





Abstract
Background Overuse of short-acting β2-agonists (SABA) may indicate poor asthma control and adverse health outcomes. Contemporary population-based data on use, risk factors and impact of SABA (over)use on asthma exacerbations and mortality are scarce, prompting initiation of the global SABINA (SABA use IN Asthma) programme.
Methods By linking data from Swedish national registries, asthma patients aged 12–45 years with two or more collections of drugs for obstructive lung disease during 2006–2014 were included. SABA overuse was defined as collection of more than two SABA canisters in a 1-year baseline period following inclusion. SABA use was grouped into 3–5, 6–10 and ≥11 canisters per baseline-year. Cox regression was used to examine associations between SABA use and exacerbation (hospitalisations and/or oral corticosteroid claims) and mortality.
Results The analysis included 365 324 asthma patients (mean age 27.6 years; 55% female); average follow-up was 85.4 months. 30% overused SABA, with 21% collecting 3–5 canisters per year, 7% collecting 6–10 canisters per year and 2% collecting ≥11 canisters per year. Increasing number of collected SABA canisters was associated with increased risk of exacerbation, as follows. 3–5 canisters: hazard ratio (HR) 1.26 (95% CI 1.24–1.28); 6–10 canisters: 1.44 (1.41–1.46); and ≥11 canisters: 1.77 (1.72–1.83), compared to two or fewer canisters per year. Higher SABA use was associated with incrementally increased mortality risk (2564 deaths observed), as follows. 3–5 canisters: HR 1.26 (95% CI 1.14–1.39); 6–10 canisters 1.67 (1.49–1.87); and ≥11 canisters: 2.35 (2.02–2.72) compared to two or fewer canisters per year.
Conclusion One-third of asthma patients in Sweden collected three or more SABA canisters annually. SABA overuse was associated with increased risks of exacerbation and mortality. These findings emphasise that monitoring of SABA usage should be key in improving asthma management.
Abstract
One-third of asthma patients in Sweden were SABA overusers (three or more canisters per year), of whom 28% had no collection of anti-inflammatory drugs. Higher SABA use was associated with increased exacerbation and mortality risks. http://bit.ly/2PqqSKn
Introduction
Worldwide, up to 30 million children and adults aged <45 years have asthma [1], with exacerbations ranging from mild attacks that interrupt daily life and work productivity to severe and life-threatening episodes [2]. Asthma deaths have become rare in developed countries [3]. However, during the past two decades there has been a lack of improvement in asthma control [4] and a plateauing of mortality rates [5], which may be related to poor adherence to inhaled corticosteroids (ICS) and/or overuse of short-acting β2-agonists (SABA) for symptom relief [6, 7]. The increasing trend in overuse of SABA is worrisome, as these agents do not address the underlying inflammatory pathology that gives rise to worsening symptoms. Indeed, the latest iteration of the Global Initiative for Asthma (GINA) report no longer recommends treatment with SABA alone, noting that such therapy does not protect against severe exacerbations and that regular or frequent use actually increases the risk of such events [8]. Used both as a monotherapy and in combination with ICS, SABA overuse is associated with an increased risk of exacerbations, and excessive use (≥11 canisters per year) has been associated with an increased asthma-related mortality risk [8–14]. Nevertheless, contemporary population-based data on use, risk factors and impact of long-term SABA use on exacerbations and mortality are scarce, prompting the initiation of the global SABA use IN Asthma (SABINA) programme. The aim of the SABINA programme is to describe asthma medication prescription patterns, the extent of SABA overprescription and its subsequent impact on clinical and healthcare resource utilisation outcomes via a series of observational studies in >25 countries.
The aims of the present study were to describe the use of SABA over an 8-year period in a nationwide cohort of asthma patients in Sweden; to evaluate the demographic and clinical determinants of SABA overuse; and to investigate the associations between SABA (over)use and the risk of exacerbation, all-cause mortality and respiratory-related death.
