





Abstract
Up to 10% of the more than 140 million high-altitude dwellers worldwide suffer from chronic mountain sickness (CMS). Patients suffering from this debilitating problem often display increased pulmonary arterial pressure (PAP), which may contribute to exercise intolerance and right heart failure. However, there is little information on the usual PAP in these patients.
We systematically reviewed and meta-analysed all data published in English or Spanish until June 2018 on echocardiographic estimations of PAP at rest and during mild exercise in CMS patients.
Nine studies comprising 287 participants fulfilled the inclusion criteria. At rest, the point estimate from meta-analysis of the mean systolic PAP was 27.9 mmHg (95% CI 26.3–29.6 mmHg). These values are 11% (+2.7 mmHg) higher than those previously meta-analysed in apparently healthy high-altitude dwellers. During mild exercise (50 W) the difference in mean systolic PAP between patients and high-altitude dwellers was markedly more accentuated (48.3 versus 36.3 mmHg) than at rest.
These findings indicate that in patients with CMS PAP is moderately increased at rest, but markedly increased during mild exercise, which will be common with activities of daily living.
Abstract
This meta-analysis shows that in high-altitude dwellers suffering from chronic mountain sickness, pulmonary hypertension, while rare at rest, is frequent during daily activities http://ow.ly/Mw8730oiZ4z
Introduction
An increase of pulmonary arterial pressure (PAP) is a hallmark of high-altitude exposure and, if pronounced, it may be associated with important morbidity and mortality. Worldwide more than 140 million people are living at high altitude, of whom a substantial number are suffering from chronic mountain sickness (CMS) [1, 2]. For example, among Andean high-altitude dwellers, an estimated 5–10% are suffering from this debilitating disease characterised by excessive erythrocytosis and arterial hypoxaemia [2]. CMS patients often also display increased PAP that is thought to contribute to exercise intolerance and right heart failure, which is common in these patients [3, 4]. There is, however, little information on the extent of the increase of PAP in CMS.
The advent of echocardiography as a reliable tool to noninvasively estimate and compare PAP between groups [5–7] allowed eliminating the restrictions related to the more precise, but invasive and often unavailable, gold standard measurements by right heart catheterisation and permitted investigators to perform studies under field conditions. Since these studies generally comprise relatively few participants, the prevalence of PAP in high-altitude dwellers suffering from CMS remains ill defined at present.
To fill this gap, we systematically reviewed and meta-analysed all data published in English or Spanish on echocardiographic estimations of PAP and measurements of arterial oxygen saturation in high-altitude dwellers (>2500 m) suffering from CMS. Moreover, since there is evidence that in patients with CMS mild exercise during daily activities worsens pulmonary hypertension and contributes to the symptoms and long-term complications [3, 8], we also analysed echocardiographic studies of PAP and arterial oxygen saturation during mild exercise in patients with CMS and high-altitude dwellers.
Materials and methods
We conducted a systematic review and meta-analysis of studies reporting echocardiographic estimates of PAP and arterial oxygen saturation in CMS patients at rest and during exercise. Reviewing and reporting were performed according to the recommendations of the Cochrane collaboration [9] and the PRISMA Statement [10], respectively (supplementary table S1).
Data sources and searches
We searched the MEDLINE and Embase databases up to June 2018, using PubMed and Ovid platforms. We used free-text words and specific thesaurus terms (MeSH in MEDLINE and Emtree in Embase), including “pulmonary artery”, “pressure”, “altitude” and “altitude sickness”. We also examined the bibliographies of relevant articles to identify eligible studies missed by the database searches (supplementary material).
Study selection
We included articles that reported the mean value and standard deviation (or standard error) of PAP by Doppler echocardiography in patients with CMS, defined as erythrocytosis with haemoglobin concentration >21 g·dL−1 in the presence of a normal pulmonary function and no history of working in the mining industry. We excluded small studies reporting data in less than 10 participants, case reports and studies reporting duplicate data. We first checked the abstracts of retrieved articles for eligibility and excluded ineligible studies at this stage. We then examined the full text of potentially eligible articles and, depending on whether they met eligibility criteria or not, included or excluded articles.
Data extraction
Two reviewers (R.S. and N.B.) extracted data, using a data extraction sheet developed and piloted for this review. The two reviewers extracted the mean and standard deviation (or standard error) of systolic PAP and, if reported, the mean and standard deviation (or standard error) of arterial oxygen saturation. In the five studies that also reported PAP and arterial oxygen saturation during mild exercise [3, 4, 8, 11, 12], data for CMS patients and (for comparison) high-altitude dwellers were extracted.
