppler may help to differentiate these conditions, with fluid showing disordered colour flow, unlike static, solid pleural thickening. Benign pleural tumours such as fibromas and lipoma are relatively rare, are usually round or ovoid in shape, hypoechoic and homogeneous and do not infiltrate surrounding structures (figure 1) [42]. Asbestos-related pleural plaques have a distinctive TUS appearance and are hypoechoic, elliptical and smoothly limited foci; if calcified, they produce prominent acoustic shadows [42].
Malignant pleural nodularity is a more common finding and can be seen as irregular, well-circumscribed, often heterogeneous lumps arising from the parietal pleura and distorting the normal contour of the visceral pleura. They may be associated with a pleural effusion or chest wall/rib invasion [43].
TUS has been evaluated in the identification of the presence and degree of chest wall invasion of intrathoracic malignancies, and in one study was shown to have a higher sensitivity than CT [44]. The absence of pleural motion next to a peripheral lung lesion may identify parietal pleural invasion, thus refining radiological staging. In one study, the use of qualitative and quantitative colour Doppler sonography was more sensitive and specific than CT for predicting chest wall invasion by lung tumours [45].
Ribs
The ribs are seen as superficial, curvilinear structures, which completely reflect the ultrasound wave, resulting in posterior acoustic shadowing (rib shadows) (figure 1). If an ultrasound probe is placed along the long axis of a rib, the cortex of the bone is visible as a static, bright, echogenic line. When a cortical fracture is present, this line is disrupted by a step or gap and reverberation echoes occur at the point of the fracture (known as the “lighthouse phenomenon”) (figure 1). Fractures may be associated with a visible haematoma, a reactive pleural effusion or subpleural parenchymal changes from lung contusion. A recent systematic review suggests that TUS is more sensitive than chest radiography in diagnosing rib fractures; however, it can be painful and time-consuming, may be technically challenging in obese patients and the first ribs and retroscapular areas are incompletely visible. TUS may have a useful role in assessing focal areas of rib pain [46].
Metastasis of disease to the ribs causes destruction of the bone cortex, resulting in an irregular cortical appearance and loss of the usual rib shadows. In this instance, the infiltrated bone structure may be more visible and appear hypoechoic and heterogenous [47].
Intercostal muscles
The intercostal muscles can be directly visualised between the ribs. Even though the role of TUS assessment of intercostal muscle function is yet to be established, studies have reported several possible clinical implications. In a study by Wallbridge et al. [48] muscle thickness and echogenicity was found to correlate with spirometry assessment of severity in patients with COPD. In addition, intercostal muscle assessment has been reported as a possible tool for assessing respiratory workload in mechanically ventilated patients and for predicting failure of spontaneous breathing trials after supported ventilation [49–51].
Intercostal vessels
Distal to the apex of the rib posteriorly, the intercostal vessels run in the subcostal groove, but their course may be tortuous, particularly in the elderly. Colour flow Doppler using a linear probe allows good visualisation of the vessels and in theory may reduce vascular injury during pleural intervention [52]. However, the technique is operator- and experience-dependent and its reliability and accuracy has been questioned.
Conclusions
TUS is a useful clinical tool for assessing the chest wall and parietal pleura. Further studies are required to ascertain its clinical utility and impact in specific clinical scenarios (table 2).
Recommendations for future research: chest wall and parietal pleura
Pleural effusion
TUS has been used to assess suspected pleural effusion for ≤40 years [53–55]. Recently, a desire for better identification, classification and quantification of pleural fluid, coupled with rapid improvements in technology, has driven the widespread adoption of TUS by many pulmonologists. Indeed, being able to locate fluid with ultrasound to guide intervention is now seen as a core skill for trainees [56].
Benefits of TUS over other modalities
Basic, grey-scale TUS can identify much smaller volumes of fluid in comparison to other modalities, particularly chest radiography [57, 58]. It can do so reliably (meta-analysis data suggests a sensitivity of 93% and specificity of 96%) [59] in real-time at the bedside, with very high spatial resolution. The addition of colour Doppler may enhance assessment and improve differentiation of fluid from pleural thickening [60, 61].
Point-of-care versus diagnostic imaging
TUS is most commonly used as a point-of-care test to guide intervention for pleural effusions, and there is strong evidence to suggest this improves safety and can guide management decisions [62–64]. With sufficient experience, more formal diagnostic imaging is possible. While the ultrasonographic appearance of the fluid in itself cannot be considered diagnostic of the underlying disease, other typical TUS findings may help support a diagnosis (e.g. irregular nodularity on the diaphragm in malignant pleural effusion) (figure 2) [65].
