





Abstract
Blood eosinophil count in chronic obstructive pulmonary disease (COPD) is associated with higher exacerbation rate and favourable response to corticosteroids; however, frequent exacerbations and use of inhaled corticosteroids could elevate pneumonia risk. We tested the hypothesis that high blood eosinophil counts are associated with high risk of pneumonia in individuals with severe COPD from the general population.
We included 7180 individuals with COPD from the Copenhagen General Population Study, including 643 with forced expiratory volume in 1 s (FEV1) <50% predicted between 2003 and 2011. All primary discharge diagnoses of pneumonia during follow-up were recorded.
Among individuals with COPD and FEV1 <50% pred, the multivariable adjusted incidence rate ratio was 2.17 (95% CI 1.31–3.58) for pneumonia comparing individuals with blood eosinophil counts ≥0.34×109 cells·L−1 versus <0.34×109 cells·L−1. In individuals with clinical COPD, defined by recent exacerbation, ≥10 pack-years of smoking and FEV1 <70% pred, the corresponding risk was 4.52 (2.11–9.72). Risk of pneumonia did not differ by blood eosinophil count in individuals with COPD and FEV1 ≥50% pred.
In individuals with COPD and FEV1 <50% pred, blood eosinophil count ≥0.34×109 cells·L−1 was associated with high risk of hospitalisation due to pneumonia.
Abstract
Eosinophilic COPD with severely impaired lung function is associated with high risk of pneumonia hospitalisations http://ow.ly/Tyl130jsi1D
Introduction
The risk of pneumonia is elevated in individuals with chronic obstructive pulmonary disease (COPD) [1, 2]; and high age, comorbidity, a history of exacerbations and severe disease with reduced forced expiratory volume in 1 s (FEV1) have all been identified as risk factors for the development of pneumonia in COPD [2, 3]. Furthermore, therapy with inhaled corticosteroids (ICS) in COPD is associated with an elevated risk of pneumonia [4–6] and possibly excess pneumonia deaths [7]. Retrospective analyses have not reported a difference in pneumonia incidence according to the levels of blood eosinophils in patients with COPD [8], but a recent post hoc meta-analysis of clinical trials found that COPD patients with blood eosinophil counts <2% had more pneumonia events compared to patients with higher blood eosinophil counts [9]. In addition, some studies suggest that there may exist an inverse relationship between sputum eosinophil count and sputum bacterial count [10].
The peripheral blood eosinophil counts correlate with sputum eosinophil counts in patients with COPD, and thus blood eosinophil count is emerging as a biomarker of eosinophilic airway inflammation [11, 12]. Although reports of higher readmission rates in COPD patients with increased blood eosinophil counts at hospitalisation are conflicting [13, 14], previous studies have found that blood eosinophil counts are associated with future risk of exacerbations. Using a cut-point for eosinophils of ≥2% of total blood leukocytes or a cut-point in absolute number of 0.34×109 cells·L−1, these studies suggest that an elevated blood eosinophil count is associated with a higher risk of COPD exacerbations [8, 15, 16].
Although controversial [17], high blood eosinophil counts in COPD probably marks a phenotype associated with frequent exacerbations, which could influence the risk of pneumonias, and we speculated that high blood eosinophil counts may mark high risk of pneumonia in individuals with COPD. As pneumonias leading to hospitalisation are rare in mild to moderate COPD, we tested the hypothesis that a blood eosinophil count of ≥0.34×109 cells·L−1 in individuals with COPD ranging in severity as assessed by FEV1 % predicted was associated with high risk of being hospitalised due to pneumonia. Furthermore, using the same cut-point in blood eosinophils, in addition we tested whether a high blood eosinophil count was associated with high risk of pneumonias in individuals with clinical exacerbating COPD [16] defined by recent exacerbation, ≥10 pack-years and FEV1 <70% pred. For this purpose, we studied individuals with COPD from the Copenhagen General Population Study (CGPS), all with baseline measurements of blood eosinophil counts, and followed these up to 8 years for development of pneumonia in a prospective study design.
