





Abstract
An e-cigarette user developed giant cell interstitial pneumonia, a rare disease largely limited to work exposure to hard metals, including cobalt. Analysis of the e-liquid identified significant levels of cobalt, supporting the e-cigarette's causative role. http://bit.ly/2VRcT1U
To the Editor:
The spectrum of pulmonary disease caused by e-cigarette use is currently emerging and appears to be multifaceted [1]. We describe a patient who developed pathologically documented giant cell interstitial pneumonia following regular use of an e-cigarette. This disorder has been termed hard metal pneumoconiosis, or cobalt lung, due to its close association with exposure to hard metal (cemented tungsten carbide with cobalt) [2]. Analysis of the device's e-liquid revealed significant levels of cobalt, supporting a diagnosis of giant cell interstitial pneumonia associated with inhaled cobalt from regular e-cigarette use.
A 49-year-old previously healthy Caucasian female presented with progressive shortness of breath on exertion. She had a non-productive cough and wheezing. She denied any other symptoms. She had recently been given a diagnosis of asthma following an adverse reaction to ketorolac injection for low back pain. At that time, she was told it could be related to her environment. Home medications included daily montelukast 10 mg tablet and albuterol inhaler p.r.n. She had recently worked as a dog trainer, but stopped due to dyspnoea. She had a remote history of smoking cigarettes in her teens and twenties. She had been using a marijuana e-cigarette (ZenPen personal vaporiser) for 6 months.
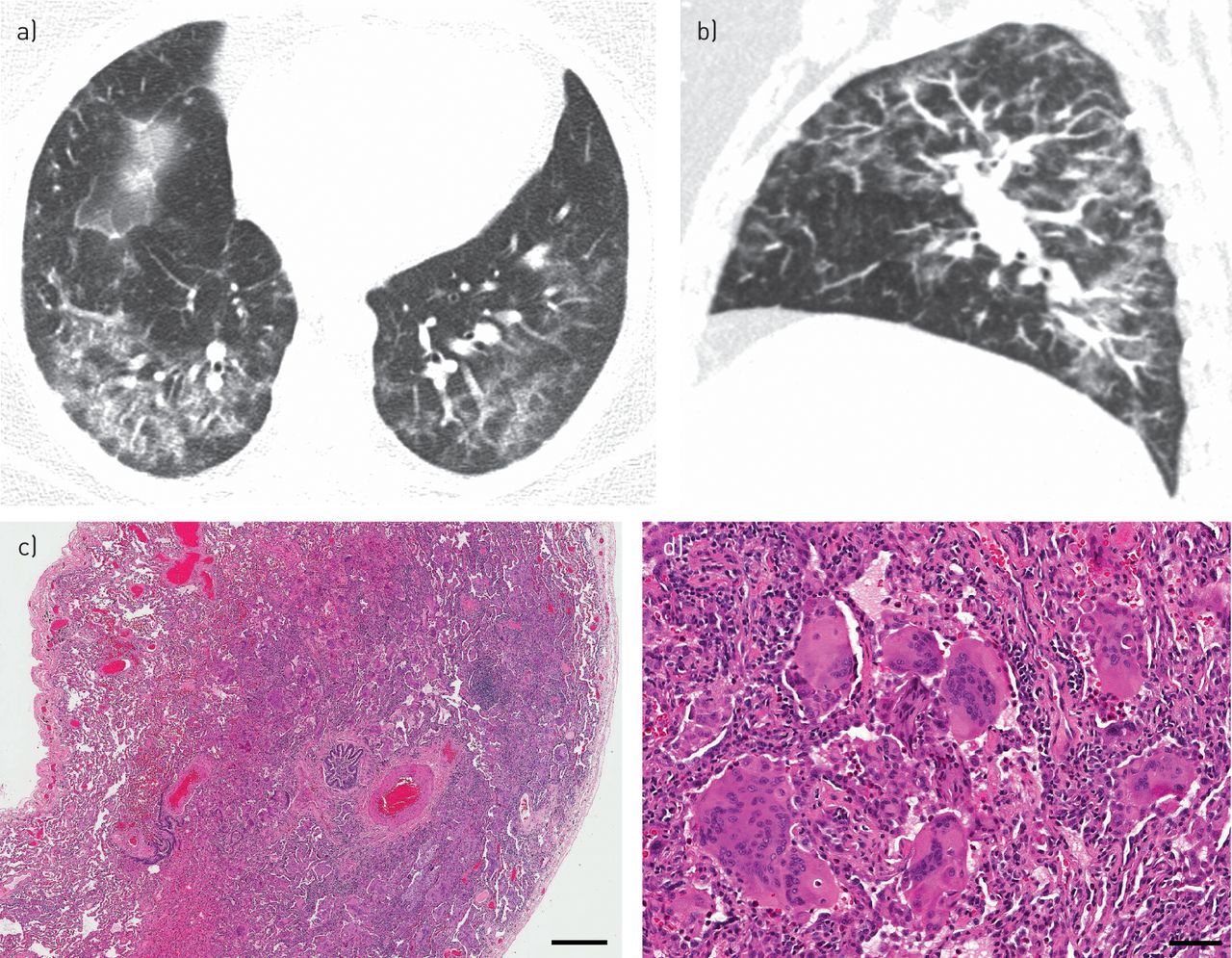
Physical examination showed a well-nourished woman with blood pressure 147/88 mmHg, heart rate 73 bpm, respiratory rate 18 bpm, and oxygen saturation 96% on room air. During a walk test in clinic she desaturated to 87% on room air after 2 min, with a heart rate of 114 bpm and respiratory rate of 25 bpm. Auscultation of her lungs revealed inspiratory crackles at the bases bilaterally. Pulmonary function tests showed moderately severe restriction with a severe diffusion defect: forced vital capacity (FVC) 1.58 L (51% predicted), forced expiratory volume in 1 s (FEV1) 1.28 L (50% predicted), FEV1/FVC 81%, total lung capacity (TLC) 2.67 L (56% predicted), diffusing capacity of the lung for carbon