Methods
Study design and data sources
This was a retrospective, population-based cohort study utilising national Swedish health registries: 1) the National Patient Register covering all hospital admissions since 1987 and outpatient specialist visits since 2001; 2) the Prescribed Drug Registry, covering all collected outpatient drug prescriptions since July 2005 using Anatomical Therapeutic Chemical (ATC) codes; and 3) the Cause of Death Register [15–17]. Sweden has a publicly funded healthcare system, with equal access for all patients, regardless of socioeconomic status or geographic location. Individual patient data were linked by the Swedish National Board of Health and Welfare using each individual's unique personal identification number, which was then replaced by a study identification number in order to secure anonymisation of the patients prior to data analysis. The study protocol was approved by the Stockholm regional ethics committee (registration number 2017/4:2). The linkage of registers data was approved and performed by the Swedish National Board of Health and Welfare. Patients do not need to give consent for use of public register data in Sweden [18, 19].
Study population
The study population included all asthma patients, defined as individuals aged 12–45 years who collected two or more drugs for obstructive lung disease (ATC R03) from pharmacies in any 1-year period during 2006–2014 in Sweden, a validated proxy for asthma (figure 1) [15]. The lower age cut-off was selected due to differences in asthma management pattern for younger patients, whereas the upper age of 45 years was to mitigate the risk of including patients with chronic obstructive pulmonary disease (COPD). Patients with a diagnosis of COPD (J44), and/or collection of adrenergics in combination with anticholinergics were excluded. To examine oral corticosteroid (OCS) collections indicated for asthma only, patients with diagnosis of other conditions for which OCS may be prescribed were excluded (i.e. Crohn's disease (K50), ulcerative colitis (K51), rheumatoid arthritis (M05), emphysema (J43), bronchiectasis (J47), cystic fibrosis (E84) and current malignancy (C00-97)). Medical history data were retrieved from the National Patient Register using International Classification of Diseases (ICD)-10 codes from 10 years prior to the index date.

Flow chart of study population. SABA: short-acting β2-agonist.
Study measures
SABA use was quantified as the number of canisters collected per calendar year. To enable comparison of different types and number of doses in the SABA canisters, a standardised SABA canister unit was defined as 150 doses. The definition of SABA overuse in the present study was calculated assuming that two puffs were used on each occasion and that a patient with well-controlled asthma would not use their SABA reliever more than twice a week, which equals a maximum of two SABA canisters per year [20]. In practice, this means that the collection of three or more SABA canisters annually was considered as overuse [20]. During the baseline period, patients were grouped by the number of collected SABA canisters: two or fewer (considered appropriate use), three to five, six to 10 and ≥11 (excessive use) [10, 11]. The index date was the date of the second asthma drug collection, and the baseline period was from the index date up to 1-year post-index.
ICS use included both monotherapy and fixed combinations (in budesonide equivalents). The mean daily ICS dose was defined as low dose (≤400 µg), medium dose (401–800 µg) and high dose (>800 µg) [8]. Patients were classified into different treatment severity steps based on their asthma-related drug use during the baseline period (details provided in supplementary table S1).
Comorbidity
Comorbidities were identified based on diagnoses (ICD-10 codes) recorded as part of inpatient and outpatient hospital care. Charlson Comorbidity Index (as marker for the comorbidity burden/fragility of patients) was estimated for the different SABA canisters groups [21].
Outcomes
Asthma exacerbation was defined as either a pharmacy collection of a course of OCS, or emergency room visits and/or hospitalisations due to asthma. All-cause, respiratory-related (J00–J99) and asthma-related (J45–J46) mortality was investigated during the observation period. Identification of asthma exacerbation and death were performed from the first day after the baseline period (last patient included December 31, 2014) until date of death, emigration or end of observation (December 31, 2016), whichever occurred first. The use of SABA and ICS was described for the first 3 years after the baseline period.
