





Abstract
To date, there are no network meta-analyses comparing the impact of as-needed treatments in asthma, including the single maintenance and reliever therapy (known as “SMART” or “MART”; for simplicity, SMART will be used hereafter) and the use of inhaled corticosteroid (ICS)/long-acting β2-agonist (LABA) combination exclusively on an as-needed basis. Therefore, we performed a systematic review and network meta-analysis concerning the efficacy and safety of SMART and as-needed therapies in asthma. Data from 32 096 asthmatic patients were extracted from 21 studies, lasting from 6 to 12 months. In adult mild-to-moderate asthmatic patients low-dose SMART and as-needed low-dose ICS/LABA combination were significantly (relative effect <0.78; p<0.05) more effective than the other as-needed therapies in reducing the risk of exacerbation, and both were ranked as the first treatment option reaching the first quartile of the surface under the cumulative ranking curve analysis (SUCRA). In adult moderate-to-severe asthmatic patients, low-dose to medium-dose SMART and high-dose ICS/LABA+as-needed short-acting β2-agonist were equally effective in reducing the risk of severe asthma exacerbation (p>0.05), although only low- to medium-dose SMART was ranked as the first treatment option (first SUCRA quartile). Overall, these treatments were well tolerated, and effective also on lung function and disease control. This study supports SMART and as-needed therapies as a suitable therapeutic option for asthma, by providing the most effective positioning of each specific treatment according to the disease severity.
Abstract
As-needed therapy represents a suitable therapeutic option in the treatment of asthma, with single maintenance and reliever therapy and as-needed ICS/LABA being the most effective therapeutic options https://bit.ly/3dEIXh4
Introduction
Since 2006, the Global Initiative for Asthma (GINA 2006) recommends a stepwise approach for the pharmacological management of asthma [1]. Accordingly with the GINA recommendations updated in 2020 [2], patients suffering from mild asthma should be controlled with Step 1 or 2 treatments, either with as-needed low-dose inhaled corticosteroid (ICS)/long-acting β2-agonist (LABA) combinations or maintenance treatment with low-dose ICS as preferred controller therapy. Moderate asthma should be controlled with Step 3 treatment, namely maintenance treatment with low-dose ICS/LABA combinations. Finally, controlling severe asthma requires Step 4 and 5 treatments, which include maintenance treatment with medium- to high-dose ICS/LABA combinations and add-on tiotropium and/or monoclonal antibody therapy in those patients that remain uncontrolled, despite maintenance therapy.
A recent pairwise meta-analysis performed by Sobieraj et al. [3] has investigated the impact of ICS/LABA as the controller and the quick relief therapy, named single maintenance and reliever therapy (known as “SMART” or “MART”; for simplicity, SMART will be used hereafter) in patients with persistent asthma [3]. Interestingly, SMART was associated with a lower risk of asthma exacerbation when compared with maintenance therapy with ICSs (with or without a LABA) plus a short-acting β2-agonist (SABA) as the relief treatment [3]. Some of the studies [4–9] included in that pairwise meta-analysis [3] may have introduced a risk of bias due to the small number of patients enrolled in the randomised controlled trials (RCTs), leading to the so-called “small-study effect” [10]. Furthermore, the safety profile of SMART was not investigated [3].
Besides SMART, an alternative approach in the treatment of mild asthma is the use of ICS/LABA fixed-dose combination on an as-needed basis, a strategy that might overcome the poor adherence to maintenance treatment with an ICS, and the over-reliance on SABAs for symptom relief. This approach has been investigated in the Symbicort Given as Needed in Mild Asthma (SYGMA) 1 and 2 [11, 12].
Indeed, the current scenario indicates that there is a need to improve the tailored approach of asthma treatment, by ranking the efficacy profile of SMART and as-needed therapies in asthmatic patients matched with the severity of disease. In this respect, the study of Sobieraj et al. [3] was a pairwise meta-analysis that did not compare all the currently available SMART and as-needed therapies for the treatment of asthma. Moreover, to date, no comparison has been performed between SMART and the use of ICS/LABA administered exclusively on an as-needed basis.
A well-conducted meta-analysis of RCTs provides the highest level of evidence, even greater than that obtained by single large RCTs. Moreover, along with the effect estimates, network meta-analyses may produce supporting information of considerable interest for clinicians in the form of treatment rankings, generally summarised by an outcome named the surface under the cumulative ranking curve analysis (SUCRA) [13].
