





Figures
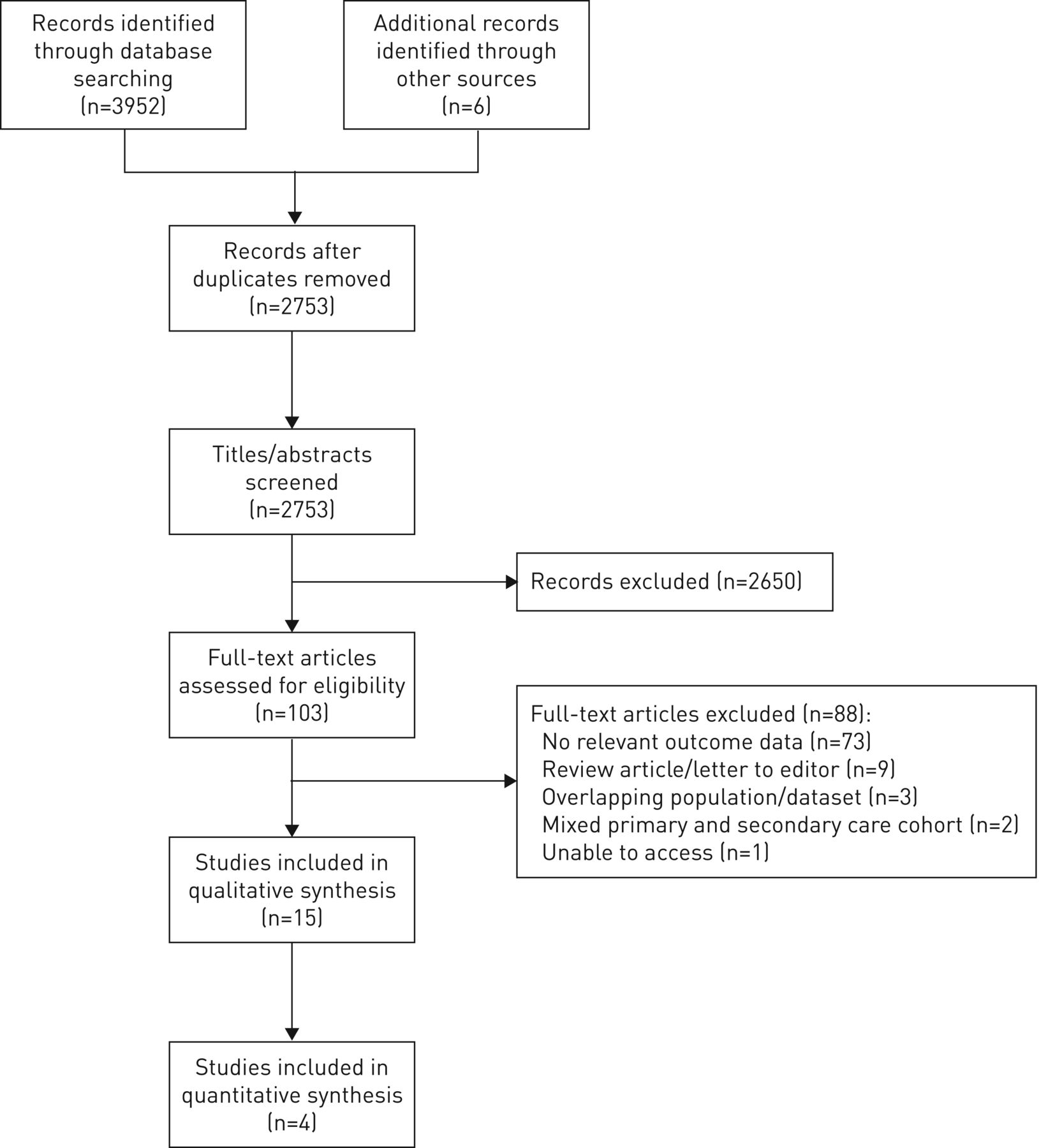
- FIGURE 1
Study flow diagram.
