





Figures
- FIGURE 1
Traditional treatment steps using short-acting β2-agonist (SABA) reliever therapy versus anti-inflammatory reliever (AIR) treatment steps and risk of severe exacerbations in published randomised controlled trials. ICS: inhaled corticosteroid; LABA: long-acting β2-agonist. The following studies contained inclusion criteria that required a history of an exacerbation in the 12 months prior to randomisation [18, 19, 21–23, 25, 27–29]. The risk of severe exacerbation (AIR versus traditional algorithm) was reported as relative rate [6, 15, 16, 19, 21, 23–25, 27, 29], relative risk [7, 17, 28] and hazard ratio [18, 22], respectively. Studies prescribed reliever therapy as follows; budesonide/formoterol (B/F) 200/6 μg, one actuation as required for relief of symptoms [6, 7, 15, 16, 19, 21, 22, 24, 25, 27–29]; B/F 100/6 μg, one actuation as required for relief of symptoms [17, 18]; ultrafine beclometasone dipropionate/formoterol 100/6 μg (BDP/F), one actuation as required for relief of symptoms [23].
- FIGURE 2
Prototype anti-inflammatory reliever therapy algorithm for clinic-based review in adult asthma based on budesonide/formoterol 200/6 µg Turbuhaler. Alternative cut points could be used to guide transition between steps (see text). GP: general practitioner.
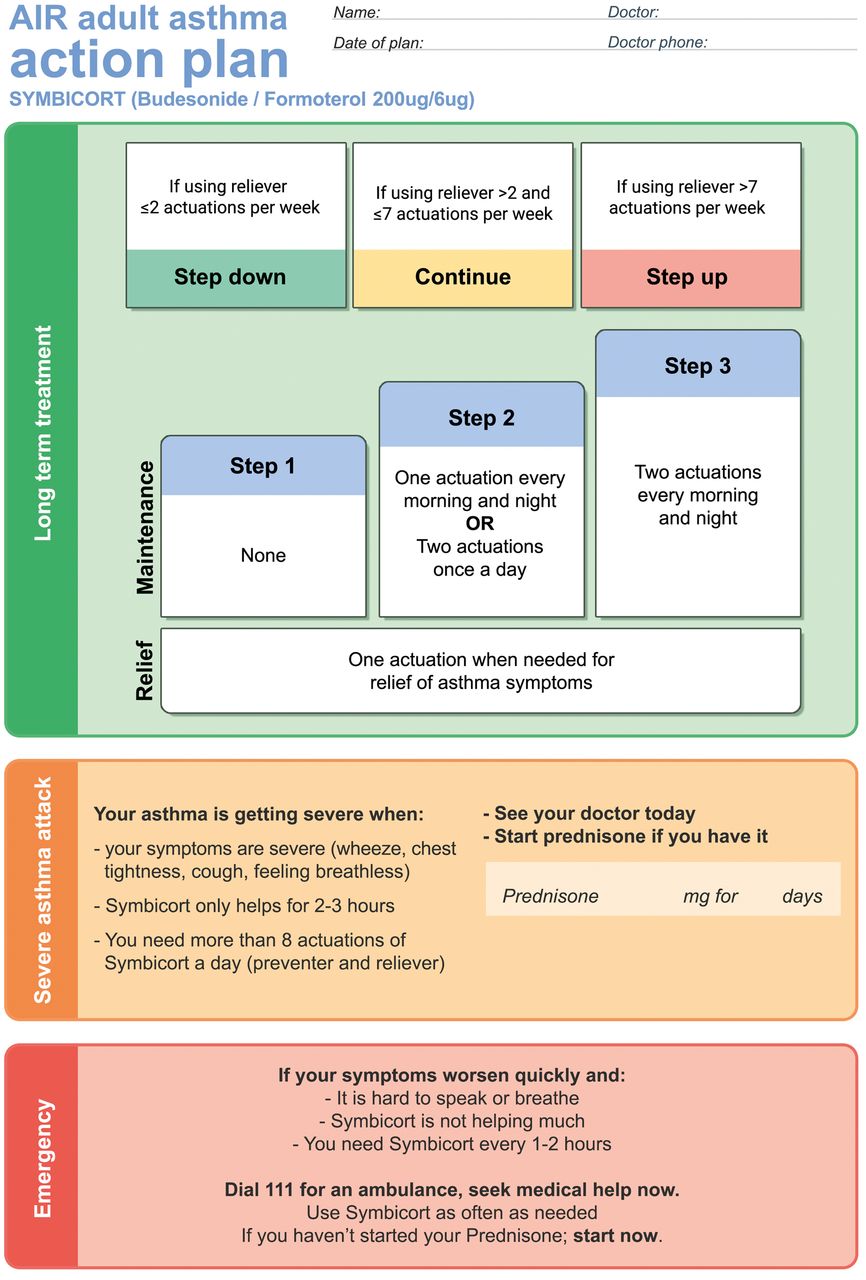
- FIGURE 3
Prototype adult asthma action plan for the anti-inflammatory reliever therapy stepwise treatment algorithm developed from the action plans used in the studies of budesonide/formoterol reliever therapy that demonstrated efficacy and safety of this regimen [7, 25]. On the reverse side of the plan additional information and guidance can be provided, but not limited to inhaler and spacer technique, medication use and the frequency of recommended medical review.


{kind=link}
{kind=link}
{kind=link}
Supplementary Materials
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-01407-2019.Shareable