Methods
Copenhagen General Population Study
The CGPS is a prospective study of the general population residing in Greater Copenhagen [18–20] with ongoing recruitment begun in 2003. All participants performed spirometry and we defined COPD as a ratio of FEV1/forced vital capacity (FVC) <0.7 and less than the lower limit of normal, excluding individuals with self-reported asthma. We further subdivided the COPD population according to Global Initiative for Chronic Obstructive Lung Disease (GOLD) grade 1–2, and GOLD grade 3–4; that is, FEV1 ≥50% pred and <50% pred. Within the COPD population, we defined a subpopulation with clinical COPD based on the following criteria: at least one exacerbation in the year prior to baseline, ≥10 pack-years of smoking and FEV1 <70% pred, as done previously [16]. From 81 107 individuals from the CGPS, we identified 7180 individuals with COPD with full information on spirometry and blood biomarker measurements; of these, 4832 had smoked >10 pack-years.
Information on the use of ICS was obtained by linking CGPS to the national Danish Registry of Medicinal Products Statistics, which records all prescriptions dispensed in Danish pharmacies.
Blood eosinophil counts
Blood eosinophil counts were measured in fresh blood samples using the ADVIA 120 haematology system (Siemens Healthineers, Erlingen, Germany) and reported in total numbers (×109 cells·L−1). We defined high versus low eosinophil counts in individuals with COPD as blood eosinophil counts of ≥0.34×109 cells·L−1 versus those <0.34×109 cells·L−1, as determined in our previous work on blood eosinophil counts and COPD exacerbations [16]. However, in sensitivity analyses we used blood eosinophil cut-points of 2% of all leukocytes, which has been widely used [15], and 3.3%, determined in our previous work [16].
Pneumonia
Risk of pneumonia was analysed prospectively. We defined pneumonia events as a hospital admission with a primary discharge diagnosis of pneumonia (World Health Organization International Classification of Diseases code J12–J18). Information on diagnoses was drawn from the national Danish Patient Registry, which records all hospital contacts in Denmark, and linked to the CGPS. Prior pneumonia events were defined in the same manner as pneumonias during follow-up, but with an admission date before the date of examination in the CGPS.
Statistical analysis
Analyses were performed using STATA/SE software (version 14.1; StataCorp, College Station, TX, USA).