- FIGURE 2
Prevalence of symptoms in recovery following community-acquired pneumonia (CAP): a) one or more symptom, b) cough, c) dyspnoea, d) fatigue, e) chest pain and f) sputum production. Metlay et al. [22] and Daniel et al. [17] are studies of patient cohorts restricted to either low/moderate severity CAP (Pneumonia Severity Index classes I–III or CURB-65 (confusion, urea >7 mmol·L−1, respiratory rate ≥30 breaths·min−1, blood pressure <90 mmHg (systolic) or ≤60 mmHg (diastolic), age ≥65 years) score 0–2) or age <65 years, by design. In the study by Marrie et al. [21], symptom prevalence was assessed twice during the follow-up period (at 14 and 42 days); the other studies reported symptom prevalence once in the defined follow-up period.
- FIGURE 3
Random effects meta-analysis of prevalence of symptoms at 4 weeks following discharge from hospital with community-acquired pneumonia (CAP): a) one or more symptom, b) cough, c) dyspnoea and d) fatigue. ES: effect size. Metlay et al. [22] and Daniel et al. [17] are studies of patient cohorts restricted to either low/moderate severity CAP (Pneumonia Severity Index classes I–III or CURB-65 (confusion, urea >7 mmol·L−1, respiratory rate ≥30 breaths·min−1, blood pressure <90 mmHg (systolic) or ≤60 mmHg (diastolic), age ≥65 years) score 0–2) or age <65 years, by design.


{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Summary of included studies
First author [ref.] Country Study period Study type Study population Outcome Studies with participants selected for low/moderate severity CAP or age <65 years (n=6 studies, n=1217 individual participants) Bruns [6] The Netherlands November 2000–
July 2003Multicentre prospective cohort 119 adults with CAP Normalisation of CAP score at day 10: 32.0%; physician-rated clinical cure at day 28: 88.9% CAP aetiology: S. pneumoniae 27.7% Selection criteria: age: unselected (mean±sd age 56.6±17.8 years); severity: low severity, PSI <110 (mean±sd PSI 65.5±22.1); comorbid disease: unselected; immune status: unselected Carratala [16] Spain October 2000–
October 2002Cohort from multicentre RCT 224 adults with CAP: 101 patients in hospitalised cohort SF-36 score: “At 30-day follow-up SF-36 scores remained abnormal, but had returned towards baseline for Spanish population” CAP aetiology: S. pneumoniae 14.0%, L. pneumophila 4.4%, H. influenzae 2.6%, “atypical” 2.6% Selection criteria: age: unselected (mean±sd age: outpatient group 67.5±11.8 years; inpatient group 64.9±13.4 years); severity: low severity, PSI classes II and III (mean±sd PSI: outpatient group 70±11.6; inpatient group 66.9±12.5); comorbid disease: excluded if pregnant, breastfeeding, respiratory failure, concomitant unstable comorbid conditions necessitating hospitalisation, complicated pleural effusion, lung abscess, shock, metastatic infection, severe social problems, cognitive impairment, psychiatric disease; immune status: immunocompetent only (excluded HIV, splenectomy, immunosuppressive therapy, corticosteroid therapy, neutropenia, solid organ transplant); other: excluded if quinolone allergy or quinolone therapy in preceding 3 months Daniel [17] UK February 2015–
April 2016Multicentre prospective cohort 108 adults with CAP (male 48.2%) Proportion of patients reporting prevalence of symptoms and functional impairment at 28 days following discharge: cough 31.9%, dyspnoea 27.5%, chest pain 16.5%, sputum 11.0%, fatigue 12.1%, ≥1 symptom 58.2%, not returned to ADLs 51.1%, not returned to work 34.3%; reconsultation within 28 days: ED attendance 12.0%, primary care 59.2% CAP aetiology: S. pneumoniae 16.7% Selection criteria: age: 18–65 years only (median (IQR) age 50 (38.3–57.8) years); severity: unselected (CURB-65 0–1: 88.9%; CURB-65 2: 9.3%; CURB-65 ≥3: 1.8%); comorbid disease: unselected; immune status: unselected El Moussaoui [18] The Netherlands November 2000–