We used the right ventricular-to-atrial pressure gradient as an estimate of systolic PAP. In most included studies, PAP derives from continuous wave Doppler sampling of the tricuspid regurgitation jet, using the simplified Bernoulli equation. In a few studies that reported mean PAP instead of systolic PAP, we used the following formula to calculate systolic PAP: systolic PAP=(mean PAP−2)/0.61 [13]. If atrial pressure had been added to the pressure gradient, we subtracted these estimates to obtain a comparable set of data for meta-analysis. Where cardiac output (L·min−1) during exercise at 50 W was not directly reported, we calculated it according to: stoke volume (mL)×heart rate (beats·min−1)/1000. Cardiac index (L·min−1·m−2) was calculated according to: cardiac output/body surface area (m2). Pulmonary vascular resistance (PVR (Wood Units)) was calculated using: PVR=(mean PAP−PAWP)/cardiac output, where pulmonary arterial wedge pressure (PAWP) was estimated by left atrial pressure.
We further extracted bibliographic details, the study location and its altitude, the number, sex, age and ethnicity of the study participants, and the number of participants excluded from the analysis. Discrepancies between the two reviewers were resolved by discussion and consultation with the senior authors (M.E., U.S. or S.F.R.).
Methodological and reporting quality
We assessed methodological and reporting quality of studies using five criteria. 1) Was the recruitment procedure described? 2) Clear description of inclusion and exclusion criteria. 3) Number of participants with missing data for variables of interest. 4) Was the study population representative for the general population? 5) Was the echocardiography performed according to established standards? 6) Were potential sources of bias addressed?
Statistical analysis
We combined the data on systolic PAP and arterial oxygen saturation using random effects meta-analysis. We converted standard deviation to standard error by dividing the standard deviation by the square root of the number of participants included in the analysis and expressed results as mean values and 95% confidence intervals. We used univariate meta-regression models to identify factors that may have influenced PAP in people suffering from CMS. We included age, study altitude, arterial oxygen saturation, body mass index and haemoglobin. We assessed heterogeneity between studies using the I2 statistic and the Chi-squared test. We used Stata version 11.2 (StataCorp, College Station, TX, USA) for all analyses.
For the simulated distribution, we plotted normal distributions of systolic PAP and oxygen saturation at rest and during exercise for hypothetical populations with and without CMS, based on means and standard deviations of reported data.
Results
Identification of eligible studies
We identified a total of 267 articles. Figure 1 shows the flow of the selection of studies and the reasons for exclusion.

Flow of information through the different phases of systematic review.
Based on titles and abstracts, we excluded 68 duplicates and 180 articles that did not meet inclusion criteria. We examined 19 full-text articles and excluded 10 articles because they did not meet the inclusion criteria (less than 10 participants, high-altitude exposure <1 year).
Characteristics of included studies
Nine studies with a total of 262 participants fulfilled the inclusion criteria [3, 4, 8, 11, 12, 14–17]. The mean age of the participants was 47 years and their number ranged from 58 participants [16] in the largest to 12 participants [15] in the smallest study (table 1). All studies were performed between 3600 and 4350 m altitude in the Andes. All participants were male and had an indigenous Andean (Aymara or Quechua) background. Five studies, in addition to reporting data at rest, also reported measurements during mild exercise. CMS patients and high-altitude dwellers were matched for age, socioeconomic background and ethnicity.
Characteristics of included studies
Methodological and reporting quality
All studies provided a clear description of the eligibility criteria; however, due to missing or incomplete reporting, it was unclear whether participants were truly representative of the general CMS population. In all studies, echocardiography was performed according to the quality criteria of the European Association of Echocardiography [18]. Some, but not all, studies addressed potential sources of bias (table 2).
Assessment of methodological quality of included studies
Two studies reported a selection bias towards the inclusion of patients with mild to moderate disease [3, 14]. This may have resulted in an underestimation of the true magnitude of pulmonary hypertension and arterial oxygen desaturation in the present meta-analysis. One study used the same absolute workload for exercise in all participants and did not use a subjective assessment of exercise intensity [4]. Even though the percentage of the maximal heart rate during exercise was similar in CMS patients and controls, the possibility exists that differences in relative workload may have contributed to the large differences of exercise-induced pulmonary hypertension (and pulmonary interstitial fluid accumulation) between the two groups. Finally, in one study, haemoglobin concentration was slightly <21 g·L−1 in some patients, because of blood-letting shortly before the time of study [11]. It is unlikely that the slightly lower haemoglobin concentrations altered PAP, since isovolaemic haemodilution has no detectable effect on vascular function in CMS patients [19].