Therefore, considering that, to date, there are no network meta-analyses comparing the impact of the as-needed treatments in asthma, including SMART and ICS/LABA on an as-needed basis, we have carried out a quantitative synthesis via Bayesian network approach by considering phase III RCTs in order to rank and compare the efficacy and safety profile of the currently available SMART and as-needed therapeutic strategies in asthma. The primary efficacy outcome of this study was the risk reduction in severe asthma exacerbation.
Materials and methods
Detailed methods are reported in the supplementary material.
Search strategy and study eligibility
This meta-analysis was performed in agreement with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P; protocol ID: CRD42019136443) [14]. The flow diagram and network nodes are shown in figure 1a and b, and table S1 reports the PRISMA-P checklist [14].

PRISMA-P flow diagram (a) and diagram displaying the network across the treatments (b). The links between the nodes indicate the direct comparisons between pairs of treatments, the thickness of lines is proportional with the number of the patients comparing pairs of treatment head-to-head, and the area of the boxes is proportional with the number of patients receiving the same treatment. HD: high-dose; ICS: inhaled corticosteroid; LABA: long-acting β2-agonist; LD: low-dose; MD: medium-dose; PRISMA-P: Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols; SABA: short-acting β2-agonist; SMART: single maintenance and reliever therapy (known as “SMART” or “MART”; for simplicity, SMART is used in the figure).
A comprehensive literature search was performed for phase III RCTs evaluating the impact of SMART and as-needed therapies for the treatment of asthma. As an example, table S2 reports the literature search terms used for OVID MEDLINE and Annex 1 shows the summary text of the identified records.
Study selection
Phase III RCTs that enrolled asthmatic patients, lasting ≥6 months, and that included at least one arm assessing the effect of any SMART and/or as-needed therapies were selected.
Data extraction
Data were extracted in agreement with Data Extraction for Complex Meta-anALysis (DECiMAL) recommendations [15]. The inter- and intra-rater reliability for data abstraction was assessed via the Cohen's κ score, as previously described [16].
Endpoints
The primary endpoint was the comparison across the different SMART and as-needed therapies with respect to the risk of severe asthma exacerbation. The secondary endpoints included the comparisons across the different SMART and as-needed therapies with respect to the changes from baseline in forced expiratory volume in 1 s (FEV1), morning and evening peak expiratory flow (PEF), changes from baseline in Asthma Control Questionnaire (ACQ) score, and risk of severe adverse events (SAEs).
Quality of studies, risk bias and evidence profile
The summary of the risk of bias for each included RCT was analysed via the Cochrane Risk of Bias 2 (RoB 2) [17] and Jadad score [18]. The weighted assessment of the overall risk of bias was analysed via the Cochrane RoB 2 [17], along with the normalised consistency/inconsistency analysis [19]. The quality of evidence was assessed for the primary endpoint via the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system [20].
Data synthesis and analysis
A network meta-analysis was performed via full Bayesian random-effect model to compare the impact of the different SMART and as-needed therapies in asthmatic patients. Subset analyses were performed in agreement with average patients' characteristics at baseline. Results are expressed as relative effect and 95% credible interval (95% CrI). The SUCRA was calculated for both the primary and secondary endpoints [21]; the SUCRA is 1 when a treatment is considered to be the best, and 0 when a treatment is considered to be the worst [19]. The statistical significance was assessed for p<0.05.
Results
Study characteristics
Data obtained from 32 096 asthmatic patients were selected from 21 phase III RCTs (table S3). Four studies were performed in mild asthma [11, 12, 22, 23], three in moderate asthma [8, 24, 25], four in mild-to-moderate asthma [26–29], and ten in moderate-to-severe asthma [6, 7, 30–36].
In agreement with the search strategy and study selection criteria, the investigated ICS/LABA combinations included budesonide/formoterol in 20 studies [6–8, 11, 12, 22–24, 26–36], fluticasone/salmeterol in four studies [30–32, 34], and beclometasone/formoterol in one study [25]. The only ICS administered as monocomponent was budesonide in 10 studies [6, 11, 12, 22, 24, 26, 28, 29, 35, 36]. Formoterol was the only LABA used alone as-needed in three studies [8, 23, 33], whereas a SABA, either salbutamol or terbutaline, was used alone as-needed in 19 studies [6, 7, 11, 12, 22, 24–36].
The definition of severe asthma exacerbation and the level of ICS doses are shown in table S4 and S5 of the supplementary material, respectively. The inter- and intra-rater reliability for data abstraction was generally excellent (Cohen's κ between 0.96 and 1.00). Further study characteristics are reported in the supplementary material.