July 2003Cohort from multicentre RCT 91 adults with CAP (male 58.8%) Median (IQR) CAP scores: day 3, 56 (38–69); day 7, 60 (37–75); day 10, 65 (37–86); day 14, 77 (61–88); day 28, 75 (58–93) CAP aetiology: S. pneumoniae 23.8% Selection criteria: age: unselected (median (IQR) age 65 (48–72) years); severity: low severity, PSI <110 (mean±sd PSI 71±23); comorbid disease: excluded if pregnant, severe underlying disease, preceding antibiotic treatment for >24 h prior to admission, concurrent comorbid disease likely to interfere with course of pneumonia, respiratory failure; immune status: unselected; other: excluded if amoxicillin allergy Laberere [20] USA/
CanadaJanuary 2001–
December 2001Cohort from multicentre RCT 549 adults with CAP (male 44%) Median (IQR) time for return to ADLs: workers 22 (11–29) days, nonworkers 20 (9–29) days; median (IQR) time return to work 14 (8–29) days CAP aetiology: not reported Selection criteria: age: unselected (median (IQR) age 66 (48–77) years); severity: low severity, PSI classes I–III (PSI I: 16.0%; PSI II: 41.0%; PSI III: 43.0%); comorbid disease: excluded if pulmonary tuberculosis, alcoholism and evidence of end-organ damage, social problems incompatible with recruitment, illicit drug use 30 days; immune status: immunocompetent only (excluded if HIV, immunosuppression) Metlay [22] USA April 1996–
February 1997Single-centre prospective cohort 126 adults with CAP (male 54.8%) Proportion of patients reporting prevalence of symptoms at 28 days following discharge: cough 19.9%, dyspnoea 16.8%, fatigue 25.7%, fever 3.5%, ≥1 symptom 35.0% CAP aetiology: not reported Selection criteria: age: 18–64 years; severity: low severity, PSI classes I–III (mean PSI 55.2); comorbid disease: excluded if pregnancy, severe neuromuscular disease; immune status: immunocompetent only (excluded if chronic immunosuppression, HIV); other: nursing home residence, psychological or social problems compromising follow-up Studies where participants were unselected for severity or age (n=9 studies, n=4427 individual participants) Adamuz [14] Spain January 2007–
December 2009Single-centre prospective cohort 828 adults with CAP (male 65.8%) Healthcare utilisation at 30 days: ED 21.4%, primary care 18.0%; symptoms reported in participants reconsulting within 30 days: primary care (n=149): respiratory symptoms 75.2%, general symptoms 22.8%; ED (n=177): worsening pneumonia symptoms 47.5% CAP aetiology: S. pneumoniae 44.1%, L. pneumophila 3.0%, H. influenzae 4.4%, anaerobes 5.6% Selection criteria: age: unselected (median (IQR) age 71 (55–79) years); severity: unselected (PSI >90 in 62.2%); comorbid disease: unselected; immune status: immunocompetent only (excluded HIV, splenectomy, immunosuppressive therapy, corticosteroid therapy equivalent to prednisolone >20 mg daily, neutropenia, Ig deficiency, solid organ transplant); other: excluded if inpatient death Adamuz [15] Spain January 2011–