monoxide (DLCO) 7.7 mL·min−1·mmHg−1 (27% predicted) and transfer coefficient of the lung for carbon monoxide (KCO) 4.17 mL·min−1·mmHg−1·L−1 (99% predicted). Computed tomography (CT) scan of the chest showed bilateral ground glass opacity and ill-defined nodules predominating in the centrilobular regions with sparing of the subpleural lung (figure 1a and b). There was no reticulation, traction bronchiectasis or honeycombing. She underwent a surgical lung biopsy for diagnosis.

{kind=link}
a) Axial and b) sagittal reconstructed computed tomography images demonstrate bilateral ground glass opacity and ill-defined nodules. The centrilobular distribution of these findings is demonstrated by the predominance around distal pulmonary arterial branches (which run parallel to bronchioles) and the presence of subpleural sparing. Giant cell interstitial pneumonia: c) low magnification shows bronchiolar-centred interstitial fibrosis with prominent intra-alveolar macrophages and multinucleated giant cells (haematoxylin and eosin, scale bar 1000 μm); d) high magnification shows consolidation of alveolar spaces by macrophages and multinucleated giant cells showing emperipolesis (haematoxylin and eosin, scale bar 50 μm).
Standard haematoxylin and eosin-stained histological sections from the surgical lung biopsy were reviewed by light microscopy.
The e-liquid from the ZenPen micro-vaporiser belonging to the patient was analysed using inductively coupled plasma mass spectrometry (ICP-MS) as described previously by Hess et al. [3]. Two aliquots from the same sample were analysed, and the mean metal concentration of the two replicates was calculated. The metals analysed were aluminium, chromium, manganese, cobalt, nickel, arsenic, molybdenum, tungsten, cadmium and lead.
Glass slides containing 5 μm sections of formalin-fixed paraffin embedded (FFPE) tissue were deparaffinised and sputtered with a conductive layer of platinum. Field emission scanning electron microscopy (FESEM) (SIGMA VP500; Carl Zeiss Microscopy, Pleasanton, CA, USA) was used for structural evaluations at 1 keV. Elemental composition was analysed by energy dispersive X-ray spectroscopy (EDX) (Bruker Nano Inc., Madison, WI, USA) at 20 keV. To increase the power of detection, 10 μm sections of FFPE tissue were mounted on carbon glass tiles, deparaffinised, and FESEM-EDX was repeated.