Statistical analyses
Baseline characteristics were described as mean±sd for continuous variables and absolute and relative frequencies for categorical variables. Logistic regression models were applied to estimate odds ratios with 95% confidence intervals of possible risk factors for SABA overuse (more than two (three or more) canisters) during the baseline period. Age at asthma diagnosis, sex, treatment steps, hypnotics and sedative drugs and comorbidity were explored individually as well as in multivariable adjusted analyses. Risk of exacerbation and mortality, post-index date, by baseline SABA use was assessed by hazard ratios with 95% confidence intervals in Cox proportional hazard models. Exacerbation was assessed by time to first exacerbation after the baseline period. As a sensitivity analysis, a stratification for patients with and without exacerbations during the baseline period was performed. In all regression analyses, both crude estimates as well as estimates adjusted for age at asthma diagnosis, sex, treatment steps and comorbidity were calculated. Exacerbation-free survival by baseline period SABA use, stratified by baseline period ICS use (no/yes) was evaluated through Kaplan–Meier graphs. Of note, in all assessment of exacerbation during follow-up patients with treatment step 5 during the baseline period were excluded, since these patients are regular users of OCS. Statistical analyses were performed using R version 3.3.2 (R Foundation for Statistical Computing, Vienna, Austria, 2013).
Results
Overall, 365 324 asthma patients (mean age 27.6 years, 55% female) were included (figure 1), of whom 30% overused SABA: 76 619 (21.0%) collected three to five canisters, 27 065 (7.4%) collected six to 10 canisters and 7140 (2%) collected ≥11 canisters during the 1-year baseline period (table 1). The observation period covered on average 85.4 (range 0.03–120) months after the 1-year baseline period. Half of the included patients were at treatment steps 1 and 2, and 34% and 16% were in steps 3 and 4, respectively.
Baseline characteristics by use of short-acting β2-agonists (SABA) during baseline year
After the 1-year baseline period, patients collecting more than two SABA canisters were similar regarding age and sex compared to those not overusing SABA, but had more asthma exacerbations, asthma-related hospitalisations and outpatient hospital visits (table 1). In addition, SABA overuse was associated with a greater comorbidity burden.
During the 1-year baseline period, the collection of ICS and long-acting β2-agonists (LABA), both as monotherapy and in combination, was similar irrespective of baseline SABA use. However, treatment with OCS differed between the SABA groups, with a higher prevalence of OCS use in patients who collected a higher number of SABA canisters (table 1). In addition, the use of antidepressants, hypnotics and sedatives was greater in patients with SABA overuse (table 1).
Patterns of ICS and SABA use over time
Among patients collecting more than two SABA canisters per year over a 3-year period after baseline, the proportion of patients in all three SABA overuse groups was stable, and in parallel, the use of ICS was stable and did not change during the 3-year period (despite continuous SABA overuse) (supplementary figure S1). From a full population perspective, ∼85% of asthma patients overusing SABA at baseline had continuous overuse during the observation period, whereas the proportion of patients not collecting any ICS was more than doubled at the end of observation (supplementary table S2).
Factors associated with SABA overuse
Males, adolescents and older patients were more likely to overuse SABA compared to females and those in the 18–24-year age group (table 2). Compared to patients in treatment step 3, patients in the other treatment steps had greater risk of overusing SABA, with a 50% and 90% increased risk for patients in treatment steps 1 and 5, respectively. In addition, use of hypnotics and sedative drugs and increasing comorbidity burden were associated with increased risk of SABA overuse.