Meta-analysis of PAP and arterial oxygen saturation at rest
In all studies, experienced echocardiographers performed the PAP measurements. The point estimate from meta-analysis of the mean systolic PAP at rest was 27.96 mmHg (95% CI 26.28–29.64 mmHg) (figure 2), with the reported mean value ranging from 25.0 to 34.3 mmHg. The point estimate of mean arterial oxygen saturation at rest was 84.27% (95% CI 82.94–85.61%) (figure 3), with the reported mean value ranging from 81.0% to 87.0%. Meta-regression analyses revealed positive relationships between PAP and study altitude (p=0.005) and haemoglobin (p=0.001), and a negative correlation between PAP and arterial oxygen saturation (p=0.005). No significant relationships existed between PAP and age (p=0.56) or body mass index (p=0.98).

Meta-analysis of mean systolic pulmonary arterial pressure (PAP) at rest in high-altitude dwellers suffering from chronic mountain sickness (CMS). Weights are from random effects analysis.

Meta-analysis of mean arterial oxygen saturation at rest in high-altitude dwellers suffering from chronic mountain sickness (CMS). Weights are from random effects analysis.
Meta-analysis of PAP and arterial oxygen saturation during mild exercise (50 W)
Five studies also reported data on systolic PAP and arterial oxygen saturation (figure 4) during mild exercise (50 W) in CMS patients (n=142) and high-altitude dwellers (n=125). The exercise-induced increase of PAP was almost 2-fold larger in CMS patients than in high-altitude dwellers (22.0 versus 13.0 mmHg; p=0.001). The point estimate of systolic PAP during mild exercise in CMS patients was significantly (p=0.001) higher (48.26 mmHg (95% CI 44.76–51.76 mmHg)) than in high-altitude dwellers (36.26 mmHg (95% CI 32.99–39.53 mmHg)). Average systolic PAP during mild exercise ranged from 45.0 to 56.4 mmHg in CMS patients and from 33.0 to 39.8 mmHg in high-altitude dwellers. The point estimate of arterial oxygen saturation during exercise was considerably lower (p=0.0004) in CMS patients (82.14% (95% CI 80.57–83.72%)) than in controls (89.40% (95% CI 88.54–90.26%)) and its mean value ranged from 79.0% to 84.9% in the patients and from 87.7% to 90.3% in the controls.
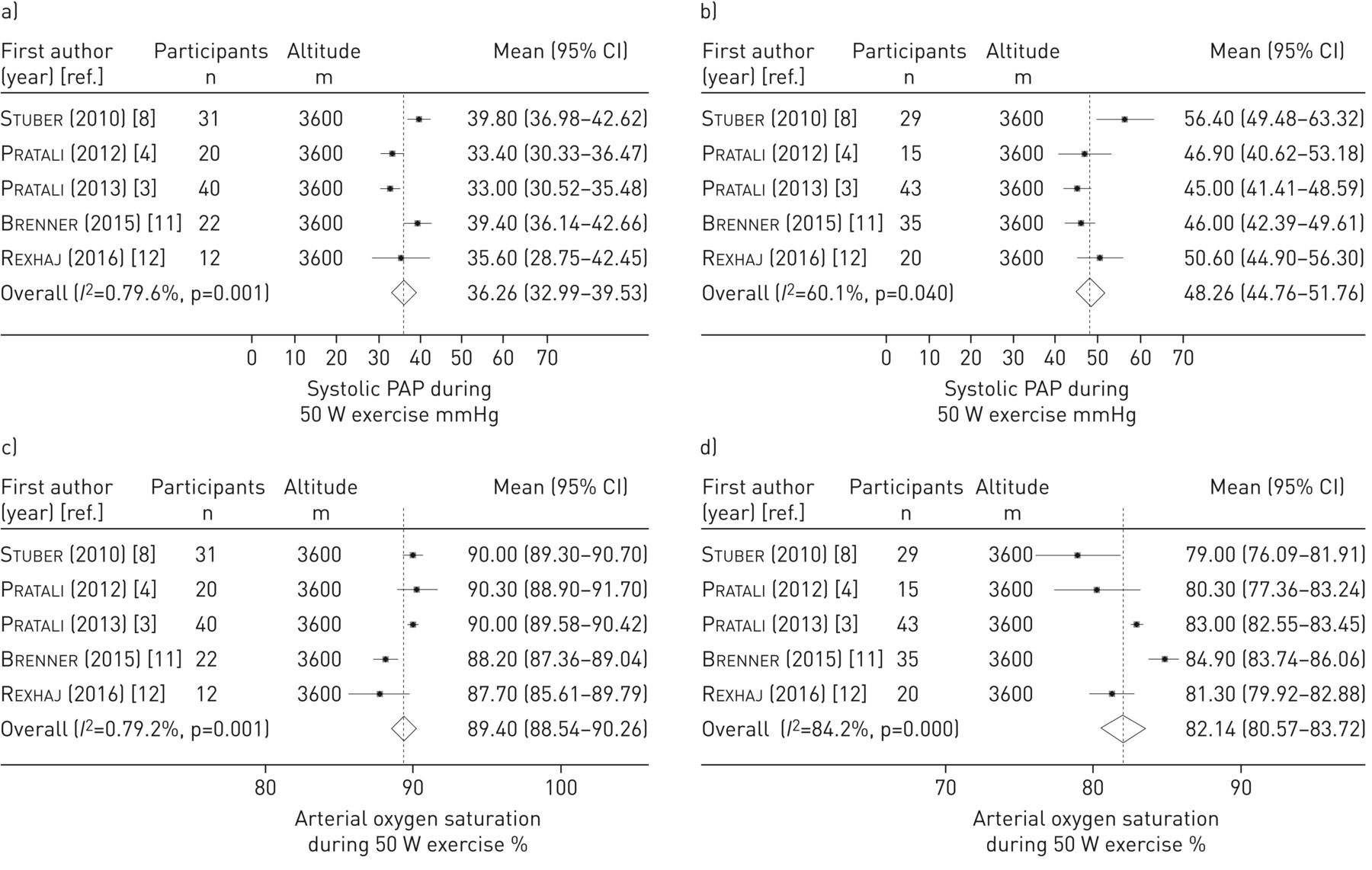
Meta-analysis of a, b) mean systolic pulmonary arterial pressure (PAP) and c, d) mean arterial oxygen saturation during mild exercise (50 W) in a, c) high-altitude dwellers (controls) and b, d) chronic mountain sickness patients. Weights are from random effects analysis.
