





Abstract
The efficacy, safety and positioning of inhaled corticosteroids (ICS) in the treatment of patients with chronic obstructive pulmonary disease (COPD) is much debated, since it can result in clear clinical benefits in some patients (“friend”) but can be ineffective or even associated with undesired side effects, e.g. pneumonia, in others (“foe”). After critically reviewing the evidence for and against ICS treatment in patients with COPD, we propose that: 1) ICS should not be used as a single, stand-alone therapy in COPD; 2) patients most likely to benefit from the addition of ICS to long-acting bronchodilators include those with history of multiple or severe exacerbations despite appropriate maintenance bronchodilator use, particularly if blood eosinophils are >300 cells·µL−1, and those with a history of and/or concomitant asthma; and 3) the risk of pneumonia in COPD patients using ICS is higher in those with older age, lower body mass index (BMI), greater overall fragility, receiving higher ICS doses and those with blood eosinophils <100 cells·µL−1. All these factors must be carefully considered and balanced in any individual COPD patient before adding ICS to her/his maintenance bronchodilator treatment. Further research is needed to clarify some of these issues and firmly establish these recommendations.
Abstract
The use of inhaled corticosteroids in patients with COPD must be personalised http://ow.ly/ZyFI30lDfUR
Introduction
The efficacy, safety and positioning of inhaled corticosteroids (ICS) in the management of patients with chronic obstructive pulmonary disease (COPD) is much debated. Here, we review the evidence available for (“friend”) and against (“foe”) ICS use in COPD and propose that ICS, added to one or two long-acting bronchodilators (never as stand-alone medication), can benefit some (but not all) COPD patients. The challenge is to identify those patients with the highest benefit/risk ratio in clinical practice. Of note, this is not a systematic literature review, it is a narrative review based on the clinical experience and judgement of authors, supported by selected references.
Available evidence for and against the use of ICS in COPD
Many studies have explored the efficacy and safety of ICS in patients with COPD. Results depend on the characteristics of the population studied, the comparator treatment and the selected clinical outcome(s).
Exacerbations of COPD
Early randomised controlled trials (RCTs) did not show an effect of ICS monotherapy on exacerbations of COPD (ECOPD) rate/severity; although, since they investigated the potential effects of ICS on lung function decline, they were not enriched with patients at increased risk of ECOPD [1, 2].
Later RCTs of ICS/long-acting β2-agonist (LABA) combinations generally recruited patients with ≥1 ECOPD in the previous year, and showed that ICS/LABA combinations reduce ECOPD rates by approximately 25–35% compared with LABA monotherapy (figure 1) [3–14]. Likewise, despite not specifically focusing on patients at increased ECOPD risk, TORCH and SUMMIT were large enough to demonstrate ICS efficacy on ECOPD [15, 16]. More recently, two RCTs (IMPACT and TRIBUTE) compared triple therapy versus LABA/long-acting muscarinic antagonist (LAMA) combinations in patients at high ECOPD risk, and also showed a 15–25% reduction in ECOPD rates (figure 1) [17, 18].

Percentage reduction in the annual rate of moderate/severe exacerbations of chronic obstructive pulmonary disease (ECOPD) for the comparison inhaled corticosteroids (ICS)/long-acting β2-agonist (LABA) versus LABA (left) and for ICS/LABA/long-acting muscarinic antagonist (LAMA) versus LABA/LAMA (right) in published studies [3–5, 7–15, 17, 18]. *: p<0.05. #: significance could not be inferred because of hierarchy of statistical testing. Reference [6] is not included as rate ratios are not reported.
Another way to assess the efficacy of a given therapeutic option is the calculation of the number needed to treat (NNT). Person-based NNTs are often thought to be superior to event-based NNTs, as the latter is influenced by the reduction in ECOPD rate in patients with frequent exacerbations, rather than by the proportion of them with no ECOPD events. This, however, makes person-based NNTs less applicable in the real world where patients often have higher ECOPD rates than in tightly controlled RCTs [19]. Although neither IMPACT nor TRIBUTE includes NNTs in their published results [17, 18], values can be approximated from their respective publications. In IMPACT [17], the event-based NNT to prevent one ECOPD for triple therapy versus umeclidinium/vilanterol (UMEC/VI) with a 25% reduction in ECOPD lies between 3 and 4, whereas for triple therapy versus fluticasone furoate (FF)/VI, with a 15% reduction in ECOPD, it lies between 6 and 7. The corresponding person-based NNT is 25 for triple therapy versus UMEC/VI whereas, according to the Kaplan–Maier plot in the publication [17], there was no reduction in the number of patients with ECOPD for triple therapy versus FF/VI. In TRIBUTE [17, 18], with an overall low ECOPD rate (0.50 and 0.59 events per patient per year), a 15% reduction with beclometasone/formoterol/glycopyrronium (BDP/FF/G) versus indacaterol/glycopyrronium (IND/GLY) results in an event-based NNT between 11 and 12, and a person-based NNT of approximately 50. These figures compare quite favourably with other chronic treatments: for example, 5-year NNTs of 53 for statins to prevent one coronary heart disease event [20], and 24 for anti-hypertensives to prevent one cardiovascular disease event [21]. However, it is still important to consider that the calculation of event-based NNTs depends directly on the underlying rate of the event of interest (ECOPD in this case), so NNT is lower in frequent exacerbators and higher in those patients with only occasional ECOPD events.