Factors associated with short-acting β2-agonist (SABA) overuse (more than two (three or more) collected canisters per year)
Exacerbations
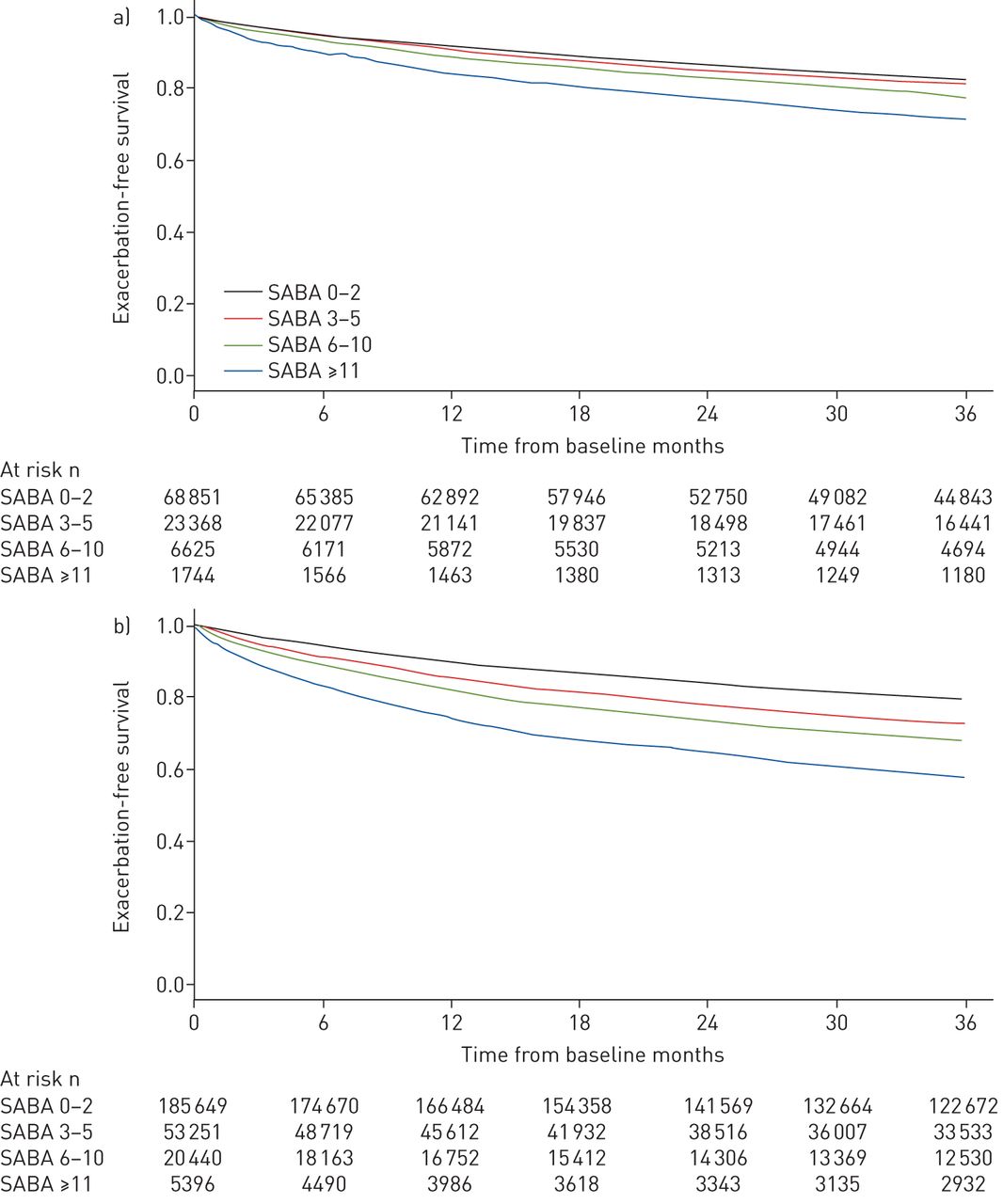
Increasing number of collected SABA canisters was associated with an increased risk of exacerbations in a dose-dependent manner after adjusting for treatment step, Charlson Comorbidity Index, sex and age (figure 2). Irrespective of treatment step, patients overusing SABA (more than two (three or more) canisters per year) were at an increased risk of exacerbations in a dose-dependent manner compared to those not overusing SABA. In the sensitivity analysis where patients were stratified into two groups (with or without exacerbations during the baseline period), the exacerbation risk and SABA use was similar in both groups (supplementary table S3). Similarly, SABA overuse was associated with more exacerbations irrespective of whether concomitant ICS was used at baseline or not (figure 3). A small proportion of patients (2.3%) were collecting LABA without concomitant ICS. In this group, SABA overuse was associated with a two-fold greater exacerbation risk (data not shown).
