





Abstract
Experimental models are critical for the understanding of lung health and disease and are indispensable for drug development. However, the pathogenetic and clinical relevance of the models is often unclear. Further, the use of animals in biomedical research is controversial from an ethical perspective.
The objective of this task force was to issue a statement with research recommendations about lung disease models by facilitating in-depth discussions between respiratory scientists, and to provide an overview of the literature on the available models. Focus was put on their specific benefits and limitations. This will result in more efficient use of resources and greater reduction in the numbers of animals employed, thereby enhancing the ethical standards and translational capacity of experimental research.
The task force statement addresses general issues of experimental research (ethics, species, sex, age, ex vivo and in vitro models, gene editing). The statement also includes research recommendations on modelling asthma, chronic obstructive pulmonary disease, pulmonary fibrosis, lung infections, acute lung injury and pulmonary hypertension.
The task force stressed the importance of using multiple models to strengthen validity of results, the need to increase the availability of human tissues and the importance of standard operating procedures and data quality.
Abstract
This document summarises the benefits and limitations of current lung disease models and how they can be improved http://ow.ly/SLFT30jEoCf
Introduction
Animal models, organs and cell cultures are often used to assist in understanding human biology. These models are critical for the exploration of putative mechanisms in health and pathogenesis in disease, and are indispensable for the development of novel drugs. However, the pathogenetic and clinical relevance of disease models and their translational potential are often uncertain. The modelling of chronic diseases is particularly challenging. Further, the use of animals for medical research has become an important point of discussion from an ethical and political perspective [1]. Substantial efforts have been undertaken by the scientific community including the development and application of the “3Rs principles” (Refinement, Reduction, Replacement) that were introduced 60 years ago to establish the highest standards for humane experimentation on animals [2].
Numerous options for modelling specific diseases in lung research exist. Traditional and established models, as well as increasingly sophisticated newer approaches, are available, stressing the need to critically choose the best model for the research question under investigation [3]. For the foreseeable future, animal models will remain an important tool for exploring the pathogenesis of pulmonary diseases and to validate new targets, treatments and mechanisms of action of potential agents for clinical use. Appropriate and meaningful readouts and standardised end-points must be employed to obtain relevant and generalisable results. Incorrect application, or interpretation, of models has resulted in failure to translate preclinical findings to human diseases, a major challenge in all areas of medicine [4–6].
The European Respiratory Society (ERS) task force “Optimising experimental research in respiratory diseases” was established to create a comprehensive document that provides statements based on literature review and research recommendations on the best possible use of models in major areas of respiratory medicine. The task force addressed a number of general questions that are of relevance to all areas of experimental medicine. These include animal ethics, choice of species, sex and age of laboratory animals, the role of ex vivo and in vitro models, the benefits and limitations of typical outcome measurements, and the principles of gene manipulation. The task force then focused on modelling specific respiratory diseases, namely asthma, chronic obstructive pulmonary disease (COPD), pulmonary fibrosis, lung infections, acute lung injury (ALI) and pulmonary hypertension. The task force acknowledges that this report covers in vivo models more than ex vivo, which results from the original aim of the task force and the resulting literature search, the current scientific discussions on the validity of animal models, and the fact that animal models are still an important tool for exploring the pathogenesis of pulmonary diseases.
We believe that this statement focusing on animal models is likely to contribute to refinement and reduction of the use of animal models.
Methods
This ERS task force was initiated in 2014 after an ERS research seminar held in Paris (France) in October 2013. The task force was composed of a multinational, multidisciplinary group of 25 clinical and research experts. Potential participants with appropriate expertise were identified by the chairs (M. Kolb, P. Bonniaud). Broad representation of countries from Europe and North America was sought. Members were vetted for potential conflicts of interest according to the policies of the ERS. The following aims were stated prior to the inaugural meeting: 1) to issue a statement document with research recommendations about lung disease models by facilitating in depth discussions between respiratory scientists from different pulmonary subspecialties; and 2) to provide better knowledge of the available models, especially their specific benefits and limitations, that will result in more efficient use of resources, reduction in the numbers of animals in research and that will enhance the ethical standards of experimental research.
Face-to-face meetings were held during the ERS International Congresses 2014–2016. The task force members were committed to creating a document with scientific rigour and transparency of the methods used to evaluate available information. The task force statement goes beyond a typical state of the art review by providing a comprehensive and unbiased summary and evaluation of the literature.
The task force statement is organised into: 1) general issues (animal ethics, species, sex and age, ex vivo and in vitro models, outcome measurements, principles of gene editing) and 2) specific respiratory diseases (asthma, COPD, pulmonary fibrosis, lung infections, ALI and pulmonary hypertension). Lung cancer was not discussed as the panel members felt that addressing the complexity of modelling cancer needs more specific expertise and is best discussed in the context of lung cancers at large. For similar reasons, neonatal and developmental models were not discussed. Task force members were assigned to focus on one or more sections, based on clinical and scientific expertise and group leaders were appointed for each section (A. Fabre, C. Guignabert, E. White, N. Frossard, M. Inman, W. Shi, W.M. Kuebler, M. Witzenrath, M. Stampfli, S. Uhlig). Groups identified four to six key and focused questions relevant for the topic (see headers in the following sections).
Two ERS methodologists (T. Tonia, D. Rigau) had the methodological overview. The task force group leaders coordinated regular exchange by telecommunication between group members. The task force members reviewed current knowledge and new scientific advances through identifying relevant individual studies and reviews from a systematic search in MEDLINE database through PubMed (last search June 2017; however, task force members also tracked any relevant citation appeared beyond this date). The search was limited to English literature with no date limitations. This document was created by combining a systematic literature review with the research expertise of the task force members.
After a 1-day face-to-face meeting at ERS headquarters in Lausanne, Switzerland, the document was drafted. This document was critically reviewed by two senior clinician scientists with a recognised expertise in methodology in clinical research (L. Richeldi, G. Jenkins) and a junior scientist (P-S. Bellaye). All task force members unanimously agreed to its content.
The supplementary material provides detailed information on: 1) anaesthesia and euthanisation of rodents; 2) pre-analytical conditions of tissues/cell harvesting/collection/storage; 3) large animal models for respiratory diseases; 4) COPD, including clinically relevant subgroup of COPD, environmental factors and exacerbations; 5) infection/pneumonia; and 6) all the references numbered in the 14 tables.
Animal ethics
Ethical principles in animal research (“the 3Rs”)
Research aimed at improving health of humans at the expense of animals has always been a topic of ethical debate. What is not debated is that whenever such research occurs, oversight is needed to ensure that exploitation of animals is minimised. Most countries mandate an extensive set of rules and enforce them by animal ethics committees at all research centres within that country or union [2]. The basic principles are focused on: 1) Reduction, or more accurately minimisation, of the numbers of animals, 2) Replacement, wherever possible, of animal research with in vitro or in silico modelling, or ethical research with human participants and 3) Refinement of research methods in an attempt to reduce the suffering of the animal.
The ARRIVE (Animal Research: Reporting of In Vivo Experiments) guidelines are intended to improve the design, analysis and reporting of research using animals and thus maximising information published and minimising unnecessary studies [7].