A negative binomial regression model with 95% confidence intervals was used to compare risk of pneumonias during follow-up. Analyses were multivariable adjusted for sex, age, smoking status, pack-years of smoking, body mass index, education and FEV1 % pred. Potential confounders were pre-specified and included, irrespective of their contribution to the model. A nested model with and without blood eosinophil counts was tested using a likelihood ratio test. Additionally, we included use of ICS in the year prior to baseline, and inflammatory biomarkers high sensitivity C-reactive protein, fibrinogen and total leukocytes as confounders, as these have previously been associated with the risk of pneumonia in COPD [21]. Follow-up began at study entry and ended at death (n=583), emigration (n=8) or end of follow-up (December 31, 2011), whichever came first. We tested for interaction of blood eosinophil counts and ICS use and risk of pneumonias using the likelihood-ratio test.
Imputation of missing covariates at baseline for adjustments in the multivariable adjusted analyses was done by multivariable regression. However, analyses only including individuals with full information on covariates gave similar results to those reported.
Additional details on the methods are provided in the online supplementary material.
Results
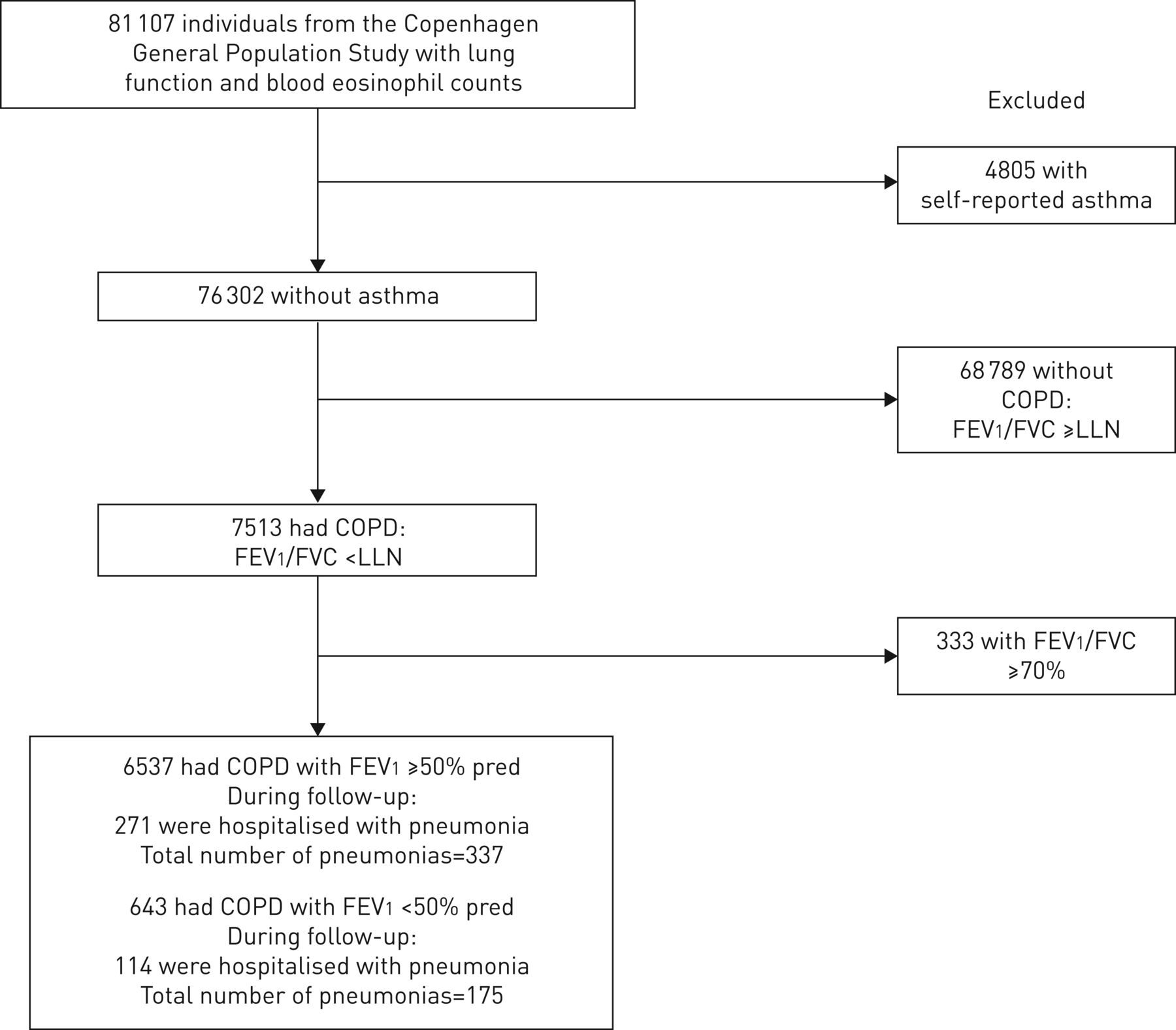
We included 7180 individuals with COPD (figure 1). Median follow-up time was 3.7 years (interquartile range (IQR) 1.5–5.8 years). Among individuals with COPD and FEV1 ≥50% pred, 271 were hospitalised due to pneumonia during follow-up; of these, 51 individuals were hospitalised due to pneumonia more than once. In the COPD population with FEV1 <50% pred, 114 were hospitalised due to pneumonia during follow-up; of these, 36 individuals were hospitalised more than once.

Study population. COPD: chronic obstructive pulmonary disease; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; LLN: lower limit of normal.
Baseline characteristics according to eosinophil count ≥0.34×109 cells·L−1 versus <0.34×109 cells·L−1 in the COPD population divided according to FEV1 % pred are shown in table 1. A higher proportion of individuals with COPD and a blood eosinophil count of ≥0.34×109 cells·L−1 had elevated markers of low-grade systemic inflammation regardless of FEV1 % pred. Among individuals with COPD and FEV1 <50% pred, we found no difference in the percentage of patients treated with ICS according to blood eosinophil count, and the distribution of those treated with fluticasone versus budesonide did not differ significantly (online supplementary table S1).