CO during mild exercise was comparable in CMS patients and controls (9.4±1.1 versus 9.2±0.9 L·min−1; p=0.80), whereas left atrial pressure was slightly, albeit significantly higher in the patients (10.1±0.7 versus 9.2±0.3 mmHg; p=0.0457). Calculated PVR at 50 W tended to be higher in the patients (2.7±0.3 versus 2.2±0.6 mmHg·min·L−1; p=0.090), a tendency which disappeared after correction for the increased haematocrit according to Vanderpool and Naeije [20].
In all meta-analyses the heterogeneity was between 60% and 85%, which in all cases was significant (p-values between 0.04 and 0.0001).
Simulated distribution of PAP and arterial oxygen saturation in CMS patients and high-altitude dwellers
Figures 5 and 6 show simulated distribution curves of PAP and arterial oxygen saturation in CMS patients and high-altitude dwellers at rest and during mild exercise. Curves are shifted towards higher (PAP), respectively lower (arterial oxygen saturation), values in the patients.

Predicted distribution of systolic pulmonary arterial pressure (PAP) in high-altitude dwellers (controls) and chronic mountain sickness (CMS) patients at rest and during mild exercise.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Predicted distribution of arterial oxygen saturation in high-altitude dwellers (controls) and chronic mountain sickness (CMS) patients at rest and during mild exercise.
Discussion
CMS represents a major health problem among the more than 140 million people living at high altitude. In the Andes, 5–10% of high-altitude dwellers suffer from this debilitating disease, which is often associated with increased PAP that is thought to lead to substantial morbidity and mortality [1, 2]. However, the extent of this increase remains poorly defined. To provide such information, we performed a meta-analysis on echocardiographic estimations of PAP and arterial oxygen saturation in 287 high-altitude dwellers suffering from CMS. Since PAP measurements at rest underestimate the values observed during daily activity [8], we also searched for measurements of PAP during mild exercise in the meta-analysed studies [21]. The meta-analysis revealed mean systolic PAP and mean arterial oxygen saturation are roughly 11% higher and 6% lower, respectively, than those meta-analysed previously in high-altitude dwellers living at similar altitude. Mild exercise strikingly accentuates the differences of PAP and arterial oxygen desaturation between the two groups. Taken together, these findings suggest that in CMS patients the PAP increase appears sufficiently severe to cause symptoms and long-term sequels.