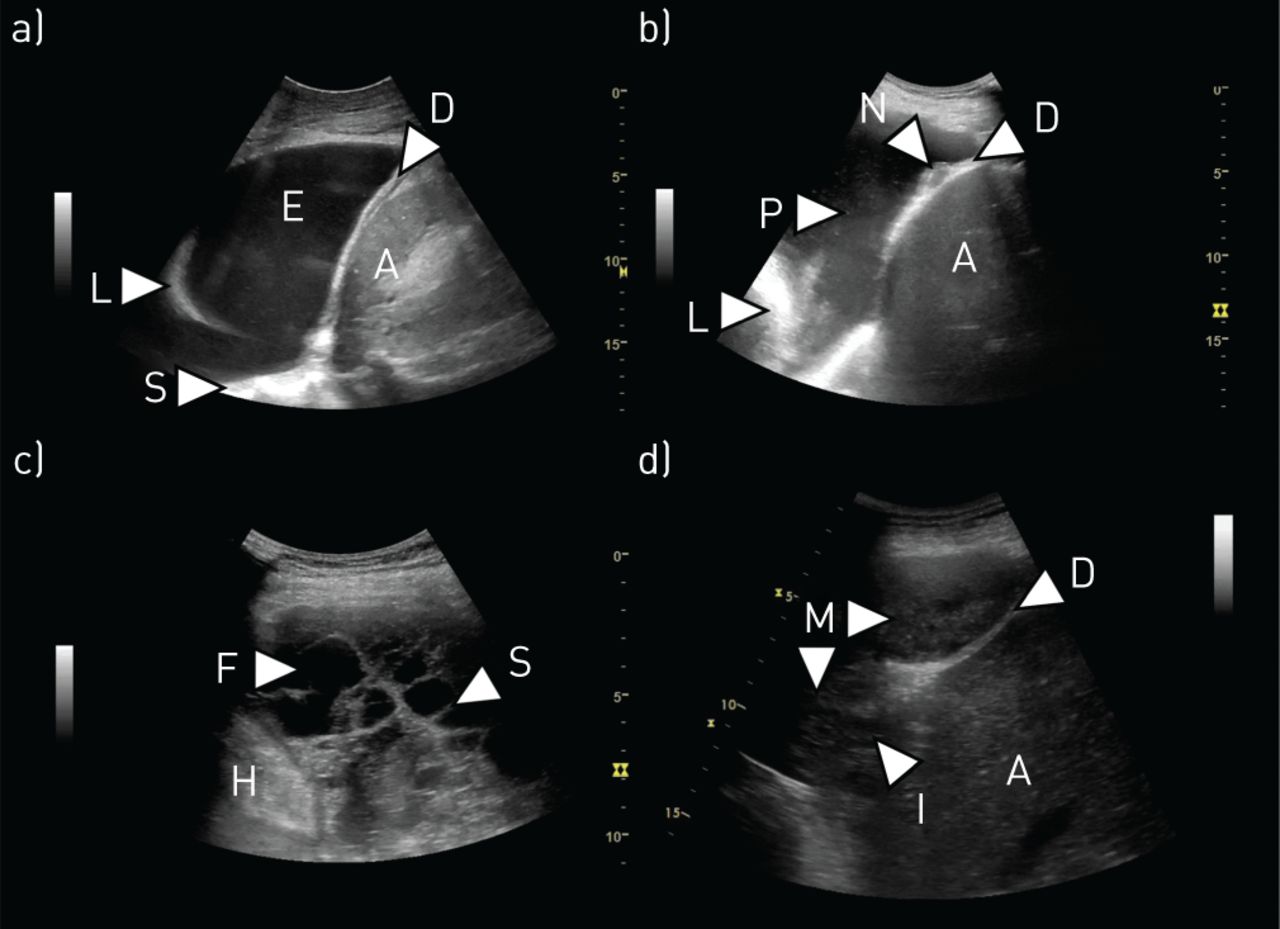
Pleural effusion and pleural malignancy. a) Simple pleural effusion: a simple, anechoic, pleural effusion (E) is present. There are no septations or visible structures floating within the effusion. The effusion can be used as an acoustic window to visualise underlying structures such as the lung (L), diaphragm (D) and thoracic spine (S). Abdominal structures such as the spleen (A) can be visualised below the diaphragm. b) Malignant pleural effusion: image from a patient with a malignant pleural effusion. A large nodule (N) is present on the diaphragm. Hyperechoic “plankton” (P) can be seen floating within the effusion. The compressed lung (L) and the liver (A) can also be seen. c) Complex septated pleural effusion: a complex septated pleural effusion is present, containing areas of anechoic fluid (F) as well as several septa (S). The heart (H) can be seen in the lower left side of the image. d) Malignant pleural mesothelioma: a large malignant pleural mesothelioma (M) is present and seen as a relatively homogeneous structure, resembling that of the liver (A) placed below the diaphragm (D). Invasive growth (I) through the diaphragm and into the liver is present.
Visualising fluid and estimating volume
Pleural effusions are most completely imaged with low-frequency ultrasound transducers, which allow for better understanding of fluid location and depth relative to deeper organs. Such frequencies are usually associated with curvilinear (typically 2–6 MHz) or sector (typically 1–3 MHz) probes [66]. Care must be taken with image processing settings, particularly gain, as these may adversely influence interpretation of fluid characteristics if incorrect [67]. The following four categories, described by Yang et al. [68], are commonly referred to when describing effusion appearance: anechoic, complex nonseptated, complex septated and homogeneous echogenic (figure 2).
Freely mobile fluid will often be most easy to scan with the probe placed on the posterior or lateral chest, with the patient sat upright to allow the effusion to pool inferiorly. In some circumstances, particularly in those who are recumbent on the intensive care unit, finding a suitable window may be more challenging.
Basic estimations of fluid volume may be useful when trying to quantify treatment effects of noninvasive therapy (such as diuretics for cardiac impairment) or when deciding whether to drain an effusion in a ventilated patient. Several simple equations have been devised to try and estimate fluid volume based on ultrasound appearances. Hassan et al. [69] tested the accuracy of five of these in 46 patients, and determined the most accurate to involve the total height of the effusion (H) in cm and the distance from bottom of the lung to apex of the diaphragm (C) in cm: This calculation was found to have an 83% accuracy when predicting fluid volume.
This calculation was found to have an 83% accuracy when predicting fluid volume.
Transudative disease versus exudative disease
Although not specific, presentation with bilateral effusions or associated ascites are strongly associated with transudates [70, 71]. Effusions due to transudative processes tend to have lower concentrations of complex molecules, particularly proteins. On TUS, this often makes the fluid appear anechoic (figure 2). However, this is not specific, with one series finding 14% of transudates to be echogenic [72]. By contrast, effusions which are exudates will almost always demonstrate echogenicity, complexity, or both [72–74]. There is a strong correlation between “swirling” and exudative processes, although again this is not a specific sign (figure 2) [75–77].
Features of malignant disease
There are no effusion features specific to malignant effusions, although many will show exudate characteristics and swirling is also frequently noted [74, 75]. Anechoic appearances have been described in ∼10% of cases [65]. Chronicity or more active malignancy may lead to the formation of fibrous septations and/or loculation [74]. The presence of an effusion in conjunction with pleural or diaphragmatic nodularity is almost always indicative of malignancy, although such signs may be subtle (figure 2) [65].
Features of pleural infection
Septation and/or loculation are suggestive of pleural infection requiring drainage in the appropriate clinical context (figure 2) [63], and may indicate a greater likelihood of failing fibrinolytic therapy [78]. One small series described the “suspended microbubble” sign and found it to be highly sensitive and specific for frank empyema [79]. In tuberculous effusions, complex septated appearances have a positive predictive value of 84% at 12 months for residual pleural thickening [80]. For “simple” parapneumonic effusions, no fluid signs are known to be associated with eventual need for treatment [81], but in a small paediatric series, a greater degree of echogenicity was associated with positive fluid culture, the need for more procedures, and longer duration of treatment [82].