The potential effect of triple therapy compared with LABA/LAMA or ICS/LABA on the rate of severe ECOPD (i.e. those leading to hospitalisation) is also clinically relevant. Neither IMPACT nor TRIBUTE were powered on this outcome [17, 18]. However, in IMPACT, the annual rates of severe ECOPD during treatment were 0.13 with triple therapy, 0.15 with FF/VI (13% difference; p=0.06), and 0.19 with umeclidinium (UMEC)/VI (34% difference; p<0.001) [17]. In TRIBUTE, the annual severe ECOPD rate was 0.07 in the beclometasone dipropionate/formoterol fumarate/glycopyrronium (BDP/FF/G) arm versus 0.09 in the indacaterol/glycopyrronium (IND/GLY) arm (21% difference; p=0.189) [18]. Whether the reduction of severe ECOPD with triple therapy versus LABA/LAMA, which was statistically significant in IMPACT, is also clinically relevant warrants confirmation in studies focusing on patients with recurring hospitalisations, since, both in IMPACT and TRIBUTE, the incidence of those events was quite low [17, 18, 22]. Finally, the use of a single inhaler for any ICS-containing combination therapy (ICS/LABA or ICS/LABA/LAMA) might improve a patient's adherence but, since available studies were not powered for this, it remains to be formally ascertained.
In summary, there is strong evidence that, in patients with previous ECOPD despite long-acting bronchodilator treatment, the addition of ICS reduces the risk of future ECOPD [23, 24].
Survival
Currently available information on the effects of ICS on survival in patients with COPD comes from three different sources: RCTs with mortality as the primary outcome, RCTs where mortality is a secondary or safety measure (not the primary outcome), and observational and registry studies.
RCTs with mortality as the primary outcome
Only two RCTs can be included in this category. 1) TORCH showed a 17.5% reduction in the risk of death in the ICS/LABA group versus placebo, but this difference just failed to reach statistical significance (HR 0.825 (95% CI 0.681–1.002); p=0.052) [15]. This result has been much debated, since a high placebo drop-out rate and statistical adjustment for an interim analysis might have impacted the ability to achieve a p-value <0.05 [25]; with the given absolute risk reduction of 2.6%, NNT would be 38. In a pre-specified secondary analysis, both the Cox model and Log-rank test suggested a mortality benefit to the ICS/LABA arm versus placebo [15]. 2) SUMMIT, which selectively recruited COPD patients with moderate airflow limitation and heightened cardiovascular risk, did not show a mortality risk reduction for ICS/LABA versus placebo (HR 0.88 (0.74–1.04); p=0.137) [16].
RCTs with mortality as a secondary outcome
Three analyses can be included in this category. 1) In INSPIRE, ICS/LABA was associated with reduced mortality versus LAMA therapy (3% versus 6%; p=0.032) [26]. 2) In IMPACT, ICS-containing treatments were associated with lower mortality versus LABA/LAMA (triple versus LABA/LAMA: HR 0.58 (0.38–0.88); p=0.01; ICS/LABA versus LABA/LAMA: 0.61 (0.40–0.93); p=0.02) [17, 27]. Of note, however, patients with a previous history of asthma could be enrolled in IMPACT and this may have influenced results. Using the reported mortality rates, the NNT in IMPACT would be 256. 3) A post hoc analysis of pooled data from TRILOGY, TRINITY and TRIBUTE showed a non-significant reduction in the hazard ratio of fatal events for ICS-containing versus ICS-free treatments (triple versus LAMA or LABA/LAMA: HR 0.72 (0.49–1.06); p=0.096) [28]. The estimated NNT in this pooled analysis, with the calculations based on the proportion of patients and not taking time to event into account, would be 141.
Observational and registry studies on the effects of ICS on mortality
The results of these studies suggest reduced mortality in patients receiving ICS-containing therapy, mostly after discharge from hospitalisation due to ECOPD [29–33]. Although they are not RCTs, their results can be clinically relevant since patients included in these studies are more likely to be elderly, multi-morbid, frail, and at high risk of re-hospitalisation and death [34, 35]. However, registry studies can have significant biases [36], including immortal time bias [30, 31], immeasurable time bias [32, 37] and “asthma” bias [38], although it is important to note that none of these potential biases has been proven to be the real explanation for the observed benefits of ICS in this population, so the latter may still represent real clinical differences. Importantly, no “real world” study on mortality in patients with COPD has optimised the treatment of other concomitant disorders that are almost invariably present in these patients, including heart failure, coronary artery disease, stroke, diabetes and hypertension, whose appropriate treatment reduces mortality [35, 39, 40].