Baseline characteristics of individuals with chronic obstructive pulmonary disease according to blood eosinophil count and forced expiratory volume in 1 s (FEV1) % predicted
Blood eosinophil counts and risk of pneumonia
Among individuals with COPD and FEV1 <50% pred, we found a multivariable adjusted incidence rate ratio (95% CI) of 2.17 (1.31–3.58) for pneumonia comparing individuals with blood eosinophil count of ≥0.34×109 cells·L−1 versus those <0.34×109 cells·L−1 (figure 2a). The risk remained significant, although attenuated, with a risk ratio of 1.81 (1.11–2.94) after further adjustment for the use of ICS, inflammatory biomarkers and prior pneumonia events. Compared to the nested full model without blood eosinophil counts, including eosinophils at a cut-point of 0.34×109 cells·L−1 improved the model (likelihood ratio test p=0.02). Further adjusting the model for exacerbations in the year prior to baseline gave an incidence rate ratio of 1.80 (1.13–2.86). Among individuals with COPD and FEV1 ≥50% pred, the multivariable adjusted incidence rate ratio for pneumonias was 0.80 (0.55–1.15) and further adjustment for the use of ICS, inflammatory biomarkers and prior pneumonia events did not change the results. Among individuals with COPD and with ≥10 pack-years of smoking, repeating these analyses gave similar results (figure 2b). Furthermore, in a model not taking multiple pneumonias into account, the main findings were similar (online supplementary figure S1). Risk of pneumonia using a multivariable adjusted Cox proportional hazard model excluding individuals with a hospitalisation due to pneumonia before baseline gave similar, although nonsignificant results when comparing individuals with a blood eosinophil count of ≥0.34×109 cells·L−1 to those <0.34×109 cells·L−1 (online supplementary figure S2). Including only individuals with COPD and no use of ICS prior to baseline gave similar, although nonsignificant results (online supplementary figure S3). In both forward and backward stepwise regression models, significant covariates were prior pneumonia events, number of high inflammatory biomarkers and blood eosinophil count (online supplementary table S2).
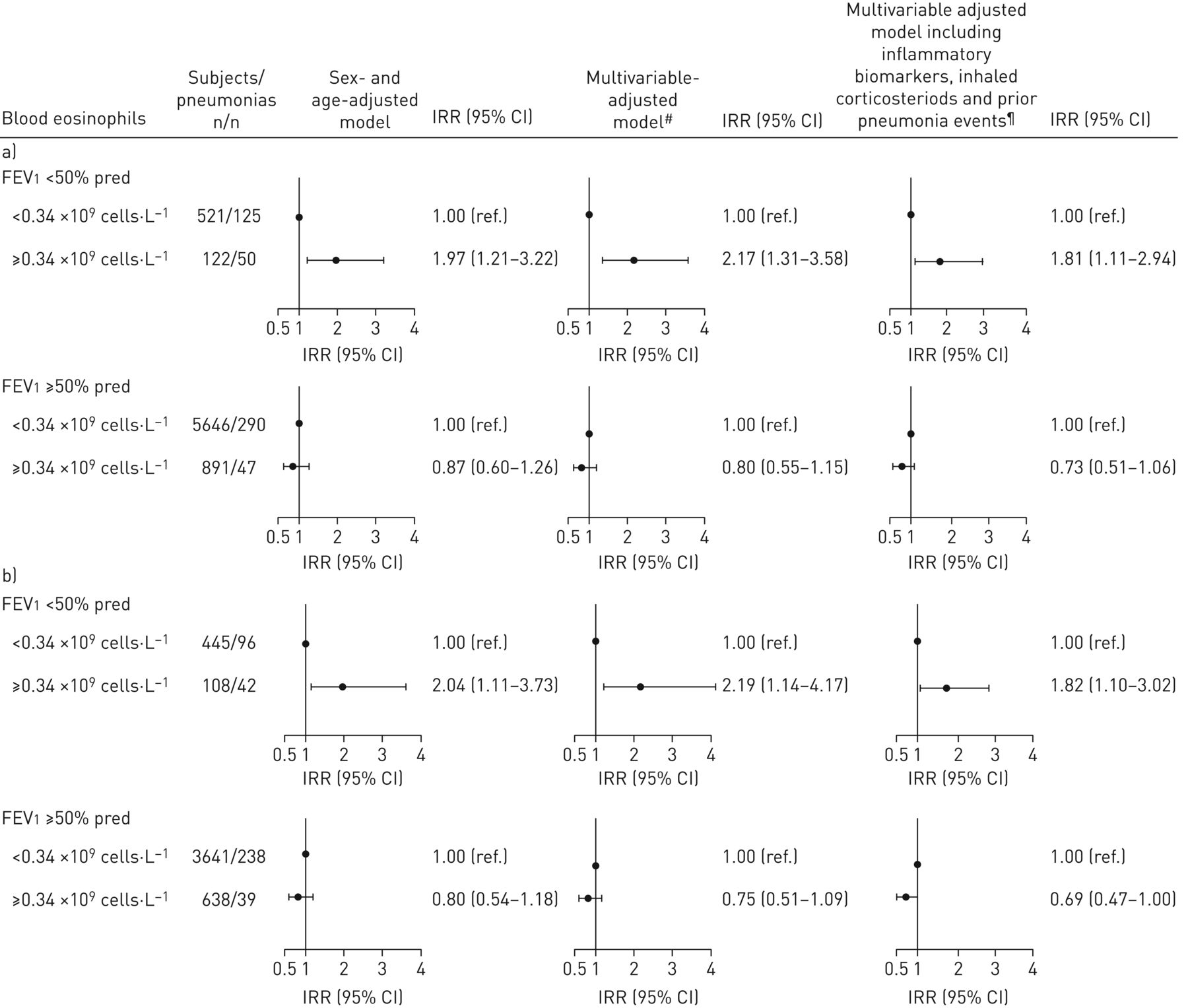
Risk of pneumonia in individuals with chronic obstructive pulmonary disease (COPD) according to blood eosinophil count. a) Individuals with COPD were grouped based on their forced expiratory volume in 1 s (FEV1) % predicted, according to the Global Initiative for Chronic Obstructive Lung Disease spirometric classification of COPD severity using FEV1 % pred (n=7180); b) analyses were repeated in a COPD population restricted to ≥10 pack-years of smoking (n=4832). IRR: incidence rate ratio. #: adjusted for sex, age, smoking status, pack-years of smoking, body mass index, education and FEV1 % pred; ¶: inflammatory biomarkers were high sensitivity C-reactive protein, leukocyte count and fibrinogen.