Ethical oversight
A recent systematic review of mouse-based research in tuberculosis shows a promising trend where more studies report oversight by ethics boards and indicate the adoption of humane end-points [8]. There also remain studies that fail to report elements of ethical oversight, and most studies still fail to report on methods of euthanasia [8].
Misinterpretation of findings
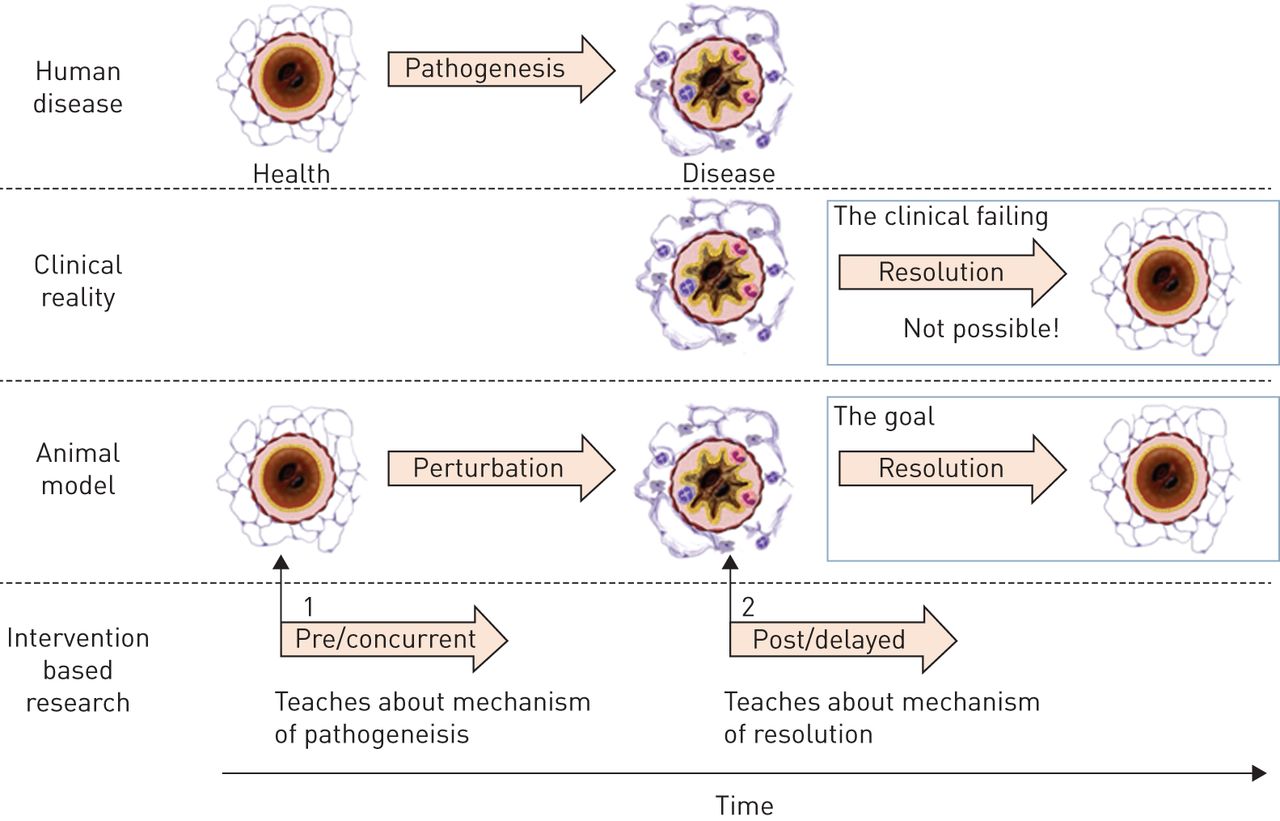
There is a growing concern with animal research regarding the extent to which it informs about human disease. Scientists argue whether a study has translational impact [9] while the public debates whether animal-based medical research is a “complete mistake” [10]. Clearly, many of those animal studies that do not directly lead to new treatments do, nonetheless, provide valuable insights for future treatments. There is an important conceptual difference between studies aiming at determining basic mechanisms of injury versus mechanisms of resolution, particularly related to a therapeutic intervention (figure 1). While there may be overlap between these in acute disease (e.g. treatment of infection with antibiotics results in resolution of inflammation), there may be no overlap whatsoever in chronic disease (e.g. blocking of a mediator that promotes deposition of fibrogenic matrix may fail to reverse established fibrotic matrix). Despite the clear distinction between injury and resolution, animal researchers often hesitate to acknowledge the limitations of their model and incorrectly present new insights in disease pathogenesis as novel therapeutic options.

Human disease involves a period of pathogenesis, resulting in a diseased state. The clinical reality of many diseases, especially chronic diseases is that treatments that reverse pathogenesis are not available. To address this failing, researchers develop models, where perturbations reproduce features of the disease, with the goal that this will aid in the development of treatments to reverse these features. A failing in the logical extension of this reasoning is that interventional research in these models is usually applied to healthy animals, or animals early in the timing of the perturbation (1), as opposed to “diseased” animals (2) which actually model the human patient.
Negative results
Publication of negative results is a major problem for scientists as there is low appetite for journals to publish them. At the current time there is little to guide editors as to whether the reasons for a negative result is due to methodological failings or whether the results represents a “true” negative outcome. However, if negative results were publishable, it would also reduce redundancy and is in line with the 3R approach [11]. One way to achieve this would be to pre-register studies and peer review these protocols, thereby confirming that the method was appropriate for the questions asked and that the negative result was correct.
Statistics
Statistical methods are essential for calculating the degree of confidence, the validity of experimental results and generalisability of the findings to other species and systems. In many papers, the lack of information detailing the statistical methods makes it difficult to judge whether or not the statistical analyses are correct and if the data had been efficiently extracted and analysed [12]. Again, this would be aided by the pre-registration of studies, which would require the inclusion of a statistical analysis plan.
Interaction with human research ethics
While the ethical principles of animal research are covered in national guidelines, care needs to be taken in cases where this research overlaps with human research ethics. An example is the use of chimeric models in which elements of human tissue (often immune cells) are introduced into a mouse host.
Recommendations for experimental research in respiratory diseases
‐ Clearly describe the rationale for the choice of the model, the identity of the ethical oversight committee, and the criteria/methods used to proceed to euthanasia.
‐ Ensure that both animal and human ethical oversight is granted and documented when required.
‐ Clearly state whether the interventional approach is aimed at uncovering mechanisms of pathogenesis or possible resolution (especially in models of chronic disease).
‐ Not claim that uncovering mechanisms of pathogenesis may lead to a new treatment unless this is warranted.
‐ Consider publication of negative results and encourage journals to accept negative results for publication.
‐ Ensure that appropriate analytical expertise is used to assess method repeatability and quality of analysis.
‐ Ensure that appropriate and stringent statistical analysis is used and provide detailed statistical methods in publications.
‐ Consider pre-registration of animal studies (as occurs with clinical trials and systematic reviews).
‐ Animal studies should be reported in accordance with the ARRIVE guidelines.
Structure, function and imaging
Imaging techniques become highly sophisticated and many of them are applicable both in humans and in animal research. Imaging bears a singular potential to advance our understanding of respiratory diseases by providing unique structural and functional information. With this in mind, the task force addressed five specific questions.