In summary, currently available evidence from RCTs fails to show that the addition of ICS to long-acting bronchodilator therapy improves survival significantly in patients with COPD. However, secondary or safety analyses of RCTs and observational data suggest that certain subtypes of COPD patients may benefit, particularly those with severe airflow limitation and/or frequent exacerbations. Further prospective research is needed to confirm or refute this clinically relevant possibility.
Health-related quality of life
Many previous studies [13, 17, 18, 41] have shown that ICS therapy improves health-related quality of life (HRQoL), as measured by the St George's Respiratory Questionnaire (SGRQ) total score, but the effect size (1.5–2.5 units) is lower than the minimal clinically important difference (4 units) [42]. However, there is controversy regarding the use of this four-unit threshold to compare active treatments [43–45]. In the case of ICS, there is significant inter-individual response variability [18], which is likely to influence the proportion of SGRQ “responders” versus “non-responders” [46]. With this caveat in mind, in IMPACT, 42% of participants responded (i.e. improved their SGRQ total score from baseline by more than 4 units) to triple therapy, whereas 34% responded to ICS/LABA or LABA/LAMA [17]. This means that, for every 100 patients treated with triple instead of one of the two dual combinations, an extra eight patients would have a clinically relevant improvement in SGRQ, which results in an NNT of approximately 13. Whether this benefit is driven by fewer ECOPDs is unclear but possible, since ECOPD events worsen SGRQ total scores, and in some individuals there is a long recovery time (many months) to return to the baseline value [47]. An alternative explanation is that the ICS anti-inflammatory effect in the stable state improves lung function and thereby contributes to a symptomatic improvement.
In summary, the effects of ICS on HRQoL vary significantly between patients; identifying and validating markers of HRQoL response in COPD remains a challenge.
Lung function
In studies lasting 6–12 months, the addition of ICS to a bronchodilator improved forced expiratory volume in the first second (FEV1) in the range of 30–90 mL [3, 4, 6, 8, 9, 11–14]. Yet, longer RCTs (3-year) with FEV1 decline as the primary outcome failed to show a significant effect from ICS monotherapy [1]. This may not be surprising, given that the rate of FEV1 decline varies greatly among patients with treated COPD [48, 49], and that there are different FEV1 trajectories leading to COPD [50]. However: 1) a post hoc analysis of TORCH showed a reduction in FEV1 decline in patients treated with ICS versus placebo (difference 13.0 mL·year−1; p=0.003) but not versus LABA (difference 3.3 mL·year−1; p=0.441) [51]; 2) in a pre-specified analysis of FEV1 decline as a secondary outcome in SUMMIT, treatment with ICS, either alone or in combination with a LABA, was associated with a 8 mL·year−1 reduction in FEV1 decline [16, 52], similar to that seen in a previous meta-analysis [53]; 3) a factorial analysis of SUMMIT suggested that the ICS component drives the improvement in FEV1 decline, whereas the effect on ECOPD reduction appears additive (ICS and LABA) [54]; 4) a post hoc analysis of FEV1 decline in ISOLDE reported a more pronounced effect of ICS in patients with higher eosinophils [55]; 5) in the GLUCOLD study, for which bronchial biopsies were obtained at baseline and during therapy with ICS/LABA or placebo, gene expression differed between those who had a significant increase in FEV1 over the duration of the study versus those whose lung function declined over the same period [56]; and, finally 6) meta-analyses of 3-year trials provide conflicting results [53, 57, 58].
In summary, the effects of ICS on lung function vary between COPD patients and are numerically small.
Infections
ICS can impair monocyte chemotaxis, bactericidal activity, interleukin (IL)-1 and tumour necrosis factor α production, and T-cell activation [59, 60], thereby increasing the risk of respiratory infections such as pneumonia [15], oropharyngeal candidiasis [61–63], mycobacterial [64, 65] and upper respiratory tract (URTIs).