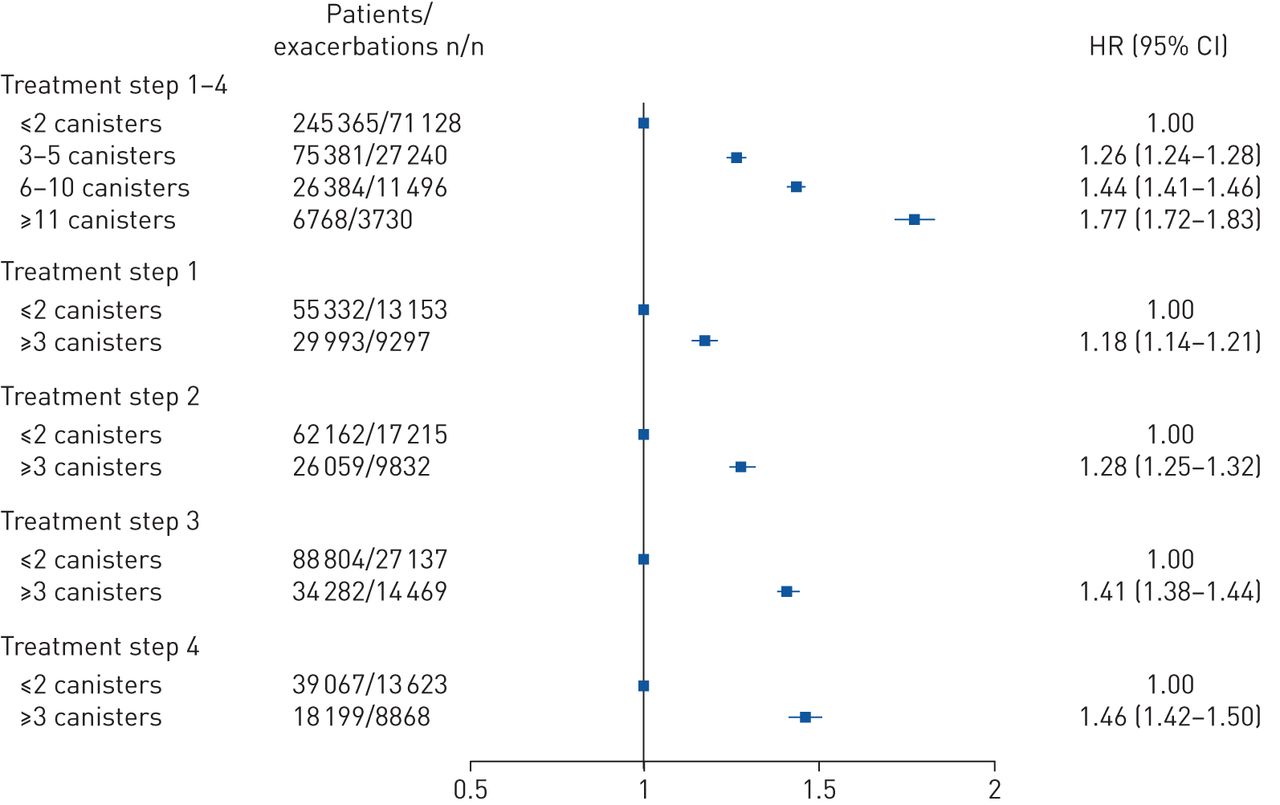
Associations between baseline short-acting β2-agonist (SABA) use and treatment step and subsequent risk of asthma exacerbation. Adjusted for age at asthma diagnosis, sex, treatment step and comorbidity. ≤2 canisters: patients collecting two or fewer SABA canisters during the baseline year; ≥3 canisters: patients collecting three or more SABA canisters during the baseline year; HR: hazard ratio.

Exacerbation-free survival in different baseline period short-acting β2-agonist (SABA) use groups. a) Patients not treated with inhaled corticosteroids (ICS) during the baseline year, n=100 588; b) patients treated with ICS during the baseline year, n=264 736.
Mortality
During the observation period, 1365 (0.54%) of the asthma patients in the group collecting two or fewer SABA canisters per year died compared with 1199 (1.07%) among the patients collecting more than two (three or more) SABA canisters at baseline (table 3 and figure 4). The mortality rate increased with increasing number of collected SABA canisters (figure 4). After adjusting for treatment step, Charlson Comorbidity Index, sex and age, increasing number of SABA canisters collected was associated with greater risk of all-cause, respiratory- and asthma-related mortality in a dose-dependent manner (figure 5).