How can we utilise imaging to obtain better in-depth understanding of disease processes?
Multidimensional molecular/functional and anatomical/structural imaging provides multilevel information from the molecular to organismic scale [13, 14]. Anatomical imaging is used to measure parameters related to structure, such as lung volume and tissue density. Molecular or functional imaging using radiotracers, fluorescent probes or contrast agents can visualise biological and physiological processes such as metabolism, inflammation, permeability, ventilation, gas exchange, perfusion, infection or mucociliary clearance (table 1).
Different imaging principles and modalities applied for the study of structure and function in lung disease processes
What functions do we need to model, and how well do we do this in vivo and in vitro?
Given the abundance of functions pertinent to lung health and disease [15], the task force focused on key physiological functions at the organ, and general functions at the cellular level (table 2).
A review from the literature of key functions modelled in experimental lung research in vivo and in vitro
What does structure teach us about disease processes, and how can we assess it?
Structural analysis allows determining how structure relates to function, how injury alters structure, and to assess tissue repair in response to pharmacological interventions [16]. Structural analyses may be invasive or noninvasive, can be performed in vivo, ex vivo, in vitro or in silico. The analyses complement functional and molecular studies, and translate cellular pathways into disease- and patient-relevant pathologies [17]. Whenever possible, quantitative approaches should be implemented [17].
How does the biological context determine the outcome of in situ versus in vitro disease models?
Cellular responses to physiological and pathological stimuli depend on the microenvironment in which these stimuli act on target cells, i.e. they are highly context dependent [18, 19]. Cells within an intact anatomical and physiological environment constantly receive (and, reciprocally, send) contextual cues that will determine their phenotype, and their response to physiological or injurious stimuli. When the nature, composition, or extent of these cues changes, cells undergo phenotypic shifts. This (typically biomechanical or biochemical) effect on biological processes has to be considered when interpreting models of cellular responses (table 3).
A review from the literature of the different context-dependent dimensions that will determine cellular responses in vivo, and how they may be modelled in vitro or ex vivo
Which technical advancements are required to better interrogate models mechanistically?
Assessment of disease processes over time is the norm in the clinical scenario. In contrast, assessment of disease severity in animals is often a terminal measurement using composites of histological, biochemical, biomechanical, and physiological end-points. While these analyses provide multiscale insight into the disease from the level of single molecules to intact organisms, they provide only a brief snapshot within the continuum between health, disease and recovery. Technical advancements are required that provide better temporal resolution of biological processes, their functional effects and the underlying mechanisms. Given its unique abilities for parallel spatial and temporal image resolution, real-time visualisation could prove ideal for these requirements [20]. However, imaging of disease processes in the intact lung still has technical challenges (table 4) common to all imaging modalities. These have to be resolved to unfold the full potential for structural, functional and mechanistic analyses of imaging techniques.
Current limitations to noninvasive, temporo-spatial imaging of pulmonary structure, function and underlying mechanisms in lung disease, as well as current approaches and aspired solutions to overcome them
Task force statements
‐ State of the art imaging modalities provide unique multidimensional and multiscale insights into structural and functional features of the intact and diseased lung that are ideally suited to allow for new mechanistic discoveries and development and testing of novel therapeutics.
‐ The mechanical, biochemical, and anatomical context play an important role as critical determinants of biological/physiological responses that need to be appropriately mimicked in vitro or ex vivo depending on the respective research question.
Recommendations for experimental research in respiratory diseases
‐ Include quantitative image analysis in addition to representative images (illustration versus quantification).
In vivo versus ex vivo models
Animal models play an important role in the investigation of health and disease (figure 2). Rodents have emerged as a reliable research species due to size, life span, reproductive affluence and defined genetic background. Further, the opportunity for gene editing and the availability of sophisticated molecular and genetic tools facilitate studies in a cost-efficient way [21]. However, the challenge for disease models is their validity to reflect major hallmarks of human disorders, in the context of chronic progressive and irreversible changes. In some instances, the aetiological factors and natural history of the disease are unknown (e.g. idiopathic pulmonary fibrosis (IPF), idiopathic pulmonary arterial hypertension), while in others a molecular signature is lacking (e.g. acute respiratory distress syndrome (ARDS)); in both cases modelling becomes more difficult. Further, differences in physiology and pharmacology between animals and man have to be considered [22]. For intervention studies, the routes of drug administration also influence the interpretation of the findings.

Limitations and advantages of animal models.
The limitations of animal models (figure 2) provide the rationale for expanded use of alternative models for experimental research, particularly human ex vivo tissue and cell cultures and three-dimensional reconstructed tissues [23]. For the epithelium, an evolving area is the use of in vitro systems to visualise the cellular mechanisms that drive epithelial tissue development, to study the genetic regulation of cell behaviour in epithelial tissues and to evaluate the role of micro-environmental factors in normal development and disease. More recently, high precision cut lung slices (PCLS) have received increased interest in lung research [24]. PCLS are generated from explanted human lungs obtained during lung transplantation. They represent biomaterials from end-stage lungs from well selected patients without major comorbidities. Some of the limitations of PCLS are that the impact of circulating cellular and humoral factors and the effects of breathing and an air−liquid interface cannot be studied. On the other hand, PCLS reflect the complex cellular composition and the matrix effects of a diseased human lung, and biological diversity underlying differential treatment response in patients may well be studied in PCLS from different patients.
How is a model selected?
The American National Research Council Committee on Animal Models for Research and Aging defines an animal model as “… one in which normative biology or behaviour can be studied, or in which a spontaneous or induced pathological process can be investigated, and in which the phenomenon in one or more respects resembles the same phenomenon in humans or other species of animals” [25]. Different reasoning may lead to choosing one approach over another. Laboratory animals should ideally have an anatomy and physiology similar to humans, which is not always the case; much has been written about the differences between the lungs of humans, rodents, pigs and other mammalian species [26–28]. Experimentally induced diseases are common in the study of biology, such as bleomycin or amiodarone to mimic pulmonary fibrosis and house dust mite or ovalbumin sensitisation to mimic asthma [29, 30]. Genetically modified models include gain or loss of function (transgenic, knockout or knock-in), and allow to study the genetic basis of disease, its susceptibility, penetrance and resistance mechanisms. This is even more applicable if the gene variation or mutation causes the disease in both humans as well as rodents, such as in Hermansky−Pudlack syndrome interstitial pneumonia [31] or in infant respiratory distress syndrome on the basis of SFTPB or ABCA3 mutations [32]. There are some examples for spontaneous models in which a disorder similar to the human disease occurs naturally in animals, such as feline allergic asthma [33], pulmonary hypertension in cattle [34, 35], or pulmonary fibrosis in dogs, cats or donkeys (more examples in table 5) [36–38]. Even if models reproduce some functional features of a disease, it does not imply that they represent this disease. Similarly, models may lack specific features, but can still be valuable for understanding specific disease mechanisms.
Large animal models of non-infectious and infectious respiratory diseases
Sex/gender representation in animal models: Lately, grant agencies (e.g. National Institutes of Health) request that preclinical research is reproduced in male and female animals to account for anticipated sex differences in humans [39]. While sex differences are important in humans, treatment effects in female and male mice offer no guarantee that the findings may be applied directly to human disease.