Pneumonia
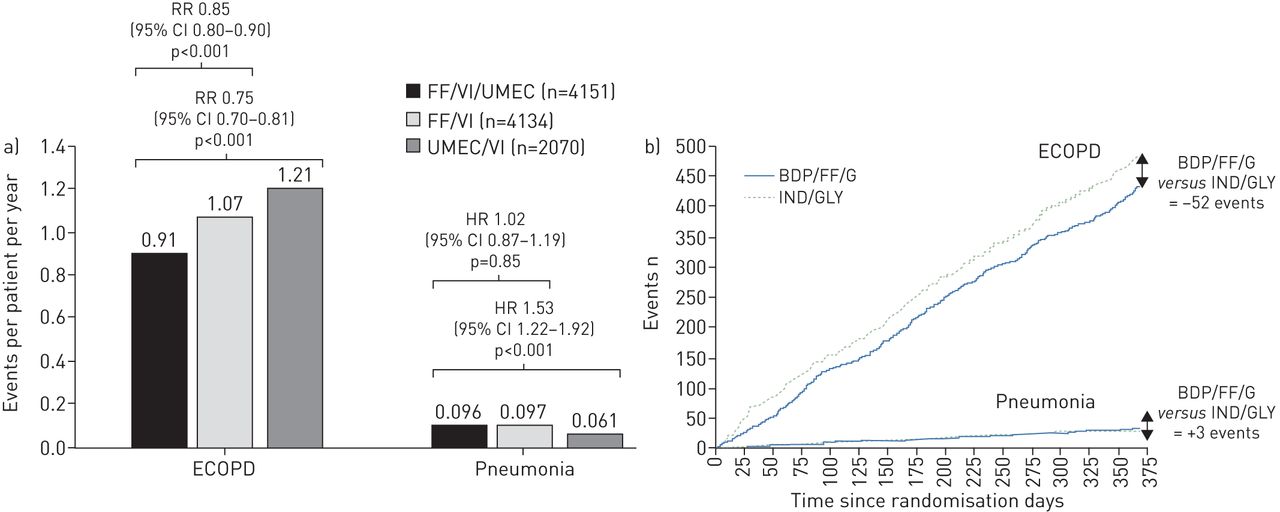
The risk of pneumonia in both smokers and patients with COPD is increased regardless of ICS use [66, 67] but ICS treatment further increases this risk [7, 13, 15, 26, 68–73], as acknowledged in 2016 by the Pharmacovigilance Risk Assessment Committee of the European Medicines Agency [74]. This is the case regardless of whether pneumonia events are reported based on a clinical diagnosis or chest radiograph [12, 18, 68]. More recently (in 2018), the incidence of pneumonia associated with single-inhaler triple therapies has been compared with that associated to treatment with ICS/LABA, LABA/LAMA or LAMA [17, 18, 75, 76]. In IMPACT, the incidence of pneumonia was higher in patients treated with FF/VI/UMEC than UMEC/VI (8% versus 5%; figure 2a) [17] whereas, in TRIBUTE, BDP/FF/G was not associated with a higher incidence of pneumonia when compared with IND/GLY (4% with each; figure 2b) [18, 77]. Likewise, in SUMMIT, the risk of pneumonia was not increased by ICS therapy [16, 78].

Effect of different pharmacological combinations on exacerbations of chronic obstructive pulmonary disease (ECOPD) and pneumonia both in the a) IMPACT [17] and b) TRIBUTE [77] studies (reproduced with permission from the authors). Note that in panel a, all bars indicate the incidence of events (as events per patient per year) but ECOPD results are shown as RR values, whereas those of pneumonia are shown as HR values for time to first event. In panel b, all lines indicate incidence of events. FF: fluticasone furoate; VI: vilanterol; UMEC: umeclidinium; BDP/FF/G: beclometasone dipropionate, formoterol fumarate and glycopyrronium; IND/GLY: indacaterol and glycopyrronium.
Differences in pneumonia incidence/risk may be due to: 1) differences in study design or adverse event reporting [79, 80]; 2) characteristics of the population studied, such as older age (≥55 years versus <55 years, HR 1.62 (1.21–2.15) [81]; ≥65 years, ICS/LABA versus LABA HR 3.3 (1.2–8.7) [79]), lower BMI (<25 kg·m−2, ICS/LABA versus LABA HR 3.4 (1.4–8.4) [79, 81]), more severe airflow limitation (FEV1 30–50% predicted, ICS/LABA versus LABA HR 2.9 (1.1–8.0) [79, 81]), frequent ECOPD (≥1 versus 0 HR 1.25 (1.08–1.45) [81]) and low blood eosinophil counts [82–84], although this has not been observed in all studies [85]; 3) higher ICS doses, although available evidence on this topic is not conclusive since head-to-head comparisons of different ICS doses in RCT are rare and available data do not show a dose-related increase in the pneumonia risk for FF/VI or for fluticasone propionate/salmeterol (FP/SAL) [79, 86]. Furthermore, indirect comparisons between studies of high versus medium/low ICS doses are difficult due to differences in design, specific drugs tested, previous treatments and/or severity of airflow limitation. Yet, the incidence of pneumonia increases even when medium doses of ICS (250 µg) are used (7% FP/SAL versus 2% SAL [10]; 7% FP/SAL versus 4% SAL [8]) and, importantly, patients receiving ≥1000 µg·day−1 of FP equivalent were at the greatest risk (RR 2.25 (2.07–2.44)) [87]; and/or 4) different ICS molecules [79, 80]. The event-based number needed to harm (NNH) was 33 for FP in TORCH [15] and 34 for FF in IMPACT [17]. For budesonide, the risk of pneumonia seems to be lower, although the budesonide studies were shorter, and so are less precise [79, 80]. In fact, a Cochrane review concluded that both budesonide and fluticasone are associated with increased risk of serious adverse pneumonia events requiring hospitalisation [73]. Event-based NNH estimates for BDP are approximately 50 for BDP/FF versus FF in FORWARD and 120 for BDP/FF/G versus tiotropium in TRINITY, but cannot be calculated for TRIBUTE as there was no difference between triple and LABA/LAMA [13, 18, 75].