Imaging atelectatic lung within fluid
The presence of even a relatively small effusion may cause compressive atelectasis, and this allows the nonaerated lung to be assessed by ultrasound [83]. Atelectatic segments have been described as resembling a “J” or a “hockey stick” (figure 2), and within them it may be possible to appreciate malignant lesions. In addition, there is evidence to suggest that M-mode measurements taken from the atelectatic lung may be predictive of nonexpandable lung [84].
Conclusions
The immediate and accurate identification of fluid prior to intervention remains the primary purpose of most TUS. Ongoing developments in technology, leading to even greater portability and higher resolution, is likely to improve our ability to identify and characterise effusions, especially at an early stage, as may the use of fluid contrast agents, which remains relatively rare (table 3).
Recommendations for future research: pleural effusion
Pneumothorax
Overview of the evidence and current practice
Pneumothorax has traditionally been identified on erect chest radiography. However, there has been increasing interest in the use of TUS in the identification of pneumothorax, particularly in the context of trauma and critical care [12]. The difficulty with TUS in pneumothorax is due to the high impedance of the tissue–air interface, causing most of the ultrasound waves to be reflected. Therefore, both air in the lung and air in the pleural space create a bright line at the pleural surface. However, there are three specific features of TUS described in pneumothorax: a lack of lung sliding, the absence of “B-lines”, and identification of a “lung point” [85–87].
Lung sliding is a sparkling of the pleural line as the lung moves with respiration [85]. If lung sliding is identified, then pneumothorax can be excluded in that area. Conversely, the absence of lung sliding is not specific for pneumothorax. Lung sliding can also be assessed using M-mode [88]. Lung sliding distal to the pleural line creates a granular pattern distal to the pleural line, referred to as the seashore sign. The absence of lung sliding creates lines known as the “bar-code” or “stratosphere” sign (figure 3). Importantly, loss of lung sliding can be caused by hyperinflation or bullous emphysema in COPD [89] and pleural adhesions.

Pneumothorax and B-lines. a) Normal M-mode findings: at the top of the image, the M-mode line can be seen as being placed vertically through the pleural line (P). In the corresponding M-mode image, the pleural line is seen as a hyperechoic line placed at the same distance from the transducer as can be seen in the two-dimensional (2D) image (∼1.8 cm). The nonmoving structures of the chest wall can in the M-mode image be seen as horizontal lines (Se) above the pleural line. In the presence of lung sliding, the area below the pleural line in the M-mode image will have a grainy appearance. The pattern has been described as resembling a seashore (Sh) and is therefore also known as the “seashore sign”. b) M-mode findings in pneumothorax: if lung sliding and lung pulse is absent, there will be no change in the area below the pleural line in the 2D/B-mode image. When using M-mode this will be seen as horizontal lines (St) being present above and below the pleural line (P). The M-mode pattern has been described as resembling a barcode or a stratosphere, and is therefore also known as “barcode sign” or “stratosphere sign”. The sign can be seen when a pneumothorax is present, but also in other conditions with absence of lung sliding and pulse (e.g. pleural adhesions). c) Multiple B-lines: multiple B-lines (B) can be seen as vertical, hyperechoic lines originating in the pleural line and stretching all the way from the pleural line to the bottom of the 2D/B-mode image. d) Idiopathic pulmonary fibrosis: thoracic ultrasound image of the lower lobe of a patient diagnosed with idiopathic pulmonary fibrosis. Multiple B-lines (B) are present and the pleural line (P) appears severely thickened and fragmented.
B-lines (otherwise known as “comet-tails”) are vertical artefacts projecting distally from the pleural line due to imperfections at the lung surface (figure 3) [86]. The presence of B-lines excludes pneumothorax, but their absence does not confirm it.
The lung point is an ultrasonographic sign which attempts to locate the junction between the pneumothorax and area with no air between the visceral and parietal pleural, i.e. where the visceral and parietal pleural part company [90]. With a stationary probe, the lung point refers to a pattern of repeated transitions between no lung sliding or B-lines (pneumothorax) into a demonstrable area of sliding (lung). It has been suggested that identification of the lung point is 100% specific for pneumothorax [90], and, by marking the lung point at multiple locations on the chest wall, this can be used to determine pneumothorax size [91]. However, a lung point is only seen in partial pneumothoraces and will be dependent on patient position.
TUS for pneumothorax can be challenging in small loculated pneumothoraces, and impossible in the context of significant subcutaneous emphysema where air in the subcutaneous tissue reflects all ultrasound waves (figure 1).
Studies have been published on the utility of TUS in pneumothorax diagnosis for >20 years. The majority of these have been prospective case series comparing imaging modalities in diagnosing pneumothorax in the context of trauma, iatrogenic (post-image guided biopsy) or in critical care, but no randomised controlled trials have assessed clinical effect or outcome. Currently, four meta-analyses have been published pooling data comparing the accuracy of TUS for pneumothorax compared to chest radiography [92–95]. Pooled sensitivity for TUS was 78–90% and pooled specificity was >98%. Chest radiography performed poorly, with a pooled sensitivity of 39–52%, but a similar specificity. However, these results must be taken in context; the vast majority of studies included mainly trauma patients lying in a supine position in the emergency department, which would naturally reduce the sensitivity of the chest radiography comparator.
There was significant heterogeneity among all four meta-analyses, with one meta-analysis suggesting it was due to operator performance [92], but a number of other factors could contribute. Importantly, pneumothoraces in trauma patients missed on supine chest radiography could have been occult. The diagnosis of occult pneumothorax has not been shown to impact clinical outcome and may indeed lead to over-treatment (e.g. pleural drainage may not be required).
The identification of pneumothorax post-lung biopsy was specifically assessed in three studies: Chung et al. [96] performed high-resolution CT (HRCT) scans on 97 patients after fluoroscopic-guided lung biopsy, identifying pneumothorax in 36%. The authors concluded a sensitivity of 80% for TUS, but did not discriminate the size of pneumothorax; thus, these studies are likely to be identifying a number of small, clinically insignificant pneumothoraces on CT (in keeping with the higher than usual pneumothorax rate). Reissig and Kroegel [97] studied 53 patients post-transbronchial biopsy during bronchoscopy, with TUS identifying pneumothorax in all four (7.5%) cases. Sartori et al. [98] also concluded that the sensitivity for TUS was 100% by examining 285 patients post-TUS guided lung biopsy. In this series only eight (2.8%) patients had pneumothorax, all of whom were identified by TUS; although CT was only performed when there was a discrepancy between TUS and chest radiography.