Structural differences between rodent and human lung: Human and rodent airways differ in anatomy and cellular composition [40]. The characteristic dichotomous branching seen in human lung is not present in the mouse. While this is relevant in areas such as aerosol drug deposition, and possibly relevant for some aspects of tissue remodelling in chronic diseases, this difference becomes less important when focus is on cellular and molecular mechanisms. Also, unlike in humans, rodent intralobular airways are lined by a simple epithelium devoid of basal cells. In mouse and rat airways, nonciliated secretory cells function as pool of renewing progenitor cells, whereas in humans, basal cells play that role [26]. Differences also exist between murine strains [41]. Innate immune responses to injury differ between mice and men, for example responses of eosinophils, granulocytes and M1/M2 macrophages [42]. Finally, the impact of the microbiome on animal health and disease, clearly being affected by housing conditions, is of great importance and needs to be taken in account.
How does the model help to draw conclusions applicable to human disease?
It is clear that “mice are not men” and extrapolating results from models to human disease should be exercised with caution. Because of the unreliability of animal models to predict human responses, an honest and accurate assessment needs to be made of the actual features of disease being modelled. Models are typically designed to mimic symptoms, disease phenotypes or key aetiological factors, such as cigarette smoke or infectious agents, rather than recapitulating the disease per se [43]. Certain aspects of study design established in clinical trials (e.g. randomisation, blinding) should also be used for animal studies. Failing to do so might overcome to overestimating drug efficacy in preclinical research (table 6) [44].
Extrapolating results from models to applications in the human disease: in vivo and in vitro variables and implications
What are the best cell culture conditions for ex vivo research?
Numerous cell lines are available through commercial suppliers, however, the identity of some commercial cell lines has been called into question [45]. Using primary human cells is most valuable, but it is crucial to obtain proper patient consent. It should, however, be taken into account that primary cells may rapidly change their phenotypes in culture [46, 47]. Written standard operating procedures should be available for each protocol and laboratory equipment must be properly maintained. Novel techniques for cell subtyping may become a reliable future tool to do this. Rapid advances in RNA/DNA sequencing and cell isolation already allow single-cell transcriptomic analyses, providing not only certainty about the cell type, but insights into biological processes as well as the transcriptional “states” of individual cells [48].
What approaches can translate findings from in vivo to in vitro and vice versa?
While many investigators have “taken the leap” from animal models to human trials for lung diseases, it needs to be emphasised that this is purely a “leap of faith.” Translational approaches (i.e. models that utilise human lung tissues ex vivo and in vitro, and animal lungs ex vivo) are necessary in order to the understand mechanisms and pathways that underlie the observed phenotypic response [49, 50]. The task force members unanimously felt that to date, in vitro and ex vivo studies are complementary to animal models, but in most instances do not yet offer viable alternative approaches on their own. In silico modelling systems may have the potential to reduce animal usage in experimental research [51].
How do sampling conditions affect molecular and morphological studies?
The pre-analytic phase impacts the biological material (supplementary material contains detailed information). This includes handling and processing, the time of freezing tissues or the temperature of storing samples prior to analysis. Rigorous standard operating procedures must be followed. The effects of anaesthetic agents should be taken into account (supplementary material contains detailed information on anaesthesia and euthanasia of rodents); for instance, depression of respiration can lead to hypercapnia, hypoxia and acidosis, all of which may impact on cytokine production and regulation, among others (supplementary material).
Can large animals help the modelling of respiratory diseases?
Large animal models are thought to offer high biological relevance due to size and anatomical similarities to humans (table 5). However, the validity of this assumption has not yet been systematically analysed. Sometimes, the study of large animals may not only benefit human, but also animal, health. Although in agreement with the 3R concept and the requirements of animal welfare, models employing domestic animals are usually less well accepted. Further, large animal models are costlier, with fewer available reagents and gene manipulations, than rodents (for more information on large animal models please refer to the supplementary material).
Task force statements
‐ Mechanistic pathways observed in vitro might not be replicable in vivo but can provide important mechanistic/biological responses.
‐ The use of multiple models is required in many situations to facilitate reliable conclusions.
‐ Statistical significance does not prove biological significance.
Recommendations for experimental research in respiratory diseases
‐ Clearly and a priori define the end-points of each study.
‐ Explicitly define if the model used is exploratory or as part of a drug/device trial where power calculations are needed to obtain reliable statistical results. Experimental conditions (such as temperature/anaesthesia) should be well documented to allow for comparison between data and reproducibility of results.
‐ Researchers should be aware of novel techniques to characterise the cells they study in vitro.
Gene editing
Genetic manipulation, especially editing of endogenous or introduction of exogenous genes, are powerful tools, not only for the study of gene function in vivo, but also for generating models that resemble pathological conditions (figure 3). However, epigenetic and environmental factors can both affect the phenotype of genetically altered animals, which might explain why outcomes using the “same” mouse may vary between laboratories. Lack of experimental reproducibility due to these variable factors must be given serious consideration in research.

{kind=link}
{kind=link}
{kind=link}
Gene editing. Summary of approaches used in mouse gene manipulation and resulting genetic changes. NHEJ: nonhomologous end joining; HDR: homology-directed repair.
Does genetic background affect phenotypic presentation?
Gene editing of the same gene in mice by different groups often have dissimilar phenotypes. The background strain is an important factor, the conventional transforming growth factor-β1 knockout mouse being one example (table 7). Knockout groups must have the same genetic background, which can be achieved by backcrossing. For repetitive studies, it is best to keep the mice to the same strain background. In contrast, for initial phenotypic screening of a new genetically edited mouse line, different backgrounds may be useful to understand its entire genetic functions.
Genetic models are affected by background; phenotypic presentation of transforming growth factor-β1 knockout in mice with different strains
How does the same transgene cause variable phenotypes?
Transgenic mice are commonly generated by injection of a DNA construct directly into the pronucleus of a fertilised single cell embryo, in which the transgenic DNA is randomly integrated into the mouse genome. Promiscuous expression patterns of the transgene have been reported, possibly due to modification of the transgene promoter by the surrounding genomic components, disruption of a gene at the integration site, different copy number of the inserted transgene, or even epigenetic complication in germ cells of the transgenic parents. For example, 25 different expression patterns were reported in Thy1-XFP transgenic mice derived from 25 different founders [52]. Therefore, full characterisation of each transgenic mouse line is mandatory. When using gene knock-in or an integrase-based approach, site-specific single copy transgene can be introduced to the mouse genome [53].
How do variable phenotypes occur in the same gene conditional knockout?
Cre/loxP is the most frequently used system for creating conditional gene knockouts [54] with cell-specific and inducible deletion. Many of the Cre driver lines used in research (table 8) are transgenic mice with the caveats discussed above. Cell type specificity of a floxed-gene deletion that is induced by the same Cre driver line may vary between ages. For example, lung mesenchymal cells are differentially targeted by the Tbx4-lung enhancer depending on the induction ages [55]. In addition, inducing agents used in gene manipulating systems (e.g. tetracycline for the Tet-on or Tet-off transcription system and tamoxifen for CreER activation) may have off-target effects. It has, for instance, been reported that doxycycline affects airway epithelial cell differentiation and alveolar development in certain backgrounds [56–59]. Doxycycline also inhibits matrix metalloproteinases [60], reduces airway mucin production, and attenuates neutrophil influx into the lungs upon endotoxin challenge [61–63]. In addition, doxycycline is an antibiotic that may affect the bacterial flora and microbiome, which play important roles in experimental mouse phenotypes [64, 65]. In the case of tamoxifen, early embryonic administration can cause nonspecific phenotypes, while late administration induces early delivery of fetuses [66]. In adults, high dose tamoxifen can cause transient hypertension and cardiomyopathy [67, 68].