Primary endpoint
Overall analysis
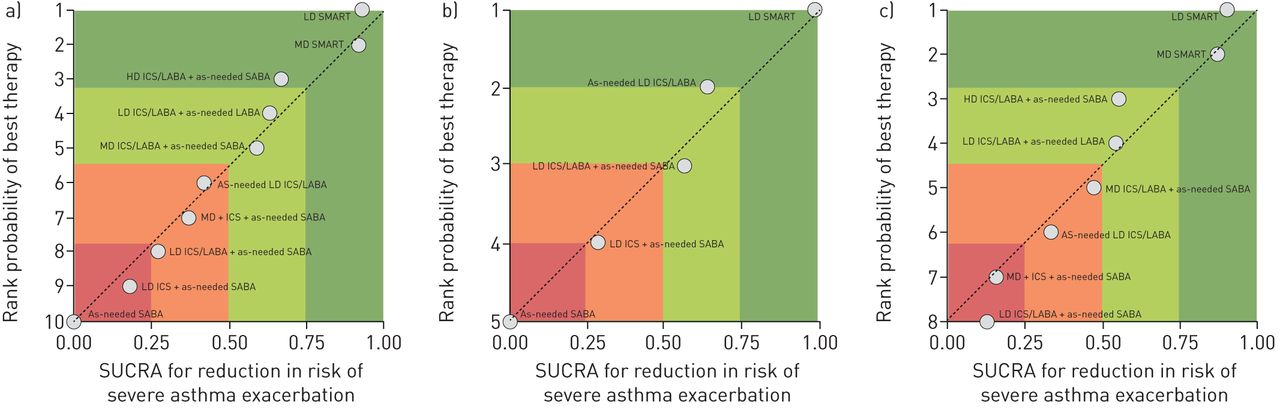
The overall network meta-analysis indicated that low- to medium-dose SMART was as effective as high-dose ICS/LABA+as-needed SABA in reducing the risk of severe asthma exacerbation, and that generally SMART was significantly (p<0.05) more effective than treating asthmatic patients with either lower doses of ICS/LABA+as-needed LABA or SABA, or ICS/LABA used exclusively on an as-needed basis, or ICS+as-needed SABA. No significant difference (p>0.05) was found when comparing high-dose ICS/LABA+as-needed SABA with either lower doses of ICS/LABA+as-needed LABA or SABA, or ICS/LABA used exclusively on an as-needed basis or ICS+as-needed SABA. Moreover, administering ICS/LABA exclusively on an as-needed basis or lower doses of ICS/LABA+as-needed LABA or SABA had the same effect on the risk of severe asthma exacerbation (p>0.05), although only the former therapy was significantly (p<0.05) more effective than ICS+as-needed SABA. All the investigated treatments were significantly (p<0.05) more effective than as-needed SABA in reducing the risk of severe asthma exacerbation, and detailed relative effect with 95% CrI are shown in table 1. The forest plot of the overall comparisons across the investigated treatments is shown in figure 2a. The SUCRA confirmed the comparison resulting from the overall network meta-analysis, by positioning low- to medium-dose SMART in the first quartile along with high-dose ICS/LABA+as-needed SABA therapy (fig. 3a).
Relative effects with 95% CrI resulting from the overall network meta-analysis in asthmatic patients. Treatment comparisons have been sorted in agreement with SUCRA# findings for the primary endpoint reported in figure 3a

Overall forest plot of the comparisons across different SMART and as-needed therapies on the risk of severe asthma exacerbation (a) and subset network meta-analyses in adult mild-to-moderate (b) and moderate-to-severe (c) asthmatic patients. Treatments comparisons have been sorted in agreement with level of efficacy. CrI: credible interval; HD: high-dose; ICS: inhaled corticosteroid; LABA, long-acting β2-agonist; LD: low-dose; MD: medium-dose; RR: relative risk; SABA: short-acting β2-agonist; SMART: single maintenance and reliever therapy (known as “SMART” or “MART”; for simplicity, SMART is used in the figure).