Another application of TUS could be in determining when pneumothoraces have resolved after chest tube drainage. One study suggested that TUS was superior to chest radiography [99], but was limited by being a single-centre study with small patient numbers (n=44).
Conclusions
The utility of TUS in diagnosing pneumothorax has been reported in many prospective case series, mostly in the context of trauma, iatrogenic (post-image guided biopsy) or in critical care. Four meta-analyses suggest that TUS has a better sensitivity for pneumothorax compared to chest radiography, but there are no randomised controlled trials assessing clinical effect or outcome, and the performance may be operator-dependent. The development of well-designed clinical trials will help to guide practice in the future (table 4).
Recommendations for future research: pneumothorax
Interstitial syndrome
Overview of the evidence and current practice
The interstitial syndrome describes a composite TUS finding that represents an increased density of the lung interstitium secondary to a diffuse underlying disease or condition [100, 101]. The space and tissues around the alveolar sacs compose the lung interstitium and includes the alveolar epithelium, pulmonary capillary endothelium, basement membrane, perivascular and perilymphatic tissues. If one or more of these tissues are affected in both lungs, interstitial syndrome may be present.
Presence and quantification of B-lines constitute the cornerstone finding when aiming to identify and confirm interstitial syndrome [102]. B-lines arise due to continuous reflection of the ultrasound beam between increased lung density areas and nonaerated areas near the pleural line [103, 104], and are defined as vertical reverberation artefacts originating from the pleural line in synchrony with lung sliding, extending uninterrupted to the edge of the screen without fading (figure 3) [105]. Several TUS scanning approaches involving a different number of scanning zones to detect interstitial syndrome have been recommended [5, 16, 17, 27, 106–110], but the majority are expansions of Volpicelli et al. [105] defining interstitial syndrome when at least three B-lines in more than two anterior or lateral lung interstitial spaces are present in each hemithorax. In many settings cardiogenic and noncardiogenic pulmonary oedema are the most common causative interstitial syndrome conditions, but other conditions, such as acute respiratory distress syndrome (ARDS) also cause interstitial syndrome [111]. In these conditions, interstitial syndrome arises due to hydrostasis or capillary leak with protein accumulation in the interstitium leading to interstitial and alveolar oedema [112]. A meta-analysis of 1827 patients found TUS to be more sensitive to detect interstitial syndrome in dyspnoeic patients with acute heart failure (AHF) than chest radiography (88% versus 73%), but with comparable specificities (90%) [113]. In a prospective multicentre study including 1005 patients attending the emergency department with acute dyspnoea, Pivetta et al. [114] found that adding TUS to a standard diagnostic regime was superior to detect interstitial syndrome as part of AHF. Two randomised clinical trials support these findings: Laursen et al. [5] compared usual clinical assessment and diagnostics with an approach using point-of-care ultrasound of the lung, heart and deep veins alongside usual clinical assessment and diagnostics. A significantly higher proportion received a correct diagnosis (88.0% versus 63.7%) and treatment (78.0% versus 56.7%) in the ultrasound group compared to the usual clinical assessment and diagnostics group. Pivetta et al. [115] demonstrated that an approach using TUS had a higher diagnostic accuracy than an approach using chest radiography and N-terminal pro-brain natriuretic peptide (area under the curve 0.95 versus 0.87, p<0.01) for the diagnosis of AHF. However, in the context of an intensive care setting, Bataille et al. [116] found that the presence of interstitial syndrome was poor in discriminating between cardiogenic pulmonary oedema and pneumonia, unless supplementary echocardiography was performed. Whether the results of the two trials can be generalised to other settings with more highly selected patients and whether TUS in the case of presence of interstitial syndrome should be routinely combined with echocardiography or focused cardiac ultrasound require further investigation.
In addition to interstitial syndrome, pleural oedema and the development of pleural fibrosis may occur in ARDS, giving rise to pleural irregularity and decreased lung sliding [23, 117]. However, extrapolation of data regarding diagnostic accuracy of interstitial syndrome detected in AHF may not necessarily be applied to interstitial syndrome in ARDS [118]. This also applies to patients undergoing dialysis, although a clear association between interstitial oedema identified by interstitial syndrome and fluid overload has been shown [119, 120]. Hence, besides its relevance as a diagnostic add-on modality in these “wet B-line” conditions, TUS shows operational applicability to monitor interstitial syndrome dynamics and guide treatment [121–124].
In interstitial lung diseases (ILDs), interstitial syndrome arises from ongoing inflammation or formation of fibrosis following collagen accumulation in the interstitium, resulting in distorted lung architecture with compromised alveolar aeration [104]. ILD represents a heterogeneous disease category involving idiopathic and connective tissue disease (CTD)-related subtypes [108, 125]. The applicability of TUS to detect interstitial syndrome based on the number of B-lines has primarily been assessed within CTD-ILDs secondary to scleroderma, rheumatoid arthritis, Sjogren's and antisynthethase syndromes [106, 107, 126, 127]. In several of these studies, an increased number of B-lines correlated with disease severity better than HRCT [108, 126]. Furthermore, the presence of pleural irregularity and increased distance between B-lines were associated with increasing fibrosis and reduced lung physiological parameters such as total lung capacity (TLC) and diffusion capacity of the lung for carbon monoxide (figure 3) [108]. Similar findings are observed in idiopathic ILDs [11]. A recent review proposed that TUS-identified interstitial syndrome can be used to determine the distribution of a usual interstitial pneumonia pattern when comparing to a HRCT [128]. Although some studies have observed high diagnostic accuracies of TUS-related interstitial syndrome in ILDs compared to HRCT [107], it is questionable whether these are representative due to small study cohorts, misclassification of disease and disease behaviour [129, 130].
The use of TUS for assessment of patients with COVID-19 has been reported in some initial studies following the outbreak of the pandemic. The typical pattern being reported as being presence of B-lines, interstitial syndrome and lung consolidation [131–133]. However, the currently published literature is still relatively scarce and further studies are urgently needed [40, 132].