Some cell type-specific Cre mouse lines used in lung research
The mammalian genome also contains cryptic “pseudo-loxP” sites, which may be recombined by Cre recombinase, resulting in loxP-independent genomic alteration with nonspecific effects [69, 70]. In contrast, deletion of floxed-gene may occur in offspring including those without inherited Cre genotype (or germline leakage) [71–74], which may be due to transmission of Cre RNA or protein in the oocyte or sperm from transgenic parents.
What are the potential issues in the Crispr/Cas9 approach?
A novel approach using RNA-guided clustered regularly interspaced short palindromic repeat (CRISPR)-associated protein 9 nuclease (Cas9) has been successful in genome editing [75]. Guided RNA (gRNA) recognises specific sequences in the genome and activates Cas9 to induce a DNA double strand break. Changes in genomic DNA can be achieved by either nonhomologous end joining or homology-directed repair. Due to potential nonspecific binding of gRNA to undesired genomic DNA, off-target effects are a major issue. Although Cas9 has been modified in order to circumvent this problem [76, 77], additional experiments may be needed to validate the data, such as rescuing the phenotype by reintroducing that particular wildtype gene or generating the mutation in the same gene by targeting different sites.
Task force statement
‐ Gene editing in mice is extremely valuable for the study of gene function and generating disease-like models.
‐ Genetic, epigenetic, age and sex, and other factors (including incomplete gene knockout with “leaking”) may affect the phenotypic presentation.
Recommendations for experimental research in respiratory diseases
‐ Use appropriate controls and complementary approaches to validate the data.
Specific aspects about modelling individual pulmonary diseases
The considerations covered so far are applicable to all areas of experimental research. Individual diseases have specific features that need to be considered when developing experimental models. The task force addressed key questions focused on common respiratory disorders (asthma, COPD, pulmonary fibrosis, infections, ALI/ARDS and pulmonary hypertension). The major unmet needs for the disease area are discussed and specific subgroups are explored. We also addressed how suitable the models are for testing and validating the efficacy of new drugs.
Asthma
How do we define asthma for experimental research?
“Asthma is a heterogeneous disease, usually characterized by chronic airway inflammation, and defined by the history of respiratory symptoms (wheeze, shortness of breath, chest tightness and cough) that vary over time and in intensity, together with variable expiratory airflow limitation” [78]. Separate, but sometimes overlapping, phenotypes exist, and both environment (e.g. microbial exposure during infancy known as the “hygiene hypothesis” or air quality) and genetic predisposition are important in asthma development [79]. Asthma is classified based on age at onset, type of inflammation, presence of allergy, sensitivity to non-steroidal anti-inflammatory drugs and obesity [80]. Inhaled corticosteroids (ICS) combined with long-acting β2-adrenergic agonists (LABA) are the cornerstone in asthma treatment, but are not beneficial to all asthma endotypes (defined by distinct functional or pathophysiological mechanisms [81]). Classical murine models mimicking the common aspects of the disease, i.e. airway inflammation and remodelling, IgE production, airway hyperresponsiveness (AHR) [82, 83], are not modelling the complex reality of asthma.
What are the major unmet needs for modelling and studying asthma?
The acute allergen-driven airway inflammation models have provided important insights into early-onset eosinophilic allergic asthma and type 2-mediated immune responses [82]. This task force puts forward three unmet needs to be further explored experimentally [80, 84]. 1) Chronic asthma and remodelling: models showing chronic inflammation, airway narrowing and AHR, with bronchi exhibiting subepithelial fibrosis, smooth muscle hypertrophy and hyperplasia, altered airway epithelium, goblet cell proliferation and mucus hyperproduction. 2) Severe asthma and exacerbations: models with sustained inflammation, remodelling and AHR despite ICS-treatment, and models with a progressive aggravation of disease (e.g. upon viral challenge). 3) Non-type 2 asthma: models with neutrophilic (often Th1/Th17-driven), mixed eosinophilic/neutrophilic or paucigranulocytic bronchial inflammation; models with low sensitivity to corticosteroids and low resolution of inflammation. Strengths and limitations of these new asthma models, including age, sex, strain, hygiene in animal facility, exposures and outcome parameters (invasive pulmonary function measurements, inflammation and remodelling, severity, sensitivity to corticosteroids) need to be acknowledged [83, 85–90].
How can we model specific clinically relevant phenotypes/endotypes of asthma?
Real life conditions should be included in the models, in particular chronic exposure to allergen [83, 91, 92], cigarette smoke [93, 94], air pollution [95–97], viruses (or viral-RNA) [98, 99] or bacteria/endotoxins [100–103]. In addition, the importance of obesity, age (neonatal and aged mice) and the microbiome in asthma onset and progression should be taken into account (table 9) [104, 105]. The advantages and disadvantages of specific animal species in experimental models of asthma should be considered [106]; e.g. for investigating early and late asthmatic responses, neuronal aspects and cough, including activity of β2-bronchodilators and pharmacological studies, research in the guinea pig can provide important insights [107–109]. In vitro/ex vivo analyses and cell culturing systems [23, 110, 111] are complementary and crucial in view of the 3Rs.
Asthma: a review from the literature of the different in vivo murine models used to study specific aspects of asthma pathogenesis
How suitable are asthma models for testing and validating the efficacy of new drugs?
The new insights in asthma phenotypes and endotypes obtained have yielded to selection of the right patients for the right drug with a need of careful patient stratification in study design. Indeed, whereas for example anti-IL-5 (developed from acute allergen-driven type 2 models) initially “failed” in the first preclinical trials [112], careful patient selection has led to successful application in patients with severe eosinophilic asthma [113] with the approved anti-IL-5 mepolizumab, reslizumab and anti-IL-5Rα benralizumab. In addition, these clinical insights have highlighted the necessity for new drug development for specific patient groups. The novel animal models aim at unravelling the complexity of asthma pathophysiology, and facilitating pharmacological research focussing on difficult-to-treat asthma phenotypes.
Task force statements
‐ One asthma model cannot mimic the whole disease, but the diversity in models will provide opportunities to mimic the various aspects and the heterogeneity of asthma.
‐ Multiple preclinical asthma models are applied for targeting specific patient groups/clinical parameters.
Recommendations for experimental research in respiratory diseases
‐ Select specific models for the parameters of interest to increase the clinical relevance and applicability of asthma models.
COPD
How do we define COPD for experimental research?