Using cut-points of 2% and 3.3% in blood eosinophils, individuals with FEV1 <50% pred and higher percentages of blood eosinophils had multivariable adjusted incidence rate ratios of 1.98 (1.27–3.02) and 1.50 (0.99–2.27), respectively, compared to individuals with lower percentages of blood eosinophils (online supplementary figure S4).
Among individuals with COPD and FEV1 <50% pred, the multivariable adjusted hazard ratio (95% CI) of all-cause mortality after hospitalisation due to pneumonia was 2.65 (1.08–6.52) comparing individuals with an eosinophil count of ≥0.34×109 cells·L−1 to those <0.34×109 cells·L−1 (online supplementary figure S5). Although the risk of all-cause mortality remained significant after additional adjustment for ICS, it was insignificant in the full model additionally adjusted for inflammatory biomarkers.
Blood eosinophil counts and risk of pneumonia in individuals with clinical COPD
To further examine the risk of pneumonia among individuals with COPD, we used a previously defined subpopulation with clinical COPD based on recent exacerbation, ≥10 pack-years and FEV1 <70% pred. Among these individuals, we found a multivariable adjusted incidence rate ratio (95% CI) of 4.52 (2.11–9.72) comparing individuals with a blood eosinophil count of ≥0.34×109 cells·L−1 to those <0.34×109 cells·L−1 (figure 3). Further adjustments for inflammatory biomarkers, the use of ICS and prior pneumonia events resulted in a multivariable adjusted incidence rate ratio of 3.14 (1.46–6.72).
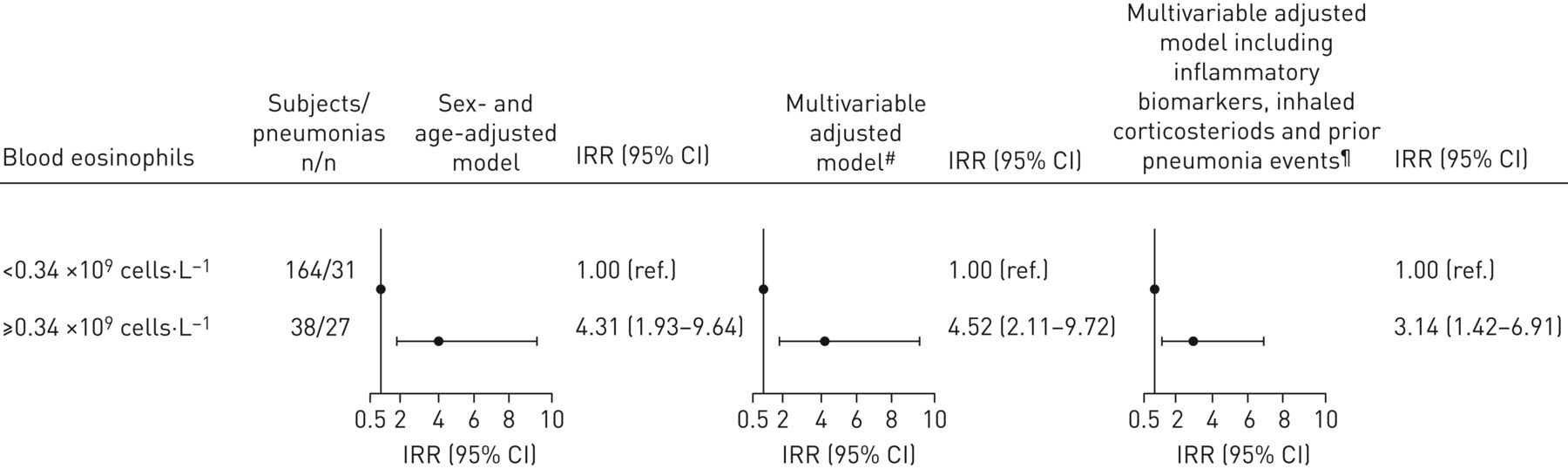
Risk of pneumonia in the clinical chronic obstructive pulmonary disease (COPD) population according to blood eosinophil count. Clinical COPD was defined as individuals with at least one exacerbation in the year prior to baseline, ≥10 pack-years of smoking and forced expiratory volume in 1 s (FEV1) <70% predicted. IRR: incidence rate ratio. #: adjusted for sex, age, smoking status, pack-years of smoking, body mass index, education and FEV1 % pred; ¶: inflammatory biomarkers were high sensitivity C-reactive protein, leukocyte count and fibrinogen.