Cause of death among asthma patients by use of short-acting β2-agonists (SABA) during baseline year
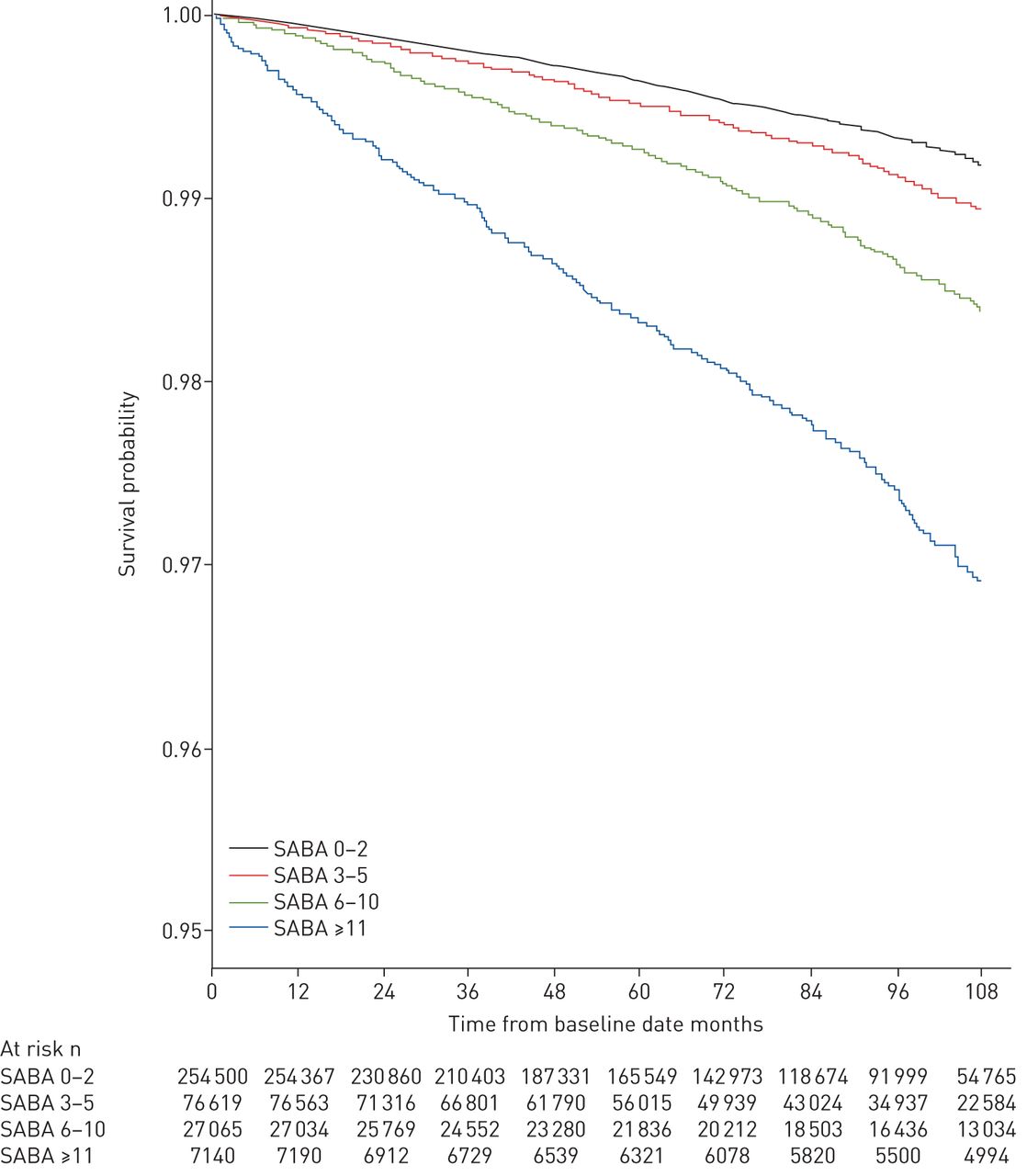
Kaplan–Meier plot of overall survival by baseline short-acting β2-agonist (SABA) use.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Association between baseline short-acting β2-agonist (SABA) use and risk of mortality. a) Overall mortality; b) asthma-related mortality; c) respiratory-related mortality. Adjusted for treatment step, Charlson Comorbidity Index, sex and age. ≤2 canisters: patients collecting two or fewer SABA canisters during the baseline year; ≥3 canisters: patients collecting three or more SABA canisters during the baseline year; HR: hazard ratio.