According to the Global Initiative for Chronic Obstructive Lung Disease, “COPD is characterized by persistent airflow limitation that is usually progressive and associated with an enhanced inflammatory response in the airways and lung to noxious particles and/or gases. Exacerbations and comorbidities contribute to the overall severity in individual patients” [114]. Recent reports have provided longitudinal insight into the evolution of airway obstruction. These studies showed that the rate of decline in forced expiratory volume in 1 s is highly variable among COPD patients, with only a fraction showing an accelerated decline [115]. Moreover, approximately half of the COPD patients have decreased lung functions in early adulthood, with a normal decline afterwards [116], suggesting an early origin of COPD [117]. Current and former smokers with preserved lung function may still present respiratory symptoms, exacerbations and activity limitation [118]. These different phenotypes need to be taken into consideration when modelling COPD.
What are the major unmet needs for modelling and studying COPD?
Exposure of animals to cigarette smoke is one of the most relevant models for the study of smoking-associated inflammation and lung pathologies [15, 119–129]. Less well understood is how these inflammatory processes contribute to accelerated decline in lung function, how they persist following smoking cessation, and why they cause predominant airway versus parenchymal disease in subgroups of individuals. Emphasis also needs to be placed on how to repair/restore damaged parenchymal tissues. Given the early origin of COPD [117], there is a need to study the contribution of lung development, including bronchopulmonary dysplasia in the genesis of the disease. The limitation of most in vivo smoke models in mice do cause emphysema but no/little airway disease, and while major attention has been paid to tobacco smoking, COPD can also be caused by exposure to other noxious particles and gases, including biomass fuels and air pollutants [130]. A key question that emerges is whether exposure to any noxious particles and gases results in similar or differing pathogenic mechanisms and disease phenotypes. Modelling acute exacerbations of COPD in animals has proven challenging due to the clinical and pathological complexity of the underlying disease and the fact that exacerbations have a variety of causes and severities (supplementary material) [131]. There is a further need for models of COPD-associated comorbidities.
How can we model specific clinically relevant subgroups of COPD?
The pathogenesis of COPD is the result of a complex series of events perpetrated over decades [114–116]; hence, experimental models, such as exposure to cigarette smoke, and various environmental and indoor air pollutants, as well as the intratracheal administration of proteolytic enzymes, provide the opportunity to examine specific facets of the disease and study them in isolation from confounding factors. The strengths of these models are a mirror of their weaknesses. The reductionist emulation of a subset of pathogenic components fails to mimic the complexity of the disease. This is an important consideration when translating observations from experimental models to human disease. There is also a need to stratify COPD studies by sex [132]. Experimental studies have access to a broad range of reagents, tissues and intervention strategies that are not available or feasible in clinical research. This has helped to investigate mechanisms of inflammatory processes and emphysema formation [15, 119–129], and implicated protease/anti-protease balance, oxidants/anti-oxidants, apoptosis/proliferation, matrix destruction/deposition, pro-/anti-inflammatory mediators, lung development (early origin), accelerated ageing, and autoimmune mechanisms in the pathogenesis of COPD (table 10). Similarly, animal models of viral or bacterial infection, and concurrent cigarette smoke exposure have contributed to our understanding of mechanisms of COPD exacerbations [119, 123, 133–135]. Animal models have also been used to study COPD-associated comorbidities [121, 127, 136]. Thus, although experimental models have provided insight into putative pathogenic mechanisms associated with COPD, successful translation of these observations from bench to bedside will require an improved understanding of the relevance of experimental models relative to specific COPD phenotypes.
Chronic obstructive pulmonary disease (COPD): a review from the literature of the different multi-model combination systems used to study a specific aspect of COPD pathogenesis
How suitable are COPD animal models for testing and validating the efficacy of new drugs?
COPD encompasses a spectrum of obstructive lung diseases of different origins and phenotypes. No single experimental model reflects this complexity. Choosing the appropriate animal model requires an in-depth understanding of the research question, the strengths and limitations of the corresponding models, and selection of clinically relevant end-points [121]. Drugs developed using this approach will likely not be suitable for all COPD patients, but be effective in specific patient subpopulations. To date, experimental models have reflected the usefulness and limitations of a number of anti-inflammatory agents that are used clinically, including steroids and phospho-diesterase-4 inhibitors [121].
Detailed information regarding COPD is available in the supplementary material.
Task force statements
‐ No single experimental model reflects the overall complexity of COPD.
‐ Current experimental models can be used to study specific clinical phenotypes.
‐ Modelling COPD requires a better understanding of the different clinical phenotypes and selection of clinically relevant end-points.
‐ There is a lack of experimental models to investigate mechanisms of COPD unrelated to smoking effects.
Recommendations for experimental research in respiratory diseases
‐ There is no “best model” of COPD. Experimental models should be selected to address specific research question and interpreted accordingly.
Pulmonary fibrosis
How do we define pulmonary fibrosis for experimental research?
Pulmonary fibrosis refers to a diverse group of lung and pleural disorders characterised by the accumulation of extracellular matrix. Pathological fibrosis is distinct from normal wound healing and scarring because of the progressive nature and typical diffuse organ involvement leading to dysfunction. Animal models typically only resemble a few aspects of the human disease. Multiple variables (genotype, age, sex, smoking, etc.) in the human condition prohibit any single model from being the “correct model.” Absolute transparency in protocols and experimental design is therefore paramount. Despite their popularity, mice may not be the ideal animal to study fibrogenesis. It is incorrect to say that “the murine bleomycin model is a model of IPF” since the cardinal features of IPF (namely progressive fibrosis, honeycombing and fibroblastic foci) do not develop in this model [137]. The model choice should be dictated by the particular aspect of fibrosis under scrutiny, and this should be explicitly stated in research proposals and publications, with full acknowledgement of the strengths and weaknesses of the models selected. Suggested readouts for studies have been recently described [138].
What are the major unmet needs for modelling and studying pulmonary fibrosis?
Unmet needs include a better understanding of the mechanisms that govern human lung fibrosis and improved models that gradually develop progressive fibrosis. Mice, rats and hamsters have been used for decades to model pulmonary fibrosis due to the availability of reagents, low costs, the relatively short time span needed to study fibrogenesis, and the ability to manipulate the genome. However, significant differences between human and mouse lungs question the appropriateness of murine lungs as valid surrogates of human lungs [26, 27, 139]. Large animal models, using ferret, pig and sheep have been described with phenotypes that appear more congruent with human pulmonary fibrosis [140–144]. Further, naturally occurring pulmonary fibrosis models exist [37, 38, 145–152], which may offer insights into pathogenesis and systems to test therapeutic agents.
How can we model specific subgroups of pulmonary fibrosis (pleural fibrosis, hypersensitivity pneumonitis, connective tissue disease-associated pulmonary fibrosis, etc.)?
Understanding the aetiologies of various fibrotic diseases is critical. Ideally, disease modelling will result in actionable information on how to interfere clinically. It may be possible to recapitulate salient disease features when the aetiology is known (e.g. radiation pneumonitis). Still, even with the aetiology known (such as hypersensitivity pneumonitis), experimental lung disease may or may not occur after exposure. A detailed understanding of the immunological mechanisms underlying the disease (such as genetic predisposition, environmental factors or exposure duration) is necessary to create an appropriate model (table 11). Substantial resources are needed to improve “standard” models of pulmonary fibrosis and advance scientific knowledge.
Pulmonary fibrosis: a review from the literature of the different multi-model combination systems used to study a specific aspect of fibrosis pathogenesis
How suitable are these models for testing and validating the efficacy of new drugs?