The right lung upper lobe surgical biopsies showed alveolar septal thickening by fibrosis with bronchiolocentric accentuation (figure 1c). There were numerous multinucleated giant cells within the alveolar spaces (figure 1d). Several of the giant cells showed emperipolesis, with intact histiocytes engulfed within their cytoplasm (so-called “cannibalistic giant cells”). No interstitial granulomas were noted. No significant polarisable or other foreign material was identified by light microscopy. Based on the histological findings a diagnosis of giant cell interstitial pneumonia (hard metal pneumoconiosis) was made.
The patient's ZenPen micro-vaporiser was sent for analysis by ICP-MS at the Dept of Environmental Health Sciences, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA. The metals detected were nickel (mean concentration 30 443 ppb), aluminium (15 360 ppb), manganese (3231 ppb), lead (1652 ppb), cobalt (654 ppb) and chromium (381 ppb). Tungsten was not detected.
FESEM-EDX was performed on formalin fixed paraffin embedded lung tissue for elemental analysis. No cobalt or tungsten particles were detected.
The final diagnosis in this case was giant cell interstitial pneumonia, secondary to cobalt exposure from the patient's e-cigarette. The patient stopped all vaping and smoking after receiving the diagnosis. She was initially reluctant to take steroids due to possible weight gain so she was started on mycophenolate mofetil (MMF). She improved significantly but stopped taking MMF after 3 months due to its perceived side-effects. Her pulmonary function tests showed a slight decline and she was started on prednisone at that time. She refused transition to alternative steroid-sparing agents, and was tapered off steroids after 1 year. After the initial improvement in lung function, her pulmonary function testing remained relatively stable with most recent values (30 months after diagnosis) as follows: FVC 2.30 L (75% predicted), FEV1 1.88 L (74% predicted), FEV1/FVC 84%, TLC 2.96 L (62% predicted), DLCO 15.4 mL·min−1·mmHg−1 (58% predicted), KCO 4.76 mL·min−1·mmHg−1·L−1 (116% predicted). Her CT scan was relatively stable over the 30 month period following diagnosis, but showed subtle changes suggesting mild fibrosis, including a slight increase in density of the ground glass opacities, more volume loss, and mild reticulation.
To our knowledge, this report of giant cell interstitial pneumonia is the first case of e-cigarette use resulting in a definitive pathology of known cause. The use of e-cigarettes has resulted in a variety of clinical patterns of lung disease and it is likely that various mechanisms are producing different pathological patterns. A recent series reporting the pathological changes of vaping-associated lung injury showed features of acute and subacute lung injury pattern, including acute fibrinous organising pneumonia, diffuse alveolar damage and organising pneumonia, often with bronchiolitis [4]. Proposed mechanisms include abnormalities in surfactant or lipid regulation, lipoid pneumonia, and metal or other fume inhalation injury [1, 5]. Inhalation of metal fumes or dusts has been implicated in several diseases. Metal fume fever from exposure to oxides of zinc, copper and magnesium results in flu-like symptoms [6]. Inhalation of metal dusts most commonly results in dust macules, but occasionally results in diffuse granulomatous disease [7, 8]. Inhalation of cobalt, most commonly as a component of hard metal, is one of the few exposures that results in a highly specific histological finding known as giant cell interstitial pneumonia [9, 10].
Giant cell interstitial pneumonia is a rare form of interstitial lung disease with histological features that are most often found in patients with exposure to hard metal or cobalt [11, 12]. These findings include bronchiolocentric interstitial fibrosis with alveolar accumulation of macrophages and “cannibalistic” multinucleate giant cells as seen in this case. The most common radiographic appearance is a reticulonodular pattern with ground glass opacities and traction bronchiectasis predominantly involving the upper lobes [12, 13]. A restrictive pattern of lung disease is reflected in pulmonary function tests. Hard metals and alloys that have been implicated in this disease include tungsten carbide and cobalt, whose physical properties enable their use in tools for drilling wells, sharpening or cutting metals, polishing diamonds and dental procedures [11, 13]. Workers are at risk of occupational exposures during the production or use of tungsten carbide or cobalt tools. Rarely, other environmental exposures have been suspected in patients who developed giant cell interstitial pneumonia without a clear history of hard metal exposure, including fire fighters and welders [14], and rare cases of nitrofurantoin toxicity have been described [15]. Treatment of hard metal pneumoconiosis consists of removing the exposure, which may improve or stabilise lung function [16], and corticosteroid therapy and/or steroid-sparing therapy [12].