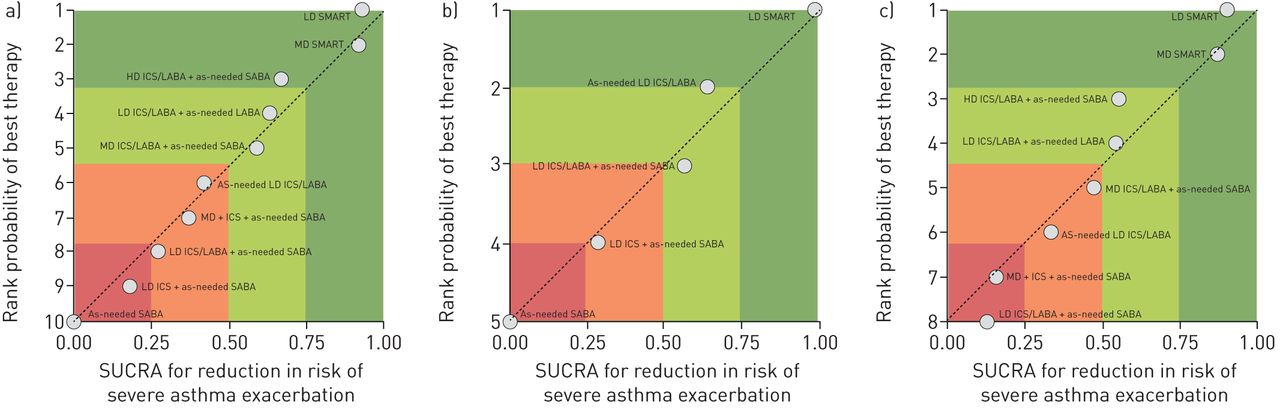
Ranking plot of the efficacy of as-needed therapies in preventing the risk of severe exacerbation. Overall ranking plot displaying the efficacy of as-needed therapies in preventing the risk of severe exacerbation in asthmatic patients (a) and subset analyses on adult mild-to-moderate (b) and moderate-to-severe (c) asthmatic patients. Therapeutic strategies were plotted on the X-axis according to the surface under the cumulative ranking curve analysis (SUCRA), where 1 results for a treatment considered to be the best, and 0 for a treatment considered to be the worst. The treatments were plotted on the Y-axis according to the rank probability of best therapy, where a score of 1 is assigned to the best therapeutic strategy. HD: high-dose; ICS: inhaled corticosteroid; LABA: long-acting β2-agonist; LD: low-dose; MD: medium-dose; SABA: short-acting β2-agonist; SMART: single maintenance and reliever therapy (known as “SMART” or “MART”; for simplicity, SMART is used in the figure); SUCRA: surface under the cumulative ranking curve.
Subset analyses
The subset network meta-analysis performed on adult mild-to-moderate asthmatic patients reported that low-dose SMART and ICS/LABA used exclusively on an as-needed basis were equally effective (p>0.05) in preventing the risk of severe asthma exacerbation. Low-dose SMART was significantly (p<0.05) more effective than both ICS/LABA+as-needed SABA and ICS+as-needed SABA, whereas the efficacy of as-needed ICS/LABA on the risk of severe asthma exacerbation was significantly (p<0.05) superior to ICS+as-needed SABA but not to ICS/LABA+as-needed SABA (p>0.05). All the above reported treatments were significantly (p<0.05) more effective than as-needed SABA in reducing the risk of severe asthma exacerbation, and detailed relative effect with 95% CrI are shown in table 2. The forest plot of the comparisons across the investigated treatments in adult mild-to-moderate asthmatics is shown in figure 2b. The SUCRA confirmed the subset analysis in adult mild-to-moderate asthmatic patients, with low-dose SMART and ICS/LABA used exclusively on an as-needed basis positioned in the first quartile (fig. 3b).
Relative effects with 95% CrI resulting from the subset network meta-analysis in adult mild-to-moderate asthmatic patients. Treatments comparisons have been sorted in agreement with SUCRA# findings for the primary endpoint reported in figure 3b
The subset network meta-analysis performed on adult moderate-to-severe asthmatic patients showed that low- to medium-dose SMART and high-dose ICS/LABA+as-needed SABA were equally effective in reducing the risk of severe asthma exacerbation (p>0.05). Low- to medium-dose SMART, but not high-dose ICS/LABA+as-needed SABA, was generally significantly (p<0.05) more effective against the risk of severe asthma exacerbation than lower doses of ICS/LABA+as-needed LABA or SABA and ICS+as-needed SABA. Detailed relative effect with 95% CrI of the subset analysis performed in adult moderate-to-severe asthmatic patients are reported in table 3. The forest plot of the comparisons across the investigated treatments in adult moderate-to-severe asthmatics is shown in figure 2c. Figure 3c reports the SUCRA in which the low- to medium-dose SMART was ranked in the first quartile. The diagram displaying the network and the relative nodes of this subset analysis are shown in figure S3a and S3b of the supplementary material.