As for the total COPD population, using cut-points of 2% and 3.3% in blood eosinophils as percentages of total leukocytes gave similar results to those reported for the absolute count (online supplementary figure S6).
Use of ICS and risk of pneumonia stratified by blood eosinophil count
As previous studies have indicated a better response of ICS in COPD patients with higher blood eosinophil counts, and because the use ICS in COPD is also associated with an elevated risk of pneumonia, we investigated whether the risk of pneumonia in users of ICS differed according to blood eosinophil count. Among all individuals with COPD and FEV1 <50% pred, the use of ICS at baseline was associated with a higher risk of pneumonia with an incidence rate ratio of 1.62 (95% CI 1.03–2.57) (figure 4). In analyses stratified by blood eosinophil count, the risk of pneumonia was elevated in users of ICS compared to nonusers in both strata, although this was not statistically significant in each stratum. There was no difference in risk of pneumonias according to the use of ICS in strata based on eosinophil count (p-value for interaction 0.78).

Risk of pneumonia according to the use of inhaled corticosteroids and blood eosinophil count. a) Risk of pneumonia comparing individuals using inhaled corticosteroids to individuals not using inhaled corticosteroids in the chronic obstructive pulmonary disease (COPD) population with forced expiratory volume in 1 s (FEV1) <50% predicted and risk of pneumonia associated with the use of inhaled corticosteroids stratified by levels of blood eosinophil count <0.34×109 cells·L−1 and ≥0.34×109 cells·L−1 (n=643); b) the same analyses for the clinical COPD population (n=202). p-value for interaction was for use of inhaled corticosteroids by blood eosinophil counts on risk of exacerbation. IRR: incidence rate ratio. #: adjusted for sex, age, smoking status, pack-years of smoking, body mass index, education and FEV1 % pred; ¶: inflammatory biomarkers were high sensitivity C-reactive protein, leukocyte count and fibrinogen.
In the subgroup with clinical COPD and less statistical power, the use of ICS was not significantly associated with a higher risk of pneumonias with an incidence rate ratio (95% CI) of 1.72 (0.81–3.67) comparing the use of ICS at baseline with no use. In stratified analyses, the risk of pneumonias was higher in individuals with a blood eosinophil count of ≥0.34×109 cells·L−1 than in those with <0.34×109 cells·L−1; however, confidence intervals overlapped and there was no significant interaction of the use of ICS by blood eosinophil counts on risk of exacerbation (p-value for interaction=0.34).
Repeated measurements of blood eosinophil counts
For 890 individuals with COPD, we had repeated measurements of blood eosinophil counts measured with a median 10 years (IQR 8.5–10.6 years) apart (figure 5). Only 41 (6.4% of the individuals included in the main analyses) of these had FEV1 <50% pred. In the COPD population with FEV1 <50% pred, 12% with eosinophil counts above the cut-point of 0.34×109 cells·L−1 had lower values at second measurements, or vice versa. The corresponding percentage in the COPD population with FEV1 ≥50% was 13%.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Repeated measurements of blood eosinophil counts 10 years apart in individuals with chronic obstructive pulmonary disease grouped according to forced expiratory volume in 1 s (FEV1) % predicted. a) FEV1 <50% pred (n=41); b) FEV1 ≥50% pred (n=849). Each individual has two measurements, with each dot representing a single measurement. Cut-off value 0.34×109 cells·L−1.