Conclusions
The presence of interstitial syndrome is a dynamic surrogate marker of a disease or condition affecting the lung interstitium. As the genesis of interstitial syndrome does not clearly permit the differentiation between “wet” and “connective” B-lines, the role of TUS is as an integrated clinical add-on modality together with supplemental diagnostic work-up in order to determine an underlying diagnosis, it may also be used to monitor disease behaviour and treatment response. However, available knowledge on the validity of TUS to identify interstitial syndrome in selected disease categories is lacking. This warrants further prospective large-scale studies to determine diagnostic cut-off points for TUS-detected interstitial syndrome before clarifying its clinical use in controlled trials (table 5).
Recommendations for future research: interstitial syndrome
Lung consolidation
Overview of the evidence and current practice
The sonographic pattern of lung consolidation has been defined as a subpleural echo-poor region or one with tissue-like echotexture [1]. Animal and human studies have demonstrated that consolidation as it appears at TUS is the result of an increase in density of lung tissue, eventually resulting in complete de-aeration [24, 134]. This is the sole condition in which the lung can be visualised as a solid organ. Since many conditions (e.g. pneumonia, malignancy, pulmonary embolism, atelectasis, contusion, aspiration) may result in complete de-aeration of the lung tissue, lung consolidation is in itself a nonspecific finding. Lung consolidation should be differentiated from the presence of B-lines in which the density of the lung tissue is increased but the lung parenchyma remains at least partially aerated and therefore does not allow visualisation of the lung parenchyma.
In order to visualise lung consolidation by the use of TUS, the de-aerated lung area needs to be in contact with the chest wall (with or without interposition of fluid) in a “lung zone” which can be assessed transthoracically. Nonetheless, the diagnostic accuracy of TUS for lung consolidation has been shown to be higher than chest radiography when CT is used as the reference standard [135]. However, studies with more robust designs limiting potential biases are still warranted [136].
Studies assessing different aspects of using TUS for diagnosing pneumonia, especially community-acquired pneumonia, have been published since the 1980s, with a steady increase with the more widespread availability of point-of-care ultrasound [26, 137–145]. In a meta-analysis by Orso et al. [146] with a combined sample size of 5108 patients, the pooled diagnostic accuracy of TUS for diagnosing pneumonia in the emergency department was sensitivity 92% (95% CI 87–96%), specificity 94% (95% CI 87–97%) (figure 4). The use of TUS integrated with clinical assessment and other diagnostic modalities including chest radiography seems to increase the overall diagnostic accuracy, but little is known of the clinical impact of TUS for diagnosing pneumonia [5, 147, 148]. Based on a study by Jones et al. [149], it seems that TUS can safely replace chest radiography as the initial imaging modality of pneumonia in children and thus reduce radiation exposure. However, the study did report frequent use of chest radiography in the TUS group. Despite studies favouring the use of TUS over chest radiography for diagnosing pneumonia in adults, the optimal combination of TUS and chest radiography from a diagnostic and safety perspective has not been established. Several confounding factors in the intensive care setting make TUS diagnosis of pneumonia more complex, reducing the diagnostic accuracy; in this setting, conversely, a constellation of TUS additional signs and preliminary microbiological findings yields a high diagnostic accuracy [145].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Consolidation and invasive procedures. a) Pneumonia: a lung consolidation is present (C). Air bronchograms (A) are present and can be seen as hyperechoic dots or lines within the consolidation. The border zone (B) to the air-filled parts of the lung tissue appear serrated and irregular. B-lines can often be seen in the area surrounding the consolidation. The sonomorphology is typical for a pneumonia. b) Lung tumour: a lung tumour (T) is present and can be seen as a rounded, well demarcated structure with a fairly homogenous, tissue-like appearance. Invasive growth (I) into the chest wall is present. c) Ultrasound-guided biopsy of a pleural tumour: a pleural tumour (T) can be seen superficial to the pleural line (P). A needle (N) has been placed in the tumour in order to obtain a biopsy. The needle tip can be seen above the pleural line, minimising the risk of pneumothorax. d) Ultrasound guided biopsy of a lung tumour: a lung tumour (T) is present. A needle (N) has been placed in the tumour in order to obtain a biopsy. The needle tip has been placed in the margin of tumour, but still with some distance to the normal air-filled lung. This has been done in order to avoid obtaining a biopsy from central necrotic areas of the lung and yet still attempting to minimise the risk of pneumothorax.
Despite the fact that using TUS for the diagnosis of pulmonary embolism was described >50 years ago, research in the area has primarily evolved within the past two decades, with several descriptive and diagnostic accuracy studies [15, 29, 150–164]. In a meta-analysis of the diagnostic accuracy of TUS for pulmonary embolism, Squizzato et al. [165] reported a bivariate weighted mean sensitivity and specificity of 87.0% (95% CI 79.5–92.0%) and 81.8% (95% CI 71.0–89.3%), respectively. Based on these findings, TUS seems superior to other forms of mono-organ ultrasound for diagnosing pulmonary embolism [166, 167]. Several studies have advocated a whole-body-ultrasonography approach combining assessment of the lungs, heart and deep veins in patients with suspected pulmonary embolism or respiratory symptoms. This multi-organ approach is superior to what has been described using a mono-organ approach, but randomised trials assessing potential clinical impact and safety aspects are yet to be published [5, 22, 27, 29, 163, 168].
Several studies describing the use of TUS for assessing various other specific causes of lung consolidation (e.g. atelectasis, tumours, contusion) have been published. The findings and utility of TUS for assessing these conditions may be highly clinically relevant (e.g. assessment of invasive growth), but most of the studies are of a descriptive nature or have relatively small sample sizes (figure 4) [19, 44, 169–180].
While most of the previous research has aimed to assess the use of TUS as a diagnostic tool, increasing attention is being directed at its abilities as a monitoring tool [181]. The basic principles on how TUS can be used in real time to monitor a gradual change from normal pattern to interstitial syndrome, lung consolidation and subsequent reversal of these findings have been well described using a whole-lung lavage model [24]. Several TUS monitoring studies have reported promising and clinically relevant results, especially in the intensive care setting of ARDS, ventilator-associated pneumonia and weaning from mechanical ventilation. However, there is still a lack of robust data on TUS-oriented management in improving clinical outcomes [6, 110, 122, 138, 182–188].
Conclusions
Based on currently published studies, TUS has a role as a bedside tool for assessing patients with possible or known lung consolidation, and potentially as a monitoring tool. Future research should focus on the effect of TUS on clinically relevant outcomes and how TUS is ideally used alongside other diagnostic modalities (table 6).