Secondary endpoints
Peak expiratory flow
The results of the overall network meta-analysis showed that low- to medium-dose SMART and high-dose ICS/LABA+as-needed SABA were equally effective (p>0.05) in improving morning and evening PEF, and that both these therapeutic strategies were generally significantly (p<0.05) more effective than lower doses of ICS/LABA+as-needed SABA or LABA, ICS/LABA used exclusively on an as-needed basis, ICS+as-needed SABA, and as-needed SABA. The efficacy of lower doses of ICS/LABA+as-needed SABA or LABA on the improvement in morning and evening PEF was generally significantly (p<0.05) greater than as-needed ICS/LABA, ICS+as-needed SABA, and as-needed SABA. Administering ICS/LABA exclusively on an as-needed basis significantly (p<0.05) improved PEF when compared with ICS+as-needed SABA, low-dose ICS/LABA+as-needed SABA, and as-needed SABA.
Detailed relative effect with 95% CrI of the overall network meta-analysis on morning and evening PEF are reported in table 1 and SUCRA values in table S6.
Forced expiratory volume in 1 s
The overall network meta-analysis indicated that low- to medium-dose SMART and both ICS/LABA+as-needed SABA or LABA were generally equally effective in improving FEV1 (p>0.05). Low- to medium-dose SMART, but not high-dose ICS/LABA+as-needed SABA, was generally significantly (p<0.05) more effective than ICS+as-needed SABA. Lower doses of ICS/LABA+as-needed SABA or LABA significantly (p<0.05) improved FEV1 when compared with low-dose ICS+as-needed SABA, but not when compared with medium-dose ICS+as-needed SABA (p>0.05). Administering ICS/LABA exclusively on an as-needed basis was generally significantly (p<0.05) less effective in improving FEV1 compared with low- to medium-dose SMART and ICS/LABA+as-needed LABA or SABA. The above reported treatments were significantly (P<0.05) more effective than as-needed SABA in improving FEV1.
Detailed relative effect with 95% CrI of the overall network meta-analysis on FEV1 are reported in table 1 and SUCRA values in table S6.
Asthma Control Questionnaire
Data concerning the change in ACQ were spurious when compared with the previously reported outcomes. In any case, when possible, the overall network meta-analysis indicated that low-dose SMART therapy was significantly (p<0.05) more effective than low-dose ICS/LABA+as-needed SABA or LABA, as-needed low-dose ICS/LABA, ICS+as-needed SABA, and as-needed SABA in reducing ACQ. Low-dose ICS/LABA+as-needed SABA or LABA significantly (p<0.05) reduced ACQ compared with both as-needed ICS/LABA and as-needed SABA. Administering either ICS/LABA exclusively on as-needed basis or ICS+as-needed SABA significantly (p<0.05) improved ACQ only with respect to as-needed SABA. Medium-dose ICS/LABA+as-needed LABA was significantly (p<0.05) more effective than all the above reported therapeutic options in reducing ACQ.
Detailed relative effects with 95% CrI of the overall network meta-analysis on ACQ are shown in table 1 and SUCRA values in table S6.
Severe adverse events
No statistically significant (p>0.05) differences were found across the investigated treatments with respect to their impact on the risk of SAEs, excluding a significant (p<0.05) reduction in the risk of SAEs detected for low-dose SMART compared with low-dose ICS/LABA+as-needed SABA. Detailed information on the relative effect with 95% CrI of the risk of SAEs is reported in table 1 and SUCRA values in table S6.
Subset analyses
Tables 2 and 3 show results of the subset analyses on adult mild-to-moderate and moderate-to-severe asthmatic patients, respectively.
Relative effects with 95% CrI resulting from the subset network meta-analysis in adult moderate-to-severe asthmatic patients. Treatments comparisons have been sorted in agreement with SUCRA# findings for the primary endpoint reported in figure 3c
Risk of bias and quality of evidence
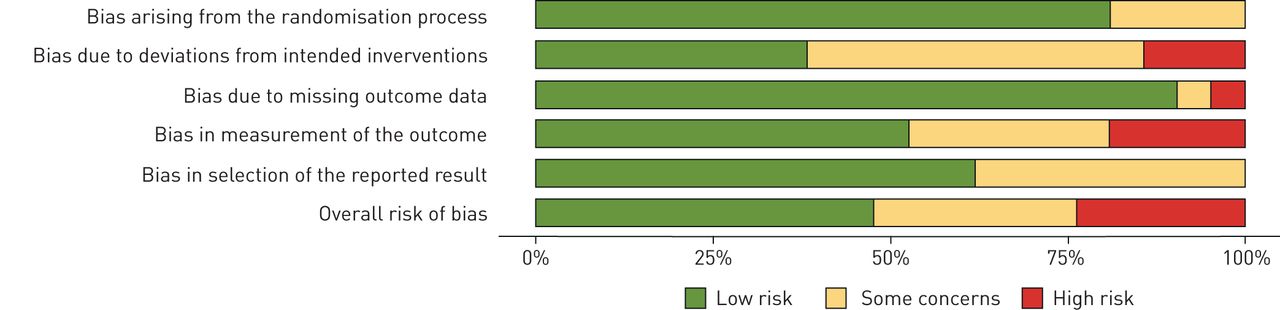
The weighted plot for the assessment of the overall risk of bias by domains is shown in figure 4, and the traffic light plot for the assessment of each included RCT is reported in figure S1. Most the RCTs had a low risk of bias for the randomisation process (17 (81.0%)), missing outcome data (19 (90.5%)), measurement of the outcomes (11 (52.4%)), and selection of the reported results (13 (61.9%)). Of the 21 RCTs, four (19.0%) had a high risk of bias due to the measurement of the outcomes, three (14.3%) due to deviations from intended intervention, and one (4.8%) due to missing outcome. Ten studies (47.6%) had some concerns on the risk of bias in the domain of deviations from intended intervention.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Weighted plot for the assessment of the overall risk of bias via the Cochrane RoB 2 tool (n=21 studies).