On a final note, it is unclear whether the occurrence of ICS-associated pneumonia increases mortality in patients with COPD [15, 87–89]. Retrospective/cohort studies that assessed mortality in subjects with COPD hospitalised with pneumonia in relation to previous ICS treatment reported conflicting results [87, 90, 91]. A Canadian study reported that the risk of pneumonia hospitalisation followed by death was increased in patients receiving ICS versus control, with the rate ratio of hospitalisation being highest in those receiving high-dose ICS (≥1000 µg FP equivalent). However, 30-day all-cause mortality was not increased [87]. In contrast, two large retrospective studies reported that prior receipt of ICS was associated with decreased mortality at 30 days and 90 days (OR 0.80 and 0.78, respectively) in ICS treated patients hospitalised for pneumonia [90, 91]. However, a RCT assessing pneumonia-related deaths was not conclusive likely due to the low frequency of events reported [73].
In summary, the use of ICS in COPD increases the risk of pneumonia, particularly in patients with older age, lower BMI, severe airflow limitation and low blood eosinophil counts [81, 82].
Mycobacteria
Observational studies suggest that patients with COPD receiving treatment with ICS have an increased risk of active tuberculosis in high prevalence areas, such as South Korea (RR 1.84 (1.56–2.17)) [92] and Taiwan (HR 4.74 (1.01–22.37) for high ICS doses) [93]. Yet, a similar trend has been reported in settings with low tuberculosis prevalence, such as Canada [94]. Further, these observations have been supported by meta-analyses of data from RCTs [65]. The risk of tuberculosis seems particularly pronounced in older males with a history of previous hospitalisations for COPD and in those with more severe lung function impairment [95]. The ICS dose associated with increased tuberculosis risk was >500 µg·day−1 FP or equivalent in the study from Taiwan [93].
In case–control studies, COPD has been identified as a risk factor for infection with non-tuberculous mycobacteria (NTM), with a ICS dose-related increased risk [96]. A Canadian database analysis confirmed the increased risk of NTM pulmonary disease among patients with COPD treated with ICS-containing medications (OR 2.09 (1.80–2.43)) with a dose–response relationship for yearly cumulative dose of FP, but not budesonide [97].
Viruses
Long-term ICS use increases URTI risk, including rhinovirus, respiratory syncytial virus and coronavirus [98]. The association is particularly significant in patients receiving high ICS doses, and appears more consistent with FP [98]. A meta-analysis of 26 trials showed that the risk of influenza was not significantly increased in patients with COPD who were receiving ICS; however, there was a statistically significant difference when only the FP studies were considered [65].
Candidiasis
An observational, matched cohort study showed that patients receiving ICS/LABA had significantly greater odds of experiencing oral thrush than those prescribed LABA alone, with a dose-dependent effect for FP/SAL [63]. RCTs have also reported an increased risk of oropharyngeal candidiasis with ICS (OR 2.65 (2.03–3.46)) [99].
ICS withdrawal
Several studies have investigated the impact of ICS withdrawal in patients with COPD with contrasting results. Potential confounders include study design (observational versus RCT), severity of airflow limitation of the patients studied, outcomes assessed, duration of follow up, background inhaled treatment (placebo versus long-acting bronchodilator(s)), definition and previous history of ECOPD, and/or duration of run-in and/or wash-out periods [100].
The ISOLDE trial was the first to report an increased rate of ECOPD following acute ICS withdrawal (during the run-in period) in patients previously treated with ICS, compared with patients never treated with ICS [101]. Similarly, O'Brien et al. [102] reported a statistically non-significant increase in ECOPD rate after ICS withdrawal in a six-week RCT which was accompanied by a 100-mL FEV1 decrease. The COPE study showed that the hazard ratio of a first ECOPD episode in patients who discontinued ICS was 1.5 compared with those continuing ICS [103]. The COSMIC study, which included patients with moderate-to-severe COPD with at least two ECOPD in the previous year, showed that ICS withdrawal resulted in a prompt and persistent decrease in FEV1 of about 4% and an increase in respiratory symptoms, although no significant differences in the rate of moderate or severe ECOPD between groups was observed during the subsequent year [104]. Another RCT in patients in primary care in the UK reported an almost 50% increased risk of ECOPD over 1 year following ICS withdrawal [105]. A systematic review of these three early RCTs [103–105] concluded that, although outcomes were generally worse for patients in whom ICS was withdrawn, differences were mostly small and not statistically significant [106].