Recommendations for future research: lung consolidation
Diaphragm
Overview of the evidence and current practice
Diaphragm mobility and thickness have been correlated with respiratory muscle strength and lung function in healthy subjects [189, 190]. In 27 patients with hemidiaphragm paralysis, diaphragm mobility during quiet breathing, thickness at functional residual capacity and TLC, and diaphragmatic thickening fraction (TF; diaphragmatic thickness variation during respiration) were decreased on the side of the hemidiaphragm paralysis when compared to the nonparalysed hemidiaphragm [191]. TUS was more sensitive than fluoroscopy to detect hemidiaphragm movement abnormalities, with four out of 30 technical failures for fluoroscopy and no failures for TUS [192]. Even though the diaphragm has traditionally been assessed using conventional B- or M-mode, a few studies have indicated that more advanced techniques (e.g. area method, speckle tracking) might prove more accurate and feasible [193–195].
TUS assessment of the diaphragm in the intensive care unit
Spontaneous breathing trials (SBT) are used to predict weaning outcomes in patients on mechanical ventilation; however, 13–26% of those extubated after successful SBT need rescue noninvasive ventilation or are re-intubated within 48–72 h [196, 197]. Ventilation-induced diaphragm dysfunction is often observed in patients who are difficult to wean off mechanical ventilation, and can be assessed using TUS by measuring diaphragm thickness at end expiration, or more dynamic evaluation of TF or diaphragm excursion (DE) at the zone of apposition of the pleural and peritoneal membranes. Data on TUS parameters and weaning are varied; in a systematic review including 19 studies and 1071 patients on invasive mechanical ventilation for ≤24 h, the area under the operating curve for TF was 0.87, with a pooled diagnostic odds ratio (dOR) 21 (95% CI 11–40), and pooled sensitivity for DE was 75%, dOR 10 (95% CI 4–24) [198]. Another meta-analysis (13 studies and 742 patients) reported pooled sensitivity of 90%, specificity 80% and dOR 32.5 (95% CI 18.6–56.8) for TF, and 80%, 70%, 10.6 (95% CI 4.2–27.1), respectively, for DE [199]. Low TF was a good predictor of weaning outcome with consistency across studies, and higher dOR suggests that TF has better diagnostic accuracy than DE. Both TF and DE are reproducible [196, 198, 200–204]. However, in a large multicentre randomised controlled trial by Vivier et al. [205], diaphragmatic dysfunction identified by TUS was not associated with an increased risk of extubation failure. Hence, further studies are needed to establish the exact role of TUS assessment of the diaphragm in mechanically ventilated patients.
Pleural effusion
The mechanism of breathlessness in pleural effusion is not fully understood. Pleural effusion adversely affects the diaphragm's ability to generate negative pressure, and this is postulated to be a cause of breathlessness. In 14 mechanical ventilation patients on pressure support ventilation with a pleural effusion, respiratory rate decreased, tidal volume increased and diaphragm displacement and thickening increased after pleural fluid aspiration, with correlation between volume of effusion drained and increase in tidal diaphragm thickening [206]. When TUS was performed before and after thoracoscopy (14 out of 19 malignant pleural effusions), larger effusion volumes were associated with impaired diaphragm movement compared to effusions with normal diaphragm movement [207]. After pleural aspiration, patients with paradoxical movement of the hemidiaphragm (n=21) had a small but significant improvement in forced expiratory volume in 1 s, forced vital capacity, arterial oxygen tension, alveolar–arterial oxygen gradient and dyspnoea, whereas those without paradoxical movement of the diaphragm (n=41) did not [208]. In a larger study (n=145) of patients with symptomatic pleural effusions, Muruganandan et al. [209] showed that TUS demonstrating abnormal hemidiaphragm shape and movement prior to thoracentesis were independently associated with relief of breathlessness post-drainage. These results suggest that diaphragm flattening or abnormal movement are strong indications for aspiration to restore normal diaphragm position and shape, and TUS can aid in this assessment.
Other
Diaphragm mobility has been shown to be decreased in COPD patients compared to healthy subjects. DE correlates with lung function [210, 211], and TF in acute exacerbations of COPD complicated by respiratory acidosis correlates with noninvasive ventilation failure, longer stay in the intensive care unit, prolonged mechanical ventilation, need for tracheotomy and mortality [212, 213]. TF predicted nocturnal hypoxaemia in COPD with mild or no daytime hypoxaemia [214].
A review of respiratory muscle imaging modalities in neuromuscular disorders (NMD) identified nine studies (n=292 patients) that used ultrasound [215]. Diaphragm thickness was significantly lower in patients with NMD than in healthy controls [216, 217], and in amyotrophic lateral sclerosis was positively correlated with vital capacity and negatively correlated with arterial carbon dioxide tension, with good interobserver reliability [218].
Conclusions
TUS assessment of the diaphragm has been assessed in various clinical settings. However, studies are mostly small observational studies, the findings of which are not yet well validated, and it is as yet unclear whether TUS findings can be translated to clinically meaningful outcomes. In addition, most studies are either done in healthy volunteers or in small highly selected populations. More data are needed from larger studies (table 7).
Recommendations for future research: diaphragm
Ultrasound-guided procedures
Overview of the evidence and current practice
The increased use of TUS has transformed the scope of procedures the interventional pulmonologist is able to offer. Studies have consistently demonstrated that TUS is safer than clinical examination in direct comparison [219], and reduces risk and cost of iatrogenic complications [220–222]. The current position of most international guidelines is that all pleural procedures (for fluid) should be performed under TUS guidance [3]. Clinical research has highlighted the diagnostic and therapeutic value of pleural interventions in improving key outcomes [223, 224], further challenging physicians to extend their procedural boundaries with the aid of TUS, to meet an increasing patient demand and improve accessibility.
As well as pre-procedure TUS guiding optimal pleural puncture site, real-time ultrasound imaging can facilitate thoracentesis of small effusions, where most experts suggest ≤1 cm depth is required to be safe [42]. In the setting of loculated effusions, the introducer needle of the aspiration catheter can be guided towards the largest collection of fluid, while being used to traverse and break-up septations along its course [225]. Post-procedure ultrasound can rule out pneumothorax with up to 100% negative predictive value [85]. The use of colour Doppler can screen for the intercostal artery at the site of intervention pre-procedure, as well as confirm absence of post-procedure haemorrhage [226, 227].