For preclinical testing purposes, the task force advocates for the development of experimental systems that can be used when triggering mechanism and the secondary pathomechanistic steps are known. When both are unknown and only hypothesised, it is preferable to use models to address specific aspects of pulmonary fibrosis, including prevention of fibrosis and treatment of established fibrosis to gauge reversibility. Multiple models (in vivo, ex vivo, and high-throughput systems such as PCLS) should be considered. For instance, pirfenidone, the first approved drug for IPF [153], has been extensively tested in various preclinical models (bleomycin in hamster, mouse and rats) [154]. Similarly, nintedanib [155] had also proved its efficacy in several models (bleomycin in rats and mice, silica in mice) [154].
Task force statement
‐ Pulmonary fibrosis generally develops in phases; defining the phasic nature of individual models is necessary when planning experiments to ensure that the area of study reflects the stage of fibrosis being assessed.
‐ A single readout of a single model is insufficient to draw conclusions about the efficacy of an intervention in pulmonary fibrosis models.
‐ A particularly valuable aspect of animal models of pulmonary fibrosis is to use them to develop pharmacodynamic biomarkers. Namely markers that demonstrate target engagement that can be readily translated in clinical trials.
Recommendations for experimental research in respiratory diseases
‐ There is no “best” model of pulmonary fibrosis. Models should be chosen to answer a specific research question, not to investigate a specific disease state, and should be interpreted with the limitations of such models in mind.
‐ Multiple readouts in multiple models such as imaging, lung function, and pathophysiological data should be available before drawing strong conclusions.
Pulmonary infections
How do we define pulmonary infections for experimental research?
Pneumonia is associated with high morbidity and mortality. Novel antibiotics and therapeutic strategies beyond antibiotics are needed and disease models are instrumental in order to achieve this. Clinically, pneumonia is induced by viable pathogens that spread and replicate in the lungs, and frequently involves systemic inflammation with extrapulmonary organ pathology (table 12). Pneumonia has to be distinguished from colonisation. The causal pathogens vary, with Streptococcus pneumoniae being most prevalent in community-acquired pneumonia (CAP) [156–159], and Pseudomonas aeruginosa being among the most common pathogens in hospital-acquired pneumonia (HAP) [160]. The pathogens and their serotypes determine the lung phenotype. More than 90 Streptococcus pneumoniae serotypes have been identified [161], with major differences in virulence profiles. Therefore, the chosen serotype defines the developing disease entity. Several techniques are available for the delivery of pathogens into the lungs of animals, such as intranasal instillation [162, 163], intratracheal aspiration via oropharyngeal tube [164–172], and surgical exposure of the trachea followed by direct bacteria injection into the airway lumen [173, 174]. Factors to be considered include the stress associated with the procedure, the dose of bacteria administered, the possibility of inducing infections other than pneumonia, the impact of the injection volume and differences in the immune system of the host.
Characteristics of specific mouse models of pulmonary bacterial and viral infection (fungal infections were omitted due to space constraints)
What are the major unmet needs for modelling and studying lung infections/pneumonia?
The lungs are composed of numerous different cell types; the respiratory epithelial layer alone may contain nearly 50 different cell types [175]. For modelling of pathogen−host interaction, cells in culture need to represent their in situ counterparts in appearance, gene expression, function and signalling pathways. Moreover, interactions between recruited cells and the pathogen, and local cells, represent a major challenge [176]. Thus, at present, caution needs to be exercised when extrapolating in vitro results from simple epithelial cell culture to the in vivo situation. Intrinsic host susceptibility to infection is influenced by sex, age and comorbidities [177, 178], among others, and also by species and mouse strains [179–185]. Such variables need to be controlled in experimental pneumonia studies. Greater emphasis should be placed on clinically relevant cofactors. Finally, the microbiota is influenced by environmental factors (e.g. husbandry practices, specific pathogen free units, etc.) and has significant impact on the outcome of animal experiments [186]. Thus, all animals required for one experiment must be housed in exactly the same environment, in parallel, to reduce the influence of the microbiota on the course of pneumonia.
How can we model relevant phenotypes (e.g. local versus systemic infection) in pneumonia?
As examples, the disease entity in mice following transnasal pneumococcal inoculation is defined by the chosen serotype, which should be selected with respect to the clinically relevant phenotypes, such as pneumonia with and without bacteraemia, sepsis or ARDS [187–189]. The clinical scenario of mechanical ventilation of patients with acute respiratory failure (due to pneumonia) can also be studied experimentally in two-hit models of established pneumonia and mechanical ventilation [190].
How suitable are the models for testing the efficacy of new drugs in lung infections/pneumonia?
Testing new therapeutic approaches (antibiotics, adjunctive therapies) requires meaningful experimental protocols that match the clinical setting as closely as possible. Determining the efficiency of new treatments requires meaningful end-points. Measuring survival may be an appropriate end-point. This approach needs frequent monitoring following an approved scoring system with predefined humane end-points. Other end-points (e.g. lung permeability, inflammation, bacterial load) may be more appropriate for specific therapeutic approaches. Experimental in vivo studies have provided the rationale for approval of numerous antimicrobial therapies [191]. Others studies revealed significant disparities between in vitro and in vivo activity of antimicrobial compounds [192].
Detailed information regarding pulmonary infection is available in the supplementary material.
Task force statement
‐ Pneumonia phenotypes are diverse, largely depending on the pathogen, serotype and delivery route as well as host-specific factors.
‐ Understanding this diversity allows experimental modelling of different clinically relevant phenotypes.
Recommendations for experimental research in respiratory diseases
‐ Meaningful experimental protocols with clearly defined end-points should be used to study new treatments in pneumonia models.
Acute lung injury
How do we define ALI/ARDS for experimental research?
ARDS is a syndrome caused by different triggers such as pneumonia, acid aspiration, sepsis or polytrauma. It is diagnosed by sudden onset, bilateral infiltrates, oedema not fully explained by cardiac failure or fluid overload and hypoxaemia (PaO2/FIO2 ratio <300 mmHg) [193]. The American Thoracic Society workshop on ARDS recommended that animal models should meet at least three of the following four criteria: histologically defined tissue injury, alterations of the alveolo-capillary barrier, an inflammatory response and physiological dysfunction [194]. This definition is largely based on the assumption that the prime problem in ARDS is an acute inflammation-triggered increase in endothelial and epithelial permeability. Within this definition, models with pulmonary inflammation, but without hypoxaemia, are valid ARDS models. Models with hypoxaemia allow grading of disease severity, similar to the clinical grading, into mild, moderate or severe ARDS. Intensive care unit (ICU) treatments are life-saving for ARDS patients, but are probably also risk factors since their modification (mechanical ventilation [195], positioning [196]) improves survival. Hence, ICU treatments may contribute to the pathogenesis of ARDS and should be included in ARDS models [197–199].
What are the major unmet needs for modelling and studying ALI/ARDS?