The WISDOM study was the first RCT specifically designed to investigate the effects of a stepped ICS withdrawal on the frequency of ECOPD and rate of FEV1 decline in a large population of severe COPD patients with ≥1 ECOPD in the previous 12 months, with all patients receiving triple therapy during the 6-week run-in period ICS withdrawal did not increase the risk of moderate or severe ECOPD but was again associated with a reduction in FEV1 [107, 108]. The interpretation of these data may be clouded by the fact that only 39% of patients were on triple therapy before inclusion, which could favour a lack of effect of ICS withdrawal.
The “real life” DACCORD study reported no increased risk of ECOPD in patients with COPD managed in the primary and secondary care during 2 years after ICS withdrawal [109]. The GLUCOLD study group reported accelerated lung function decline in patients with moderate COPD after ICS discontinuation over a 5-year follow up [110]. Of note, in this biopsy study, ICS withdrawal resulted in increased airway inflammation [111]. Finally, the INSTEAD study suggested that in patients with moderate COPD and no history of ECOPD, ICS could be discontinued safely; however, it should be noted that follow-up in this study lasted only for 26 weeks [112]. This was recently confirmed in the SUNSET study, in which direct de-escalation from long-term triple therapy to LABA/LAMA in patients without frequent ECOPD episodes led to a small decrease in lung function, with no difference in ECOPD [113, 114].
In summary, ICS withdrawal results in a slight but consistent deterioration of lung function (FEV1) and airway inflammation, whereas the effects upon the rate of ECOPD varies across studies, likely in relation to the type of patients studied (high versus low blood eosinophils), concurrent bronchodilation maintenance therapy and previous history of ECOPD.
Personalised ICS treatment in COPD
From the evidence reviewed above, it seems clear that some COPD patients may benefit from the addition of ICS to their long-acting bronchodilator maintenance treatment whereas others don't. Thus, the risk/benefit ratio of adding (or withdrawing) ICS has to be carefully considered in each individual patient. The challenge is, therefore, how to identify what markers can help to identify in the clinic those COPD patients who can benefit most from ICS use at the lowest risk possible of undesired side effects (table 1).
Factors to consider when initiating inhaled corticosteroids (ICS) treatment (in combination with one or two long-acting bronchodilators) in chronic obstructive pulmonary disease (COPD) patients (the scenario is different when considering ICS withdrawal; see text)
Clinical markers of potential ICS benefit
To ascertain which patients with COPD can benefit more from the addition of ICS to their maintenance long-acting bronchodilator treatment it is important to define what is the specific outcome that we want to target. 1) Death: currently available evidence from RCTs does not support that the addition of ICS improves mortality in COPD patients. Yet, secondary analyses and observational data suggest a potential beneficial effect in certain subgroups, particularly in those with severe disease, frequent exacerbations [15–17], and/or history of (or concomitant) asthma [115], albeit this has never been confirmed in a formal RCT [116]. While waiting for further prospective research to confirm or refute this possibility, if the therapeutic target is survival, it seems advisable to use clinical judgment to balance the benefit/risk ratio of adding/avoiding ICS in individual patients. 2) Rate of ECOPD: available evidence here is clear, ICS are indeed effective at all stages of airflow limitation [17, 18, 70, 117]. 3) HRQoL: the response to the addition of ICS varies significantly between patients [118]. 4) Lung function decline: older patients, current smokers, patients with more severe airflow limitation and lower BMI will benefit less [51].
Clinical markers of potential ICS risk
Factors associated with an increased risk of pneumonia in patients with COPD treated with ICS include older age (>55 years), BMI <25 kg·m−2, greater severity of airflow limitation (FEV1 30–50% predicted), prior ECOPD history and low blood eosinophil counts [72, 81]. Thus, in clinical practice, it seems advisable to discontinue ICS if repeated episodes of pneumonia are documented (albeit there is no proof of increased risk of death from these pneumonias [79, 119]). Analyses of large databases also suggest that ICS use in COPD is associated with increased risk of diabetes (RR 1.34 (95% CI 1.29–1.39)) [120, 121], particularly with the highest ICS doses (≥1000 µg per day fluticasone equivalent; RR 1.64 (1.52–1.76)) [120, 121], cataract (current ICS users had twice the risk of incident posterior subcapsular cataract; OR 2.5 (1.3–4.7)) or incident nuclear cataract (OR 2.0 (1.2–3.4)) [122] and osteoporosis/fractures (OR 1.21 (1.12–1.32) ICS current or ever users versus non-users) [123, 124], so these potential undesired side effects need to be monitored in clinical practice. Finally, it is important to consider that the dose or specific type of ICS molecule used may also influence the risk for undesired outcomes [119, 125].