Most the studies (90.47%) included in this network meta-analysis were ranked as being of medium-to-high quality in agreement with Jadad score; whereas, only 9.53% of them were characterised by low-quality level. The sensitivity analysis performed by excluding the two studies [6, 7] reporting a Jadad score ≤2, and for which the RoB 2 tool mainly provided some concerns to high risk of bias (figure S1), did not result in significant (p>0.05) differences in both the relative effect and SUCRA, compared with the overall network meta-analysis.
The normalised consistency/inconsistency analysis showed that all points fit adequately with the line of equality (overall goodness of fit: R2 0.997; slope 1.027, 95% CI 1.022–1.032), indicating that this network meta-analysis was not affected by significant bias (figure S2a–f). The lack of bias in the overall Bayesian network was further confirmed by the absence of significant (p>0.05) inconsistency factors when the investigated as-needed therapies were compared directly or indirectly. No significant (p>0.05) inconsistency resulted for the subset analyses of both primary and secondary endpoints performed in agreement with disease severity.
The overall quality of evidence ranked in agreement with the GRADE system concerning the impact of each SMART and as-needed treatment in preventing the risk of severe asthma exacerbation is reported in table 1. The specific GRADE analysis performed in adult mild-to-moderate asthmatic patients indicated that the low-dose SMART and the use of ICS/LABA used exclusively on an as-needed basis, both therapeutic strategies positioned in the first quartile by SUCRA, were ranked as having a high quality of evidence (median value: ++++). In adult moderate-to-severe patients low- to medium-dose SMART, the only therapeutic strategy positioned in the first quartile by SUCRA, was also ranked as having a high quality of evidence (median value: ++++) in preventing severe asthma exacerbation.
Discussion
The main finding resulting from the meta-analysis of the primary endpoint is that SMART and as-needed therapies are effective strategies in preventing the risk of severe asthma exacerbation, and that as-needed SABA administered as monotherapy should be avoided in all asthmatic patients. Specifically, the treatment ranking analysis of the efficacy of specific as-needed therapies against the risk of severe asthma exacerbation provides the high quality of evidence that both low-dose SMART and administering ICS/LABA exclusively on an as-needed basis are the best therapeutic options in adult patients suffering from mild-to-moderate asthma, and that low- to medium-dose SMART should be considered the first therapeutic strategy in adult moderate-to-severe asthmatic patients. From a clinical point of view, the effect estimate resulting from the network meta-analysis in adult mild-to-moderate asthmatic patients indicates that both low-dose SMART and the use of ICS/LABA exclusively on an as-needed basis overlapped the minimal clinically important difference (MCID; at least a reduction from four to three exacerbations per year, meaning ∼0.75 RR) [37, 38] in reducing the risk of severe asthma exacerbation compared with either ICS/LABA+as-needed SABA, or ICS+as-needed SABA, or as-needed SABA. Generally SMART reached such a level of MCID also in patients suffering from moderate-to-severe asthma versus low- to medium-dose ICS/LABA+as-needed LABA or SABA, and ICS+as-needed SABA, but not when compared with higher dose of ICS/LABA+as-needed SABA. Thus, since high-dose ICS/LABA+as-needed SABA was ranked in the upper position of the second quartile of SUCRA, this therapeutic approach could be considered as second-line treatment in preventing the risk of severe asthma exacerbation.