The present data represent by far the largest dataset on PAP and arterial oxygen saturation in patients suffering from CMS. Echocardiography is the standard technique to assess PAP in high-altitude populations, since for ethical and logistic reasons invasive measurements are not feasible in population-based studies [21]. Echocardiographic estimations of PAP have been validated against invasive measurements at high altitude [5] with good agreement between invasive and noninvasive measurements [6, 22]. Moreover, agreement between echocardiographic and invasive measures of pulmonary pressures during exercise is good among patients with a high-quality tricuspid regurgitation Doppler signal [23]. Finally, the accuracy of echocardiographic estimations of PAP may depend on the experience of the echocardiographer. It is important to note that experienced investigators who had published extensively in the field performed the estimations of PAP in all the studies meta-analysed [13, 24–26]. Taking the current definitions of pulmonary hypertension as mean PAP >25 mmHg (European Society of Cardiology/European Respiratory Society) [27] or >30 mmHg (high-altitude consensus) [2], the findings of our meta-analysis (systolic PAP of 27.9 mmHg=mean PAP of 19 mmHg) indicate that pulmonary hypertension at rest is rare in CMS patients living at high altitude (3600–4350 m).
The high-altitude consensus [2] states that this limit holds true in the absence of excessive erythrocytosis, implying that an increased haematocrit may be a cause of falsely diagnosed pulmonary hypertension [28]. This effect, which could contribute to differences in PAP between high-altitude populations showing different erythropoietic responses to ambient hypoxia, has, however, never been systematically quantified. Along the same lines, the effects of blood-letting as treatment of increased PAP in CMS are controversial [29–33] and need to be re-examined in controlled prospective studies.
An important strength of the present study is that we also meta-analysed PAP during exercise. There is evidence that PAP measurements at rest may greatly underestimate PAP values during daily activity in CMS patients. In turn, this might underestimate the potential consequences of increased PAP for long-term morbidity and mortality in this population [8]. To provide information on this important issue, we included in our meta-analysis studies assessing PAP during mild exercise (50 W), which will be associated with many activities of daily living. Of note, all exercise studies were performed in the semirecumbent position, a procedure suitable to obtain reliable and reproducible tricuspid regurgitation envelopes during exercise [7].
During mild exercise, the difference in mean systolic PAP between CMS patients and high-altitude dwellers was markedly greater (48.3 versus 36.3 mmHg) than that meta-analysed previously at rest (28.0 versus 25.0 mmHg in CMS versus controls) [21]. Indeed, in CMS patients mean PAP during mild exercise at 50 W (36.3 mmHg (95% CI 33.0–39.5) mmHg)) is above the recently suggested definition of exercise-induced pulmonary hypertension (mean PAP >30 mmHg) [34], whereas in high-altitude dwellers mean PAP remains below this suggested cut-off value (27.2 mmHg (95% CI 25.2–29.3 mmHg)). There is consensus emerging to define exercise-induced pulmonary hypertension by mean PAP >30 mmHg at cardiac output <10 L·min−1 and total pulmonary resistance >3 Wood Units, in the absence of pulmonary hypertension at rest [34]. The present meta-analysis demonstrates that CMS patients fulfil two of these three criteria already at mild exercise. It is likely that many of them will fulfil all three criteria at maximal exercise. In line with this speculation, in the study of Groepenhoff et al. [17], we estimated PVR ∼3.7 Wood Units in CMS patients at maximal exercise.
Of note, in disease states predisposing to pulmonary hypertension, exercise-induced pulmonary hypertension is a well-established cause of decreased exercise capacity, precedes the development of manifest pulmonary hypertension at rest in a proportion of patients and is associated with decreased life expectancy [34]. Several mechanisms may increase PAP in CMS. Pulmonary resistive vessels are less distensible in CMS patients than in healthy highlanders, probably because of vascular remodelling [8, 17], which is also detectable in the systemic circulation [19]. Moreover, exaggerated sympathetic activation [35] in conjunction with increased oxidative/nitrosative stress and decreased nitric oxide bioavailability [36, 37] may also facilitate pulmonary vasoconstriction. Finally, exercise-induced arterial oxygen desaturation was considerably more severe in the patients than in the control subjects (82.1% versus 89.4%).