October 2014Multicentre RCT 207 adults with CAP (male 59.9%) Healthcare utilisation at 30 days: primary care 20.3%, ED 18.4%; median (IQR) time off work: intervention group 30 (15–66.5) days, usual care group 26 (12.5–37) days CAP aetiology: S. pneumoniae 24.6%, H. influenzae 5.4%, influenzae A 3.4% Selection criteria: age: unselected (21–49 years: 20.2%; 50–69 years: 30.5%; >70 years: 49.3%); severity: unselected (CURB-65 0–1: 49.3%; CURB-65 2: 34.3%; CURB-65 ≥3: 16.4%); comorbid disease: excluded cognitive impairment; immune status: immunocompetent only (excluded HIV, splenectomy, immunosuppressive therapy, corticosteroid therapy equivalent to prednisolone >20 mg daily, neutropenia, Ig deficiency, solid organ transplant); other: excluded if nursing home resident or long-term care facility, language barrier Fine [19] USA/
CanadaOctober 1991–
March 1994Multicentre prospective cohort 1343 adults with CAP (male 52.4%) Proportion of patients reporting prevalence of symptoms and functional impairment at 30 days following discharge: cough 47.1%, dyspnoea 46.5%, sputum 42.3%, fatigue 72.6%, ≥1 symptom 68.5%; not returned to ADLs: workers 18% (median 15 days), nonworkers 42.8% (median 24 days); not returned to work 31.9% CAP aetiology: S. pneumoniae 9.1%, H. influenzae 4.8%, “atypical” 2.1%, Enterobacter sp. 2.8%, P. aeruginosa 0.9% Selection criteria: age >65 years 58.7%; severity: unselected (PSI I: 13.8%; PSI II: 17.4%; PSI III: 18.9%; PSI IV: 33.2%; PSI V: 16.7%); comorbid disease: unselected; immune status: excluded if HIV Marrie [21] Canada January 1998–
July 1998Multicentre prospective cohort 535 adults with CAP (male 52.3%) Proportion of patients reporting prevalence of symptoms/functional impairment at 14/42 days following discharge: cough 55.8%/35.3%, dyspnoea 48.6%/34.2%, chest pain 17.3%/11.6%, sputum 35.9%/26.4%, fatigue 66.7%/45.0%, fever 8.4%/4.7%, ≥1 symptom 85.6%/64.3% CAP aetiology: not reported Selection criteria: age: unselected (mean±sd age 61.6±19.1 years); severity: unselected (mean±sd PSI 76.2±32.8); comorbid disease: unselected; immune status: unselected Nickler [23] Switzerland October 2006–
March 2008Cohort from multicentre RCT 753 adults with CAP (male 58.8%) EQ-5D index: decline in ADLs in 29% at day 30 CAP aetiology: not reported Selection criteria: age: unselected (median (IQR) age 72 (52–82) years); severity: unselected (PSI I: 10.0%; PSI II: 19.7%); comorbid disease: excluded if terminal illness; immune status: immunocompetent only (excluded if long-term immunosuppression); other: excluded if language impairment precluding written consent, i.v. drug abuse Sharma [24] USA March 1995–
March 1998Single-centre prospective cohort 79 adults with CAP (male 35%) Proportion with decline in ADLs score of >1 point 28% at day 30 CAP aetiology: not reported Selection criteria: age: unselected (mean±sd age 79.9±6.1 years); severity: unselected (mean±sd PSI 106.2±23.9); comorbid disease: excluded if terminal illness; immune status: unselected; other: excluded if coma, intensive care admission, unable to participate in interview Uranga [25] Spain January 2012–
August 2013Multicentre RCT 312 adults with CAP (male 62.8%) Mean±sd CAP-symptom score at 5 days 24.7±11.4 to 27.2±12.5; mean±sd CAP-symptom score at 10 days 18.6±9.0 to 17.9±7.6; median (IQR) time for return to normal activity 15 (10–21) to 18 (9–25) days CAP aetiology: S. pneumoniae 16.0%, L. pneumophila 3.5%, H. influenzae 0.3% Selection criteria: age: unselected (mean±sd age 62.2±6.07 and 64.7±18.7 years in the control and intervention groups, respectively); severity: unselected (mean±sd PSI 83.7±33.7 and 81.8±33.8, in the control and intervention groups, respectively); comorbid disease: unselected; immune status: immunocompetent only (excluded if HIV, immunosuppression for solid organ transplantation, splenectomy, receiving ≥10 mg·day−1 prednisone equivalent for >30 days, taking other immunosuppressive agents, neutropenia); other: excluded if care home resident, antibiotics within preceding 30 days, intercostal chest drain, extrapulmonary manifestations, death or ICU admission prior to randomisation Wootton [26] UK February 2011–