SMART was effective also on secondary endpoints, as it generally improved lung function and disease control compared with the other as-needed therapies in adult mild-to-moderate asthmatic patients. Conversely, in adult patients with moderate-to-severe asthma, low- to medium-dose SMART was only partially more effective than the other as-needed therapies on lung function and asthma control. Unexpectedly, no differences were found on the safety profile measured as the risk of experiencing SAEs across all the investigated therapeutic strategies and clustered in agreement with disease severity.
The findings of this network meta-analysis concerning the efficacy of as-needed ICS/LABA treatments strongly support the evidence raised from the SYGMA 1 and 2 studies [11, 12], in which it resulted that although the treatment with as-needed budesonide/formoterol prevented severe exacerbations, this therapeutic option was less effective than budesonide maintenance therapy at mitigating symptoms and improving lung function [39]. In any case, the differences in these treatment outcomes were smaller than the accepted MCIDs for these endpoints [12].
The fraction of exhaled nitric oxide (FeNO) is useful to predict the response to ICS treatment, to monitor the adherence to therapy, and as a diagnostic tool in ICS-naïve patients [40]. FeNO seems to be also a predictive factor for the risk of asthma exacerbation [40, 41]. In this respect, the Novel START Study [22] documented a greater reduction in the FeNO levels among patients treated with either as-needed budesonide/formoterol or budesonide maintenance therapy compared with those treated with as-needed SABA. Nevertheless, although budesonide maintenance therapy resulted significantly more effective than as-needed budesonide/formoterol in reducing FeNO [22], the findings of our study demonstrate that as-needed ICS/LABA is significantly more effective than maintenance ICS therapy+as-needed SABA in preventing the risk of severe exacerbation in mild-to-moderate asthmatic patients.
The discrepancy between the results of this meta-analysis and the assumption that the levels of FeNO are related with the risk of asthma exacerbation [40, 41] could be explained by considering that FeNO levels are poorly reproducible and do not correlate with the severity of exacerbations [42]. As a matter of fact, recent evidences from an open-label RCT performed in mild asthmatic patients reported no significant interaction between baseline biomarkers, namely blood eosinophil count and FeNO levels, and the effect of as-needed budesonide/formoterol for exacerbations and severe exacerbations [43].
The evidences raised from this study further endorse the last version of the current GINA 2020 document that suggests to administer low-dose as-needed ICS/LABA in mild asthma, low-dose ICS/LABA+as-needed low-dose ICS/LABA (low-dose SMART) in moderate asthma, and medium-dose ICS/LABA+as-needed low-dose ICS/LABA (medium-dose SMART) as preferred therapy in severe asthma [2]. Certainly, across the available ICS/LABA combinations, the current evidence supports prevalently the use of as-needed budesonide/formoterol to treat mild asthmatic patients [11, 12, 22], and budesonide/formoterol to be administered as SMART in mild-to-moderate [27–29] and moderate-to-severe asthma [7, 34, 36, , ]. Only one study was performed to test the efficacy of beclometasone/formoterol used as SMART in patients with moderate asthma [25]. However, we cannot omit that a recent study [26] provided the indication that budesonide/formoterol used as-needed for symptom relief was effective in reducing the risk of severe asthma exacerbation in a population that included also moderate asthmatic patients. A further important point is that the current literature does not provide evidence for using as-needed budesonide/formoterol on top of non-formoterol containing combination therapies.
Although this quantitative synthesis clearly provides the rank of efficacy for the as-needed therapies in asthma, an issue could remain concerning the comparison between medium-dose ICS/LABA+as-needed low-dose ICS/LABA (medium-dose SMART) and high-dose ICS/LABA+as-needed SABA in severe, not moderate, asthmatic patients. In fact, the studies that directly compared these two therapeutic options were carried out in patients suffering from moderate-to-severe asthma [9, , ]. However, we have to highlight that despite in the study of Pavord et al. [9] budesonide/formoterol maintenance and reliever therapy was compared with four-fold higher maintenance dose of budesonide, the medium-dose SMART regimen resulted as effective as high-dose ICS/LABA+as-needed SABA in preventing the risk of severe asthma exacerbation. Thus, we could argue that budesonide/formoterol maintenance and reliever therapy is a suitable choice also for the most severe patients.
Network meta-analytic procedures are relatively new and they have been criticised especially for their recent use in the indirect comparison across biologic treatments in severe asthma [44]. We agree that, when a network meta-analysis includes treatments that have been never compared head-to-head in RCTs, the resulting effect estimates from indirect comparisons could be uncertain [44]. Furthermore, although some degree of variation across study populations could be acceptable in pairwise meta-analyses, this can be disastrous in network meta-analyses [44]. Fortunately, several treatments we have assessed in the overall network meta-analysis were directly compared in head-to-head RCTs, leading to network loops that were further consolidated in the subset analyses performed in more homogenous populations, namely adult patients suffering from either mild-to-moderate or moderate-to-severe asthma. Definitely, the methods used in our study permitted to maintain a low and not significant level of inconsistency across the nodes of the Bayesian evidence network [45–47].