Collectively, these data strengthen the concept that measurements at rest markedly underestimate pulmonary hypertension and arterial oxygen desaturation during daytime activity in patients with CMS. Interestingly, recent data show that sleep disordered breathing and nocturnal hypoxaemia are more severe in CMS patients than in control subjects [12] and associated with pulmonary vascular dysfunction. It appears therefore possible that daytime measurements of PAP at rest also underestimate differences in PAP between CMS and high-altitude dwellers during sleep. In line with this speculation, invasive measurements of PAP in patients with obstructive sleep apnoea showed a marked progressive increase of PAP during the night [38].
All studies meta-analysed here were performed in Andean high-altitude dwellers. This may be related, at least in part, to the fact that the prevalence of CMS appears to be considerably higher in Andean than in Tibetan or African high-altitude dwellers [39]. Genetic studies provide evidence for differences in the evolutionary adaptation to high altitude between Andean, Tibetan and Ethiopian high-altitude populations [40]. These differences may have resulted in different regulation of the pulmonary circulation and may contribute to differences in PAP between high-altitude populations. It would be important to assess PAP in CMS patients of other than Andean origin.
We used meta-regression models to identify factors that may have influenced PAP in CMS patients. We found that significant positive relationships existed between PAP and study altitude and haemoglobin concentration. Moreover, a significant negative relationship existed between PAP and arterial oxygen saturation. The significant relationship between study altitude and PAP (and arterial oxygen saturation) also indicates that differences in study altitude explain, at least in part, the heterogeneity of the studies meta-analysed. Other reasons for the heterogeneity might be differences in CMS severity between studies or other unreported differences between study populations.
Although the present data represent by far the largest dataset on PAP and arterial oxygen saturation at rest and during mild exercise in patients with CMS and high-altitude dwellers, the number of subjects remains relatively small and is limited to Andeans. Additional studies assessing PAP and arterial oxygen saturation at rest and during mild exercise in CMS patients living in the Andes and, importantly, in other high-altitude regions of the world are urgently needed. Finally, one should keep in mind that echocardiographic measurements of PAP, while highly accurate for population studies, are inappropriate for diagnostic decisions in individuals, because of their lack of precision.
To conclude, this is the first systematic review and meta-analysis of studies reporting echocardiographic estimates of PAP and measurements of arterial oxygen saturation in high-altitude dwellers suffering from CMS. The data indicate that in CMS patients, mean systolic PAP at rest is roughly 3 mmHg higher and arterial oxygen saturation 6% lower than the values previously meta-analysed in high-altitude dwellers [21], but PAP at rest does not fulfil the current criteria for pulmonary hypertension. Importantly, mild exercise expected to be frequently associated with daily activity markedly accentuates the difference in PAP between patients and controls. Exercise-induced pulmonary hypertension may cause symptoms and long-term sequelae in high-altitude dwellers.
The exaggerated increase of PAP during exercise induces interstitial fluid accumulation in the lung [4] and may represent a cause of exertional dyspnoea frequently encountered in CMS patients. Moreover, exercise-induced pulmonary hypertension, however measured, has been shown to be of diagnostic and/or prognostic relevance in mitral valve disease [41], aortic stenosis [42], heart failure [43], systemic sclerosis [44–46], chronic obstructive pulmonary disease [47] and symptomatic patients after pulmonary endarterectomy [48]. Prospective studies are urgently needed examining whether similar long-term sequelae are present CMS patients.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERJ-02040-2018.Supplement
Footnotes
This article has supplementary material available from erj.ersjournals.com
Conflict of interest: R. Soria has nothing to disclose.
Conflict of interest: M. Egger has nothing to disclose.
Conflict of interest: U. Scherrer has nothing to disclose.
Conflict of interest: N. Bender has nothing to disclose.
Conflict of interest: S.F. Rimoldi has nothing to disclose.
Support statement: The authors acknowledge funding from Bundesbehörden der Schweizerischen Eidgenossenschaft (Federal Authorities of the Swiss Confederation). R. Soria was the recipient of a Swiss Federal-Excellence Scholarship for foreign scholars.
- Received October 25, 2018.
- Accepted March 21, 2019.
- Copyright ©ERS 2019
References