TUS provides similar procedural benefits in chest tube insertion. TUS is not currently recommended to guide drainage of pneumothorax. Currently used techniques for chest tube insertion are “Seldinger” (or guide-wire), blunt dissection and the trocar method. Most of the data suggests that 12-French (F) drain is an appropriate size for the majority of pleural drainage indications, providing a balance of safety, effectiveness and patient comfort [228, 229]. A retrospective analysis of the largest prospective randomised controlled trial of pleural infection to date (Multicenter Intrapleural Sepsis Trial-1; n=405) [230], showed that there was no significant difference in frequency of death or surgery in patients managed with small-bore (<15 F) chest tubes [229]. In addition, their suitability for intrapleural fibrinolysis makes them an appropriate treatment choice [231]. The optimal size of chest tube for pleurodesis is still an area of controversy, with some studies suggesting that small-bore (<14 F) drains may be less effective [232, 233]. Based on these studies, the pulmonologist will be able to handle the majority of indications for chest tube insertions by the use of TUS-guided insertion of small-bore chest tubes.
Indwelling pleural catheters (IPCs) have had a huge impact on the management of recurrent malignant pleural effusions [234], with ongoing studies looking to delineate their place in benign effusions. While TUS plays an established role in guiding initial insertion, it may potentially guide the selection of patients who may be more suitable for IPCs rather than drainage and pleurodesis. The identification of nonexpandable lung has been traditionally achieved through drainage of pleural fluid followed by a chest radiography demonstrating pneumothorax ex vacuo or using pleural manometry [235]. Data suggest that speckle tracking imaging analysis and M-mode can identify entrapped lung prior to effusion drainage, allowing upfront choice of definitive management option [84].
Local anaesthetic thoracoscopy (LAT) has now become the gold-standard investigation of an undiagnosed unilateral pleural effusion and/or suspected malignancy [236], with an increasing number of centres having routine access [237]. TUS is a vital accessory to LAT, allowing the operator to assess volume of fluid, presence/absence of lung sliding and degree of septation as well as characterising the nature of pleural and diaphragmatic thickening and nodularity. The operator is then able to target entry point for maximal success or conversion to an alternative intervention in the same visit, e.g. if effusion volume is deemed to be inadequate. In this circumstance, TUS can facilitate artificial pneumothorax-induction in suitable patients, using real-time introduction of a Boutin needle or blunt dissection [238, 239]. Another option in this setting, and increasingly conducted by physicians in recent years, is TUS-guided closed pleural biopsy (figure 4). This technique is particularly advantageous in the elderly or frail patient, as a less invasive alternative to LAT. In the hands of an experienced operator, TUS-guided pleural biopsy outcomes are comparable to those conducted by specialised colleagues in radiology [4]. To date, there is no robust evidence to determine whether newer core-cutting needles are superior to traditional reverse-bevel (e.g. Abrams) needles.
TUS-guided lung biopsy conducted by pulmonologists is not only safe and feasible with comparable yields [240, 241], but may also be advantageous over radiologist-led CT-guided biopsy due to shorter procedure times, quicker access and limited risk of complications [242–244] (figure 4). The supplementary use of more advanced ultrasound modalities such as contrast-enhanced ultrasound and elastography could have a role for selecting patients with a high risk of malignancy for subsequent biopsy and to guide the choice of biopsy site, thereby increasing the diagnostic yield of the biopsy procedure [245–249].
Focused ultrasound performed by pulmonologists of structures related to the chest (e.g. neck) and subsequent ultrasound-guided biopsy has been described and potentially provides a rapid, less invasive method for obtaining a diagnosis and staging patients with suspected thoracic malignancy [250–253]. In addition, a potential role has been described in other diseases with extrapulmonary involvement (e.g. sarcoidosis, tuberculosis) [254–256].
Conclusions
TUS is portable, cost-effective and adds diagnostic and therapeutic value in guiding pleural interventions. As an increasing number of practitioners continue to extend the scope and complexity of procedures they undertake, it is important to recognise limitations, both of operator and environment, and remain safe and evidence-based at all times (table 8).
Recommendations for future research: ultrasound-guided procedures
Training
Overview of the evidence and current practice
TUS has no direct complications or risks, but important decisions are made based on TUS and competent operators are essential to achieve a high diagnostic accuracy [97–258]. Structured and evidence-based training and assessment of new operators are necessary to ensure competence [2, 259]. A systematic review in training methods and assessment in TUS was published in 2018 with 16 included articles [259]. Since then, 12 articles have been published and were eligible for inclusion in this statement.
Procedural competence in TUS is often taught at the bedside, during rounds by an experienced colleague, or at courses with a fixed time frame [3, 260–263]. Unfortunately, the clinical setting can be an unsystematic and stressful environment, where learning is dependent on the simultaneous availability of suitable patients and skilled supervisors. Several TUS courses exist, but the fixed time frame makes it impossible to guarantee that all trainees reach competence in scanning a range of different pathologies. Additionally, implementation and integration of the technical procedure is just as important as learning the procedure itself, meaning that feedback and clinical discussions with other ultrasound operators are important.
Simulation or phantom-based training provides a stress-free and standardised learning environment where individual trainees can continue practicing their technical skills and hand–eye coordination until they have acquired necessary competencies [264, 265]. Trainees’ hands-on training time is maximised and the need for expert supervision is reduced, which can make simulation-based training more effective and economically advantageous [266].
Hands-on training, whether on simulators or by scanning simulated patients or healthy volunteers, must be based on solid theoretical knowledge to improve the efficacy of training and must be followed by supervised refinement of skills in the clinic until independent competency is acquired. A fixed time frame or an arbitrary number of performed/supervised procedures do not equal obtained competence; all trainees have different learning paces [267].
The European Federation of Societies for Ultrasound in Medicine and Biology and the Royal College of Radiologists have made recommendations about which topics to include in a theoretical curriculum (table 9) [262, 263]. Several studies assess new operators’ theoretical knowledge by using theoretical tests covering the same topics, or nearly the same topics [260, 268–270]. Many different learning methods have been used, e.g. classroom-based lectures, group sessions, web-based sessions or individual homework with books or papers [270–273]. All studies showed increased knowledge regardless of the learning method used, but only one study presented validity evidence for the theoretical test that was used [274].