Blood eosinophils to guide ICS use in COPD
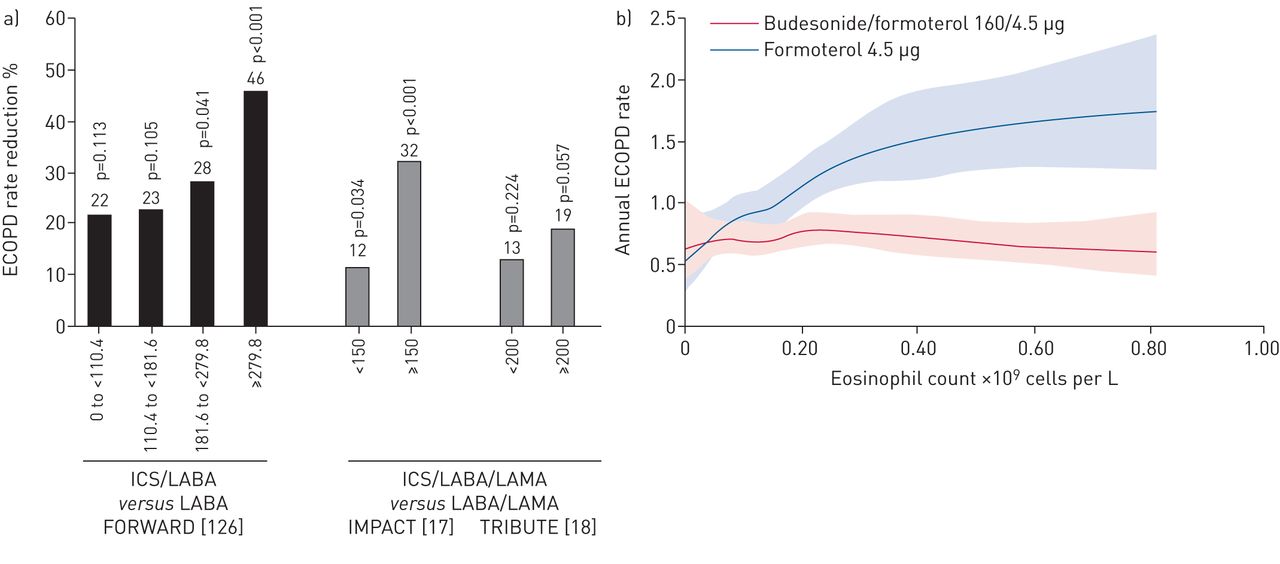
There is an emerging pattern that suggests that blood eosinophil levels can be a potentially useful biomarker to identify those patients with COPD in whom the addition of ICS to their long-acting maintenance therapy is more likely to reduce the risk of future exacerbations. Although no RCT has yet explored directly the response to ICS in this type of patients according to their blood eosinophil levels, the following observations do support this pattern. 1) Post hoc analyses of RCTs comparing ICS/LABA versus LABA showed that, in patients treated with LABA only, the ECOPD rate was higher in those patients with higher blood eosinophil counts, and that ICS prevent future ECOPD most effectively in such patients (figure 3a) [17, 126]; 2) two recent RCTs of triple therapy versus LABA/LAMA (IMPACT and TRIBUTE) pre-specified the analysis of blood eosinophils to determine the level of response to the investigated therapies and confirmed greater ICS effects in patients with ≥150–200 eosinophils·µL−1 [17, 18]; 3) the FLAME study showed fewer moderate-to-severe exacerbations with LABA/LAMA treatment compared to ICS/LABA (17% treatment difference) [68], with a post hoc analysis showing that the lowest response to ICS/LABA was in patients with <150 eosinophils·µL−1 [127]; 4) ICS withdrawal in WISDOM caused increased ECOPD in patients with ≥300 eosinophils·µL−1 [128, 129]; and 5) using continuous negative binomial regression modelling, a threshold of ≥100 eosinophils·µL−1 appeared to predict a positive ICS response, with greater effect sizes at higher eosinophil counts (figure 3b) [130].
{kind=link}
{kind=link}
{kind=link}
Influence on the relative effect of inhaled corticosteroids (ICS)-containing versus non-ICS-containing therapies on annualised exacerbations of chronic obstructive pulmonary disease (ECOPD) rates at different eosinophil levels: a) percentage of ECOPD rate reduction in FORWARD [126], IMPACT [17] and TRIBUTE [18] by blood eosinophil levels; b) pooled analysis of three studies comparing ICS/long-acting β2-agonist (LABA) versus LABA showing ECOPD incidence by eosinophil level (reproduced from [130] with permission from the publisher).
Alternatively, there are arguments against the use of blood eosinophils as a clinically useful biomarker of ICS response in COPD. 1) The relationship between blood and sputum eosinophils is poor or absent [131–133]. However, sputum eosinophils are prone to variability, and bronchoscopic sampling reported more eosinophilic airway inflammation in those patients with COPD who had higher blood eosinophil counts [134]. 2) Blood eosinophils show variability, particularly when using higher (e.g. 300 eosinophils·µL−1) than lower (e.g. 100 eosinophils·µL−1) thresholds [83, 135, 136]. 3) Some observational cohort studies have found no association between systemic eosinophil levels and outcomes, including exacerbations, hospitalisations and mortality, while others did [137, 138]. 4) Finally, recent studies have shown that the IL-5 antibody mepolizumab nearly eliminate circulating eosinophils yet influence ECOPD modestly [139]. However, this does not exclude the possibility that blood eosinophils may be a biomarker of other biological processes (not necessarily an effector molecule) that favour ICS benefit (e.g. less bacterial colonisation or different T-helper 2 biology). Further studies are needed to elucidate these possibilities.