Discussion
In this nationwide asthma cohort study, which was conducted as part of the global SABINA programme, approximately one-third of all asthma patients in Sweden were overusing SABA. Male sex, age, use of hypnotics and sedative drugs and increasing comorbidity burden were the main determinants of SABA overuse. Notably, SABA overuse was also associated with an increased risk of exacerbation and all-cause-, respiratory- and asthma-specific mortality compared to appropriate SABA use.
A key finding of the present study was the observed association of SABA overuse with dose-dependent increased risk of all-cause mortality. Indeed, while six times as many patients died in the excessive SABA use group (≥11 canisters collected) compared to the group with appropriate SABA use, an association between SABA overuse and risk of all-cause mortality was also found at lower levels of SABA overuse. Other studies have reported an association between excessive SABA use and increased risk of asthma-related deaths, and our findings for respiratory and asthma-specific deaths are in keeping with these previous studies [16–18, 22]. Although most of the studies regarding SABA overuse and asthma mortality were undertaken in the 1990s, our findings from contemporary data emphasises the fact that SABA overuse continues to be a risk factor for mortality and that there is a dose-dependent trend at three or more canisters collected per year.
As the majority of deaths in our study cohort are not related to asthma, our findings indicate that SABA overuse may be a general marker for increased risk among asthma patients. In addition, a parallel association between all SABA overuse and increased risk of respiratory and asthma-related deaths was also observed. Our data showed an increased use of antidepressants, hypnotics and sedatives in patients with SABA overuse, indicating a frailer patient group. Regardless of whether there is a causal effect of SABA use and these adverse effects, or if they are mainly a marker for more severe asthma and/or a reflection the frailty of the patients, increased use of SABA should alert clinicians to monitor these patients more closely [10, 23, 24].
No significant changes in the proportion of patients in the different SABA overuse groups were seen among the those consistently collecting more than two SABA canisters per year over a 3-year period after baseline. Interestingly, this persistent long-term SABA overuse did not trigger any significant changes in asthma management, as no concomitant increase in maintenance ICS therapy was identified. This may be explained by the Swedish healthcare setting, where annual reviews in primary care, and referrals to specialist care for asthma patients are scarce, as previously reported by Larsson et al. [25]. In addition, Janson et al. [26] showed recently that asthma patients in Sweden, regardless of exacerbation frequency, did not have more frequent healthcare visits or alterations in asthma medication than patients with fewer exacerbations. That study suggested that repeated prescriptions of asthma drugs may be issued without proper consultation with the treating physicians.
An additional observation from our study is that mild and severe asthma, i.e. treatment steps 1 (without concomitant use of maintenance ICS therapy) and 5, were both associated with an increased risk of SABA overuse compared to step 3. This highlights the need for appropriate drug therapy for mild asthma patients [24]. This has been noted in the recently updated GINA report, where SABA without ICS should no longer be a treatment option in mild asthma [8]. Other important predictors for SABA overuse were male sex, younger age and having a greater use of hypnotics and sedative drugs, as well as increasing comorbidity burden indicating a generally more frail patient population. These findings are in line with those of other studies [9, 12], as well as our findings of an association between the use of increased number of SABA canisters and risk of exacerbations, both for patients with and without concomitant use of maintenance ICS therapy [11, 23].