However, this study has also limitations. First, some RCTs led to concerns on the overall risk of bias related with the deviation from intended intervention and selection of the reported results. Secondly, considering the number of outcomes that were assessed, some statistically significant associations may represent type I error. Thirdly, the SUCRA should be interpreted in agreement with the quality of evidence, where the lower the quality of evidence the worse the accuracy of SUCRA. Since several outcomes have been investigated in this network meta-analysis, the SUCRA should be considered specifically for each outcome. Moreover, the extent of differences in the effects between treatments is not considered during the computation of SUCRA and, equally important, SUCRA does not allow assessing any statistically significant difference [48].
Indeed, the burden of severe asthma is associated with detrimental clinical impact in patients and increasing healthcare costs [49–51]. Furthermore, therapeutic strategy should be optimised in difficult-to-treat asthma before escalating to add on treatments such as oral corticosteroids or biologic therapy [52, 53]. In this regard, there is the medical and scientific need for balanced and well-designed head-to-head RCTs to assess the extent of superiority of SMART in reducing the risk of severe exacerbation in Step 5 asthmatic patients compared with high-dose ICS/LABA+as-needed SABA.
To conclude, the evidence raised by this network meta-analysis clearly indicates that both SMART and as-needed therapies represent suitable therapeutic options to reduce the risk of severe asthma exacerbation, by providing the most effective positioning of each specific treatment in the management of asthma according to the disease severity. In particular, while low-dose SMART was the first therapeutic choice at every level of disease severity, as-needed low-dose ICS/LABA resulted as effective as low-dose SMART in mild-to-moderate asthma being ranked borderline between the first and second treatment option. Conversely, as-needed low-dose ICS/LABA was ranked only as the sixth option in moderate-to-severe asthma. Although there may be discussion around the regular use of ICS versus as-needed ICS/LABA to treat specifically mild asthmatic patients, to date, there is definitely no rationale for using as-needed SABA as monotherapy in asthma. The findings of this study suggest the correct therapeutic indications to clinicians that, however, should be interpreted in agreement with the medical needs of each single asthmatic patient.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERJ-00625-2020.SUPPLEMENT
Shareable PDF
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-00625-2020.Shareable
Footnotes
This article has supplementary material available from erj.ersjournals.com
Author contributions: P. Rogliani, B.L. Ritondo, J. Ora, M. Cazzola and L. Calzetta had full access to all of the data in the study and take the responsibility for the integrity of the data and the accuracy of the data analysis. P. Rogliani, B.L. Ritondo and L. Calzetta designed the statistical analyses in consultation with J. Ora and M. Cazzola. P. Rogliani and L. Calzetta wrote the first draft of the article, in consultation with J. Ora, B.L. Ritondo and M. Cazzola for data interpretations. All authors revised the article critically for important intellectual content, gave final approval of the version to be published, and agreed to be accountable for all aspects of the article in ensuring that questions related to the accuracy or integrity of any part of the article were appropriately investigated and resolved. P. Rogliani and L. Calzetta are the guarantors of this review and meta-analysis.
Conflict of interest: P. Rogliani reports grants and personal fees from Boehringer Ingelheim, Novartis, Chiesi Farmaceutici and Almirall, personal fees from AstraZeneca, Biofutura, GlaxoSmithKline, Menarini and Mundipharma, grants from Zambon, outside the submitted work.
Conflict of interest: B.L. Ritondo has nothing to disclose.
Conflict of interest: J. Ora has nothing to disclose.
Conflict of interest: M. Cazzola reports grants and personal fees from Boehringer Ingelheim, Novartis, Almirall and Zambon, personal fees from AstraZeneca, Chiesi Farmaceutici, ABC Farmaceutici, Edmond Pharma, Verona Pharma, Ockham Biotech, Biofutura, GlaxoSmithKline, Menarini, Lallemand, Mundipharma and Pfizer, outside the submitted work.
Conflict of interest: L. Calzetta reports grants and personal fees from Boehringer Ingelheim, Novartis and Zambon, non-financial support from AstraZeneca, grants from Chiesi Farmaceutici and Almirall, personal fees from ABC Farmaceutici, Edmond Pharma, Verona Pharma and Ockham Biotech, outside the submitted work.
- Received March 10, 2020.
- Accepted May 7, 2020.
- Copyright ©ERS 2020
References