Discussion
In this study of 7180 individuals with COPD from the general population, blood eosinophil count of ≥0.34×109 cells·L−1 in individuals with COPD and FEV1 <50% pred was associated with a higher risk of future hospitalisations with pneumonia, compared with individuals with the same degree of airflow limitation but lower eosinophil count. However, the high risk was driven by few individuals in the whole COPD cohort. Only few studies have investigated the association between blood eosinophil count and risk of pneumonias, but knowledge of this relationship becomes relevant, as COPD patients with high blood eosinophil counts are candidates for ICS treatment, and as ICS as such elevate pneumonia risk in COPD. However, as we were only able to include pneumonias treated in a hospital setting, we cannot conclude on the association between blood eosinophil count and less severe pneumonias. Moreover, we cannot exclude that some severe exacerbations of COPD might have been misdiagnosed as pneumonia, which could potentially bias our results.
High blood eosinophil counts in COPD probably marks a phenotype with frequent exacerbations, although the underlying mechanism remains unknown. Eosinophilic activation during viral infections has been reported [22] and eosinophils might have an antibacterial role, although this is controversial and only reported in vitro [23]. The elevated sputum and blood eosinophil counts reported in both stable COPD [12, 24, 25] and at exacerbations of the disease [11, 13] might reflect a persistent eosinophilic inflammation with high recruitment rate of eosinophils to the airways as part of chronic airway inflammation in individuals with severe lung function impairment and increased susceptibility to pneumonias. In our study, the high risk of pneumonias appeared not to be mediated through ICS use, prior exacerbations or prior repeated events of pneumonia, but rather related to the specific eosinophilic phenotype with severe lung impairment.
In contrast to high eosinophil counts, peripheral eosinopenia can be observed in response to acute inflammation or infection [26] and has previously been identified as a strong predictor of mortality in COPD patients hospitalised with acute exacerbations complicated by pneumonia [27]. However, in the general population, elevated blood eosinophil counts when the condition is stable have been associated with a higher risk of mortality from COPD in a study with up to 30 years of follow-up [28], although retrospective data from a cohort of COPD patients with shorter follow-up time did not support this [29]. Our group has previously shown that the increased COPD exacerbation frequency associated with a higher blood eosinophil count was more pronounced when restricted to severe exacerbations requiring hospitalisation [16]. In the present study, we found an association between a blood eosinophil count of ≥0.34×109 cells·L−1 and high risk of pneumonias in individuals with COPD and severely impaired lung function, that is, a FEV1 <50% pred. Using cut-points of percentage of blood eosinophils, we found similar results. Lange et al. [30], using data from another Copenhagen cohort, have previously shown that age and FEV1 % pred are the most important risk factor for hospitalisation due to pneumonia in the general population. In the present study, we found no association between high blood eosinophil counts and pneumonia in individuals with COPD and less severe lung function impairment. We were able to demonstrate an association in a subgroup with clinical exacerbating COPD with low FEV1 and smoking history, similar to COPD patients included in clinical trials. However, our findings contrast with a recent post hoc meta-analysis of GlaxoSmithKline-funded clinical trials, including 10 861 patients with COPD from 10 clinical trials, which reported a small increase in risk of pneumonias in patients with blood eosinophil counts <2% [9]. The discrepancy may be due to different populations studied, as individuals with COPD identified from the general population, as in our study, might differ from patients included in clinical trials in terms of treatment. Another difference relates to the fact that our study had longer follow-up time than most clinical trials, which enabled us to capture more pneumonia events. The post hoc meta-analysis found no increased risk of pneumonia in COPD patients with blood eosinophil count <2% in the trials of shorter duration, with less severe COPD patients, and with low incidence of pneumonia [9]. Previous post hoc analyses of randomised trials found no difference in pneumonia incidence according to subgroups divided by a blood eosinophil count of 2% [15, 31] or the median blood eosinophil count [8]. However, the same analyses did find higher exacerbation rates with increasing levels of blood eosinophil counts and a better response to ICS among COPD patients with eosinophil counts ≥2%, although recent data from the FLAME (Effect of Indacaterol Glycopyronium vs Fluticasone Salmeterol on COPD Exacerbations) study, a randomised trial of a combination of long-acting β-agonist and long-acting muscarinic antagonist compared with a combination of long-acting β-agonist and inhaled corticosteroid did not confirm blood eosinophils as a potential biomarker of ICS response [32]. In the present study, we found that use of ICS was associated with an elevated risk of pneumonia in individuals with COPD and severely impaired lung function. Although our data show a trend towards higher risk of pneumonias among individuals with high eosinophil count, this risk did not vary significantly according to blood eosinophil count, suggesting that the use of ICS among individuals with COPD and high blood eosinophil counts might not increase the risk of pneumonias further. This was true for individuals with clinical COPD and a history of exacerbations in which treatment with ICS is relevant. Although we used a cut-point in absolute blood eosinophil count, our findings are in accordance with the FLAME study, which reported a higher incidence of pneumonia in patients on ICS, regardless of their blood eosinophil count [33].