The present findings have several potential clinical implications. According to GINA, patients with well-controlled asthma should not have need for reliever therapy (SABA) more than twice weekly. The definition of SABA use in the present study is calculated assuming that two puffs are used on each occasion, which equals a maximum of two SABA canisters per year. In practice, this means that collection of three or more SABA canisters annually is considered as overuse. A large proportion (30%) of asthma patients in our study had SABA overuse. Of these, almost one in 10 patients used more than six canisters per year, and for the majority of these patients, SABA overuse was maintained throughout a 3-year observation period. With SABA overuse being a clear marker of patients with an increased risk of exacerbations and mortality [12], this is quite remarkable.
One of the strengths of the present study is the nationwide perspective, thus including all asthma patients in Sweden during the study period. The nationwide data ensured that selection bias was minimised, and consequently the generalisability of the study findings is enhanced. One limitation of the study is the use of pharmacy collection of drugs for obstructive lung disease as a proxy for asthma diagnosis and treatment, and the lack of access to primary-care data, where asthma diagnosis may commonly be captured. However, the collection of drugs for obstructive lung disease has been shown to be a suitable proxy for asthma diagnosis in this age group in validation studies from Sweden [15]. To mitigate the risk of including patients with COPD, a number of exclusion criteria were applied, including patient aged >45 years, COPD diagnosis and use of COPD-specific drugs. Similarly, as some OCS use could relate to other conditions than asthma, patients with conditions for which OCS may be prescribed were excluded. Another potential limitation was that SABA use was based on collected prescriptions, which may not fully reflect patients’ actual medication use. It should be noted that comorbidities managed only in primary care were not captured in our database and may thereby be underestimated in our study. In addition, the possibility of coding errors cannot be completely ruled out; however, validation studies have reported high correlation between data in the Swedish National Patient Register and diagnoses in medical records [15, 16].
In conclusion, the present findings demonstrate that a large proportion of asthma patients in Sweden are overusing SABA, and that such overuse may be maintained for several years without any addition or dose adjustment of the maintenance ICS. SABA overuse was associated with a dose-dependent increased risk of exacerbations and increased all-cause, respiratory and asthma-related mortality risk. Such findings emphasise that monitoring of SABA usage should be a key strategy in improving asthma management.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERJ-01872-2019.SUPPLEMENT
Shareable PDF
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-01872-2019.Shareable
Acknowledgements
The authors would like to thank Urban Olsson (Statisticon AB, Uppsala, Sweden), for data management. Helena Goike (AstraZeneca Nordic-Baltic, Södertälje, Sweden), is acknowledged for valuable comments to the manuscript. Bright Nwaru acknowledges the support of Knut and Alice Wallenberg Foundation, the Wallenberg Centre for Molecular and Translational Medicine, and the VBG Group Herman Krefting Foundation on Asthma and Allergy.
Footnotes
This article has an editorial commentary: https://doi.org/10.1183/13993003.00542-2020
This article has supplementary material available from erj.ersjournals.com
The dataset supporting the conclusions of this article can be available upon request.
Author contributions: Data collection was performed by C. Janson. Statistical analysis was conducted by F. Wicklund and B.I. Nwaru. Analysis, interpretation and drafting of the manuscript was conducted by B.I. Nwaru and P. Hasvold and in cooperation with the other authors. All authors approved the manuscript before submission.
Conflict of interest: B.I. Nwaru reports personal fees for advisory board work from AstraZeneca, during the conduct of the study.
Conflict of interest: M. Ekström reports personal fees for advisory board work from AstraZeneca, during the conduct of the study.
Conflict of interest: P. Hasvold is an employee of AstraZeneca.
Conflict of interest: F. Wicklund is an employee of Statisticon, for which AstraZeneca is a client.
Conflict of interest: G. Telg is an employee of AstraZeneca.
Conflict of interest: C. Janson has received payments for educational activities from AstraZeneca, Boehringer Ingelheim, Chiesi, Novartis, and Teva, and has served on advisory boards arranged by AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, and Teva.
Support statement: The study was sponsored by AstraZeneca. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received September 20, 2019.
- Accepted December 10, 2019.
- Copyright ©ERS 2020
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