March 2013Multicentre prospective cohort 169 adults with CAP (male 52%) Average CAP-symptom score 23.8 at day 2; average CAP-symptom score 13.6 at day 28; proportion of patients reporting prevalence of symptoms at 28 days following discharge: cough 13.6%, dyspnoea 67.1%, chest pain 31.2%, fatigue 57.0%, ≥1 symptom 96.4% CAP aetiology: not reported Selection criteria: age: unselected (mean±sd age 68 (range 16–98) years); severity: unselected (CURB-65 0–1: 46.7%; CURB-65 2: 29.6%; CURB-65 ≥3: 23.7%); comorbid disease: excluded if bronchiectasis, cystic fibrosis, advanced malignancy; immune status: unselected; other: excluded if palliative treatment, invasive ventilation Wyrwich [27] USA Unknown Multicentre retrospective cohort 201 adults with CAP (male 45%) Mean (median (IQR)) time to symptom resolution: cough 13.6 (7 (2–14)) days, dyspnoea 25.1 (14 (7–43)) days, chest pain 12.9 (7 (2–14)) days, sputum 14.8 (7 (7–14)) days, fatigue 25 (20 (7–24)) days, fever 2.7 (2 (1–2)) days; median time for return to work 14 days CAP aetiology: not reported Selection criteria: age: ≥50 years; severity: unselected; comorbid disease: unselected; immune status: unselected; other: respondent to e-mail survey, excluded if nursing home resident CAP: community-acquired pneumonia; RCT: randomised controlled trial; S. pneumoniae: Streptococcus pneumoniae; PSI: Pneumonia Severity Index; L. pneumophila: Legionella pneumophila; H. influenzae: Haemophilus influenzae; SF-36: Short Form-36 health survey; IQR: interquartile range; CURB-65: confusion, urea >7 mmol·L−1, respiratory rate ≥30 breaths·min−1, blood pressure <90 mmHg (systolic) or ≤60 mmHg (diastolic), age ≥65 years; P. aeruginosa: Pseudomonas aeruginosa; ICU: intensive care unit; ADLs: activities of daily living; ED: emergency department; EQ-5D: EuroQoL health-related quality of life questionnaire.
- TABLE 2
Summary of methodology of included studies
First author [ref.] Destination after initial review Severity Outcome measure Timing of assessment of outcome measure Assessment of symptoms Health status Assessment of function (return to) Clinical cure Healthcare utilisation IP OP CURB-65 PSI Prevalence CAP score CAP-symptom score SF-36 EQ-5D ADLs Occupation Primary care ED Average time to … ≤14 days 28 days 30 days 42 days Studies with participants selected for low/moderate severity CAP or age <65 years (n=6 studies, n=1217 individual participants) Bruns [6] ✓ ✓ ✓ ✓ ✓ ✓ Carratala [16] ✓ ✓ ✓ ✓ ✓ Daniel [17] ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ El Moussaoui [18] ✓ ✓ ✓ ✓ ✓ Laberere [20] ✓ ✓ ✓ ✓ ✓ ✓ Metlay [22] ✓ ✓ ✓ ✓ Studies where participants were unselected for severity or age (n=9 studies, n=4427 individual participants) Adamuz [14] ✓ ✓ ✓ ✓ ✓ ✓ Adamuz [15] ✓ ✓ ✓ ✓ ✓ ✓ ✓ Fine [19] ✓ ✓ ✓ ✓ ✓ ✓ ✓ Marrie [21] ✓ ✓ ✓ ✓ ✓ ✓ Nickler [23] ✓ ✓ ✓ ✓ Sharma [24] ✓ ✓ ✓ ✓ Uranga [25] ✓ ✓ ✓ ✓ ✓ ✓ Wootton [26] ✓ ✓ ✓ ✓ ✓ ✓ Wyrwich [27] ✓ ✓ ✓ ✓ ✓ IP: inpatient; OP: outpatient; CURB-65: confusion, urea >7 mmol·L−1, respiratory rate ≥30 breaths·min−1, blood pressure <90 mmHg (systolic) or ≤60 mmHg (diastolic), age ≥65 years; PSI: Pneumonia Severity Index; CAP: community-acquired pneumonia; SF-36: Short Form-36 health survey; EQ-5D: EuroQoL health-related quality of life questionnaire; ADLs: activities of daily living; ED: emergency department.
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERJ-02165-2018_Supplement