There is additional evidence that e-cigarette liquid and aerosol samples contain detectable concentrations of toxic metals. Hess et al. [3] used ICP-MS to examine cartomiser liquid from five brands of e-cigarettes and reported high levels of toxic metals including nickel, cadmium, chromium, lead and manganese. Similarly, Goniewicz et al. [17] used ICP-MS to measure heavy metals in the aerosol of 12 brands of e-cigarettes and detected cadmium, lead and nickel. Williams et al. [18] reported concentrations of nickel that were 2–100 times greater in e-cigarettes in comparison to standard brand cigarettes, while lead and chromium were present in similar concentrations. Another study interrogated the transfer of toxic metals from the heating coil to the liquid within the e-cigarette reservoir and the generated aerosol [19]. The findings showed higher concentrations of chromium, nickel, lead, manganese and zinc in the reservoir and aerosol samples compared to the cartomiser liquid, suggesting that the heating coil induced contamination of the liquid.
The presence of cobalt in the e-cigarette in this case could be related to differences in the material composition of the reservoir casing or the heating coil. Notably higher temperatures are required to aerosolise the active ingredient of cannabis oil, tetrahydrocannabinol (∼230°C [20]), in comparison to e-cigarettes, which aerosolise nicotine, ethylene glycol and glycerine at temperatures ranging from 110 to 185°C [21]. A study on e-cigarettes showed that the emission of toxic substances increased with raising the voltage supplied to the device [22]. Our inability to detect cobalt in the lung tissue by FESEM-EDX is disappointing, but is likely secondary to a combination of two factors. First, cobalt is highly soluble in body fluids and is excreted rapidly in the urine [23]; for example, Abraham et al. [24] detected cobalt in only 20% of cases with known hard metal exposure. Second, FESEM-EDX is more effective at detecting dust-like particulates. In this case, the cobalt-contaminated aerosolised vapour may result in deposition of particles below the limit of sensitivity for this technique.
Our results suggest that regulation of the material composition of the reservoir and heating coil in the vaporisation device should be sought to avoid toxic exposure when the device is being used as intended to vaporise cannabis oil. The public health implications of this are substantial given the increasing trend towards legalisation of cannabis for recreational and medical purposes. The risk of metal exposure for never-smokers and young users is of particular concern, inasmuch as long-term sequelae may develop, as shown in the present case. The more common pathological alterations in vaping-associated lung injury appear to be variations of acute lung injury pattern. However, this case demonstrates that other insidious toxicities can arise from e-cigarette use. Further studies are needed to determine whether severity of disease relates to duration or extent of exposure.
Shareable PDF
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-01922-2019.Shareable
Acknowledgement
We thank Sunita Ho and Misun Kang of the UCSF Biomaterial and Bioengineering Correlative Microscopy Core. The authors appreciate the critical and constructive comments of the reviewers. This case was alluded to in a recent correspondence (Henry TS, Kanne JP, Kligerman SJ. Imaging of vaping-associated lung disease. N Engl J Med 2019; 381: 1486–1487).
Footnotes
Conflict of interest: D.R. Fels Elliott has nothing to disclose.
Conflict of interest: R. Shah has nothing to disclose.
Conflict of interest: C.A. Hess has nothing to disclose.
Conflict of interest: B. Elicker has nothing to disclose.
Conflict of interest: T.S. Henry has nothing to disclose.
Conflict of interest: A.M. Rule has nothing to disclose.
Conflict of interest: R. Chen has nothing to disclose.
Conflict of interest: M. Golozar has nothing to disclose.
Conflict of interest: K.D. Jones has nothing to disclose.
- Received September 27, 2019.
- Accepted October 16, 2019.
- Copyright ©ERS 2019
References