Comparing the recommendations on theoretical knowledge needed for completion of level 1 practitioner in thoracic ultrasound by different organisations
Practical hands-on training was included in a majority of studies [260, 261, 269, 271–273, 275–279]. Several hands-on training modalities are represented and probably useful, including animal models, virtual reality simulators, phantoms and humans (healthy volunteers or patients with pulmonary disease/symptoms). However, the study designs and methods were heterogeneous; outcome measures without evidence of validity were used; and results were difficult to compare. Two studies have presented simulator models with validity evidence for practical assessment [280, 281]; several tools for assessment in a clinical setting were identified [282–284]; and a guide for a minimum training standard with both theoretical and practical training by experienced TUS operators is proposed [285].
Gaps in knowledge and/or evidence in training and assessing TUS
Just as physicians are expected to treat and practise according to best medical evidence, educators should use the best available evidence to guide their education in the best possible direction [286]. Geographical, financial and administrative aspects can affect the possibilities to educate on the highest possible level. No studies have assessed the effect of different hands-on training modalities, the educational intervention on an institutional level or used patient outcomes as a primary end-point. These studies are needed to propose recommendations on a European level.
Conclusion
A TUS curriculum should be well planned and evidence-based similar to the requirement for clinical practice. The ERS launched such a training programme in 2020. Heterogeneous caseload, scarcity of expert supervision and different learning paces are major challenges to education in a clinical setting. Suitable, objective assessments with solid evidence of validity are necessary to ensure competence at each step before independent practice moving towards competency-based training and entrusted professional activities (table 10).
Recommendations for future research: training
Patient perspectives
Overview of the evidence
The literature search could not identify any quantitative or qualitative studies specifically addressing this topic. Four articles were included for review addressing patient discomfort and satisfaction with ultrasound in emergency department settings, and included, but were not limited to TUS [287–290]. Key themes identified were high patient satisfaction, low levels of discomfort with bedside ultrasound and patient–provider interactions.
Patient satisfaction
Bedside ultrasound in the emergency department was found to increase patient satisfaction in two studies [287, 288]. Heating the ultrasound gel did not significantly increase patient satisfaction, overall satisfaction with the emergency department visit or patient perceptions of physician professionalism [290]. Patient feedback indicated that bedside scanning is also welcome outside the emergency setting, particularly if the patient is having trouble breathing as it avoids the additional strain of visiting multiple hospital departments. Patients may take comfort from understanding the lower risks of ultrasound when compared to other imaging techniques, such as CT. Exposure to radiation is of concern to patients, particularly if multiple scans are required over time.
Discomfort
The majority of patients do not experience discomfort during point-of-care ultrasound of the heart, lungs and deep veins [289]. An increased level of discomfort was most often due to an underlying condition (e.g. rib fracture) or the result of an intervention (e.g. resuscitation) causing localised pain. Most patients, including those who experience some discomfort, would be willing to accept ultrasound assessment in future. Before performing ultrasound, professionals should inform patients with an underlying condition that they may experience discomfort.
Patient–provider interactions
Bedside ultrasound may improve communication between patients and professionals by offering the chance to explain examination results and provide a clearer understanding of the patient's diagnosis [287, 288]. Professionals’ communication skills play a crucial role in patient experience of imaging. Professionals should be mindful of the language they use and avoid jargon when discussing the procedure and results.
Conclusions
TUS is acceptable to most patients in emergency department settings. Further qualitative studies are needed to fully understand patient experiences and preferences of TUS (table 11).
Recommendations for future research: patient perspectives
Overall conclusions
Continued clinical use and research has established TUS as a key tool and skill for the modern pulmonologist. The increased availability of ultrasound equipment has helped facilitate the implementation and use of TUS across Europe and worldwide. Since, historically, ultrasound examinations have been provided by other specialties, many of the national and international respiratory societies have no tradition or recommendations for the use of TUS. Therefore, in many ways the clinical use of TUS by pulmonologists is far ahead of the guidelines and recommendations. A potential advantage of TUS is the relatively short pathway from research to clinical implementation, with the major disadvantage being a general lack of consensus, and research results being implemented without sufficient scientific evidence to support such implementation. In order to achieve a further “professionalisation” of pulmonologists performing TUS, societal guidelines and recommendations from national and international respiratory societies are called for. The aim of this task force statement was to provide a state-of-the art summary guide for the pulmonologist of the current use of TUS and to identify key future research areas. This first official ERS statement on TUS is an important step to further advance professionalisation of TUS at an international level, which will in turn benefit the many patients being assessed by physicians in this way on a daily basis.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Appendix: Search terms used for each statement topic ERJ-01519-2020.SUPPLEMENT
Shareable PDF
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-01519-2020.Shareable
Acknowledgement
We thank David Rigau Comas (Iberoamerican Cochrane Center, Barcelona, Spain) for providing valuable methodological assistance and support during the making of the statement.
Footnotes
This article has supplementary material available from erj.ersjournals.com
This ERS statement was endorsed by the ERS Executive Committee on 2 September, 2020.
Conflict of interest: C.B. Laursen has nothing to disclose.
Conflict of interest: A. Clive has nothing to disclose.
Conflict of interest: R. Hallifax has nothing to disclose.
Conflict of interest: P.I. Pietersen has nothing to disclose.
Conflict of interest: R. Asciak has nothing to disclose.
Conflict of interest: J.R. Davidsen has nothing to disclose.
Conflict of interest: R. Bhatnagar has nothing to disclose.
Conflict of interest: E.O. Bedawi has nothing to disclose.
Conflict of interest: N. Jacobsen has nothing to disclose.
Conflict of interest: C. Coleman is an employee of the European Lung Foundation.
Conflict of interest: A. Edey has nothing to disclose.
Conflict of interest: G. Via has nothing to disclose.
Conflict of interest: G. Volpicelli has nothing to disclose.
Conflict of interest: G. Massard has nothing to disclose.
Conflict of interest: F. Raimondi has nothing to disclose.
Conflict of interest: M. Evison has nothing to disclose.
Conflict of interest: L. Konge has nothing to disclose.
Conflict of interest: J. Annema has nothing to disclose.
Conflict of interest: N.M. Rahman reports equipment provision from Esaote, Italy, outside the submitted work.
Conflict of interest: N. Maskell has nothing to disclose.
Support statement: This work was supported by the European Respiratory Society (grant: TF-2018-05). Funding information for this article has been deposited with the Crossref Funder Registry.
- Received May 1, 2020.
- Accepted August 20, 2020.
- Copyright ©ERS 2021
References