Considering all these pro–con arguments, we propose the following practical strategy for the addition/avoidance of ICS in individual patients with COPD who still suffer frequent ECOPD episodes despite appropriate bronchodilator therapy: 1) given that <100 eosinophils·µL−1 seems a useful and reproducible threshold to predict a poor response to ICS in terms of ECOPD prevention, we would suggest limiting their use in these patients, unless the individual patient has a history of asthma; 2) alternatively, because >300 eosinophils·µL−1 seems to predict a beneficial ICS response in terms ECOPD risk reduction [130, 137], we would support the addition of ICS to long-acting bronchodilator therapy in those patients who still experience ECOPD despite appropriate bronchodilator treatment; and, finally, 3) there is an intermediate group of patients, with 100–300 eosinophils·µL−1, for whom current evidence is insufficient to make a firm recommendation. In this group, a careful consideration of the potential benefits and risks discussed above should be individually considered. Needless to say that this strategy must be validated in prospective studies. The role of other biomarkers to predict ICS response in COPD remains unknown and requires further research.
Conclusions
Since ICS in COPD can be both “friend” and “foe”, their addition to long-acting bronchodilator maintenance therapy in these patients must be personalised. To this end, a number of clinical and biological markers related to their benefits and risks (table 1) can help clinicians to decide on their use in an individual patient.
Footnotes
Disclaimer: Most authors of this review are (or have been) members of the Global Initiative for Chronic Obstructive Lung Disease (GOLD) Scientific Committee; the content of this paper reflects their views, not necessarily those of GOLD.
Conflict of interest: A. Agusti reports receiving grants from GSK; lectures fees from Novartis and Chiesi; grants, and lecture and advisory board fees from AstraZeneca; and lecture and advisory board fees from Boheringer Ingelheim, all outside the submitted work.
Conflict of interest: L.M. Fabbri reports being paid for lectures and membership of advisory boards, and receiving travel expense reimbursement and grants for research from Boehringer Ingelheim, Chiesi, GSK, Merck Sharp & Dhome, Takeda, AstraZeneca, Novartis, Menarini, Laboratori Guidotti and Almirall; being paid for lectures and membership of advisory boards, and receiving travel expense reimbursement from Pearl Therapeutics, Mundipharma, Boston Scientific and Zambon; being paid for lectures by Kyorin and Bayer; and has received grants for research from Pfizer, Dompe, Malesci, Biofutura Italia and Vree Health Italia.
Conflict of interest: D. Singh reports grants and personal fees from Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Glenmark, Johnson and Johnson, Merck, NAPP, Novartis, Pfizer, Takeda, Teva, Therevance, and Verona; and personal fees from Genentech and Skyepharma, all outside the submitted work.
Conflict of interest: J. Vestbo reports receiving personal fees for consultancy on COPD phase 2 and 3 programmes, and payment for lectures including service in speaker bureau, from GlaxoSmithKline, Chiesi Pharmaceuticals, Boehringer Ingelheim, Novartis and AstraZeneca, outside the submitted work.
Conflict of interest: B. Celli reports personal fees and funding for a research site from AstraZeneca, and consulting fees from GlaxoSmithKline, Boehringer Ingelheim, Novartis, Chiesi and Menarini, all outside the submitted work.
Conflict of interest: F.M.E. Franssen reports receiving personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline and Teva; and grants and personal fees from Novartis, all outside the submitted work.
Conflict of interest: K.F. Rabe reports receiving consultancy and speaker fees from AstraZeneca, Boehringer Ingelheim, Novartis, Sanofi, Teva, Intermune, Chiesi Pharmaceuticals and Berlin Chemie; and grants from Ministry of Education and Science, Germany, outside the submitted work.
Conflict of interest: A. Papi reports receiving fees for board membership, consultancy, payment for lectures, grants for research, travel expense reimbursement from Chiesi, Astrazeneca, GlaxoSmithKline, Boehringer Ingelheim, Mundipharma, and TEVA; payment for lectures and travel expense reimbursement from Menarini, Novartis and Zambon; and grants for research from Sanofi, all outside the submitted work.
Support statement: Editorial support was provided by David Young of Young Medical Communications and Consulting Ltd, which was funded by the Consorzio Futuro in Ricerca of Ferrara, Italy. Jørgen Vestbo and Dave Singh are supported by the NIHR Manchester Biomedical Research Centre.
- Received June 30, 2018.
- Accepted August 23, 2018.
- Copyright ©ERS 2018
References