Strengths of the present study include the large sample size and the fact that we were able to follow all individuals through the Danish registries with no loss to follow-up. However, a limitation of this study is that we could only capture severe pneumonias treated in a hospital setting, as pneumonias treated in primary care by the general practitioners are not captured by the Danish registries [34]. Therefore, we cannot conclude on the association between blood eosinophil count and less severe pneumonia. Moreover, the present study included individuals with COPD from the general population, and thus the association between blood eosinophil count at stable state and risk of pneumonia may differ in a population of COPD patients recruited in a pulmonary department. As we rely on pneumonia diagnoses drawn from the national Danish Patient Registry we cannot exclude that some severe exacerbations of COPD may be reported as pneumonias instead, as the differential diagnosis between these two events can be difficult. In addition, we are limited by the lack of information on pneumococcal or influenza vaccination. Furthermore, it can be debated whether single measurements of blood eosinophil count during stable COPD can be used as a marker of eosinophilic airway inflammation [17, 35]. Yet, a study of 141 stable COPD patients found that a peripheral blood eosinophil count of ≥0.30×109 cells·L−1 had a specificity of 76% and a sensitivity of 60% to identify sputum eosinophilia [12]. Data from the UK Clinical Practice Research Datalink have shown that blood eosinophil counts are more variable in COPD, especially for patients with higher baseline eosinophil levels [36]; however, this would tend to bias our result towards the null hypothesis. In our study we had repeated measurements of blood eosinophil counts in 890 individuals with COPD; of these, 13% had varying blood eosinophil counts around the cut-point of 0.34×109 cells·L−1. Although repeated measurements were performed with a median of 10 years apart in only 6.5% of the individuals included in our main analyses, this suggests a certain stability of the blood eosinophil count in COPD. Lastly, as we defined COPD according to the lower limit of normal and ratio of FEV1/FVC based on spirometry measurements without the use of a bronchodilator we cannot exclude that some individuals had asthma and not COPD, although we excluded individuals with self-reported asthma from our definition of COPD. In our analyses, we adjusted for inflammation using established markers of low-grade inflammation such as C-reactive protein, fibrinogen and leukocytes. Adjustments for these confounders may be problematic as they may be intermediate variables or a descending proxy for an intermediate variable, and thus adjusting for these may bias results toward the null hypothesis [37], which might be the case with mortality after pneumonia.
In conclusion, in this population study of COPD defined as a ratio of FEV1/FVC under the lower limit of normal and below 0.7 determined without the use of a bronchodilator, we found that a blood eosinophil count of ≥0.34×109 cells·L−1 in individuals with COPD and FEV1 <50% pred was associated with a higher risk of being hospitalised due to pneumonia. Among individuals with high blood eosinophil counts and FEV1 <50% pred, the use of ICS did not elevate the risk of pneumonia further. As we were not able to capture less-severe pneumonias, our study cannot conclude on the association between blood eosinophil count and pneumonias treated outside a hospital setting.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERJ-00120-2018_Supplement
Acknowledgements
The authors would like to thank staff and participants of the Copenhagen General Population Study.
Footnotes
This article has supplementary material available from erj.ersjournals.com
Conflict of interest: J. Vestbo has received personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi Pharmaceuticals, GlaxoSmithKline and Novartis, outside the submitted work.
Conflict of interest: P. Lange has received grants and personal fees from Almirall, AstraZeneca, Boehringer Ingelheim, Novartis and GlaxoSmithKline, and personal fees from Norpharma, Takeda and Pfizer, outside the submitted work.
Support statement: The study was funded by the Lundbeck Foundation, Denmark, and the Faculty of Health and Medical Sciences, University of Copenhagen, Denmark. The sponsors of the study had no role in study design, data collection, data analysis, data interpretation or writing of the paper. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received January 19, 2018.
- Accepted April 4, 2018.
- Copyright ©ERS 2018
References