Mortality of severe ARDS within the first week is 20% and 40% after 4 weeks [200]. Yet, most animal models last only a few hours. In many of the commonly used models (e.g. lipopolysaccharide or acid administration), animals surviving the first 72 h will recover completely [201]. The reason why 25–50% of patients will not recover is one of the central unresolved questions in ARDS [202]. Another important issue is that ARDS patients usually do not die of respiratory failure alone, but mostly succumb to multiple organ failure [203]. Therefore, ARDS models need to put more emphasis on extrapulmonary organ injury. Usual end-points in ARDS clinical trials, such as 28-day mortality, ventilator or ICU free-days are unrealistic for animal models. Unfortunately, there are no accepted surrogate end-points; even arterial oxygenation may be misleading [195]. Inflammation per se should be interpreted with caution, because inflammation develops easily and is frequently benign. End-points with absolute scales (e.g. oxygenation, compliance or wet-to-dry ratio) have benefits and allow better comparability between studies.
How can we model specific subgroups of ALI/ARDS?
Since a molecular signature is not available, a majority of ARDS models aim to replicate its aetiology and, in a minority, its pathophysiology (table 13). There are numerous reviews on assets and shortcomings of ARDS models [198, 199, 204–207]. Clinically, ARDS has been divided into pulmonary (direct) and non-pulmonary [208]. Experimentally, direct ARDS can be modelled by administering agents such as lipopolysaccharide, acid, smoke or bacteria into the airways. Non-pulmonary ARDS is more difficult to model, because systemic sepsis or peritonitis cause only relatively mild lung injury in laboratory animals. In the clinical course of sepsis, ARDS does usually not occur before several days, and it is therefore no surprise that short term sepsis models (i.p. or i.v. injection of bacteria or lipopolysaccharide) do not lead to severe lung injury.
Animal models replicate acute respiratory distress syndrome (ARDS) aetiology or pathophysiology
How suitable are these models for testing and validating the efficacy of new drugs?
Of more than 150 ARDS trials, only two interventions have proven effective by sufficiently powered trials: low tidal volume ventilation and prone positioning [209]. While these two interventions were based on animal experiments, no single model can be accredited for this success. The lack of approved pharmacological interventions, despite so many promising preclinical trials, suggests major deficiencies of current ARDS models. One key problem is certainly that most experimental studies in rodents are short-term and use prophylactic rather than therapeutic interventions. Whether fully instrumented large animal models lasting beyond 24 h have a better predictive value for subsequent clinical translation remains to be shown.
Task force statement
‐ Current preclinical models of ALI or ARDS substantially deviate from the time course, management, and end-points of clinical ARDS.
‐ While lung inflammation is usually present, it is not identical to ALI or ARDS.
‐ There is at present no ideal model that recapitulates all features of ARDS; however, individual models reflect specific aspects of the disease.
Recommendations for experimental research in respiratory diseases
‐ The use of end-points on absolute scales is encouraged to facilitate assessment of disease severity and comparisons between studies.
Pulmonary hypertension
How do we define pulmonary hypertension for experimental research?
The pathogenesis of pulmonary hypertension involves a complex and multifactorial process [210–213]. The extensive remodelling of the pulmonary vasculature develops sequentially and includes medial hypertrophy, intimal proliferation, in situ thrombosis, occlusion of small vessels, loss of distal vessels and the formation of plexiform lesions. Model systems that mimic part of the pathophysiological process of pulmonary hypertension are valuable for validating new targets or treatments and give insights into disease mechanisms (table 14). However, they do not recapitulate the full spectrum of the human condition. An ideal model of pulmonary hypertension would have a similar genetic basis, anatomy and physiology, involve the same underlying mechanisms, present similar phenotypes as do patients, and should help to predict the clinical efficacy of drugs. It is crucial to define the research problem as precisely as possible and to identify the strengths and weaknesses of each current available pulmonary hypertension model in the research context. Inherent limitations of the current available animal models are critically evaluated elsewhere [214–216].
Pulmonary arterial hypertension (PAH): a review from the literature of the different multi-model combination systems used to study a specific aspect of pulmonary hypertension (PH) pathogenesis
What are the major unmet needs for modelling and studying pulmonary hypertension?
Animal pulmonary hypertension models should include a minimum of standard parameters to inform about important aspects of this complex disorder. Cardiac catheterisation is the gold standard to measure the following haemodynamic parameters in vivo: mean pulmonary artery pressure (or right ventricular (RV) systolic pressure for mice), systemic blood pressure and cardiac output. In addition to these parameters, RV hypertrophy should be assessed by the Fulton index and lung histology should be performed to evaluate wall thickness and the percentage of muscularised pulmonary arteries. Other secondary parameters (heart rate, RV pressure rise (dP/dt maximum) and fall (dP/dt minimum), right atrial pressure, RV end-diastolic pressure) and noninvasive techniques (echocardiography, cardiac computed tomography, magnetic resonance imaging, lung function and exercise tests) can be useful to add.
Since each model system is different and mimics only some parts of pulmonary hypertension, the association of several models combined with evidence obtained from human blood, DNA, bronchoalveolar lavage, urine, and lung tissue is usually the most meaningful approach (table 14) [217]. In addition, the use of primary cultures of human pulmonary vascular cells, studied at early passages, is another valuable tool. A significant contribution to the identification of emerging molecular targets in PH has been made through genetically modified animals [218–221]. However, none of these have realistically reproduced the human disease. By combining in situ observations, animal models and in vitro studies, our knowledge of pulmonary hypertension pathogenesis will continue to increase [217].
How can we model specific subgroups of pulmonary hypertension (group 1, 2 and 3 pulmonary arterial hypertension)?
Although different forms of pulmonary hypertension [222] reflect distinct pathophysiological mechanisms, there are common denominators, such as endothelial dysfunction, exaggerated recruitment of inflammatory cells, imbalance between apoptotic and survival pathways, and abnormal interaction between endothelium and surrounding pulmonary vascular cells in pulmonary arteries [210–213]. Therefore, efforts should continue to better understand the chronobiology of the different pulmonary hypertension subgroups [223–228]. Specifically, models of pulmonary hypertension groups 2, 4 and 5 are needed, even though some common forms of pulmonary hypertension, such as chronic thromboembolic pulmonary hypertension, pulmonary hypertension associated with left heart disease or systemic sclerosis-related pulmonary hypertension have sporadically been modelled in animals [223, 225, 229, 230]. A better understanding of the similarities and differences between pulmonary hypertension subgroups is needed to know what models exist, how they can help to identify more adapted and more powerful therapeutic tools and to propose new and more relevant in vivo, ex vivo and in vitro models.
How suitable are these models for testing and validating the efficacy of new drugs?
A key element in translational research is the development of biomarkers for disease diagnosis, progression, and for testing efficacy of innovative agents. Despite drug development success in recent years, the failure to translate positive results from preclinical pulmonary hypertension studies into clinical therapies remains a major problem [217]. Both curative and preventive protocols are useful to validate clinical relevance of potential targets and to understand their mechanisms of action [231]. In confirmatory investigations, more stringent study designs are recommended and the addition of complementary models is essential.
Task force statement
‐ Animal models used in pulmonary hypertension research are very valuable for validating new molecular targets and/or treatments and giving insights into pathogenic mechanisms.
‐ No ideal model recapitulates all features of pulmonary hypertension; however, it is clear that by combining in situ observations together with findings in animals and in vitro, our knowledge of the pathobiology of pulmonary hypertension will continue to accelerate.
Recommendations for experimental research in respiratory diseases
‐ There is a need for robust assessments of the degree of pulmonary hypertension severity in animal models to confirm establishment of experimental pulmonary hypertension before studying it and/or modulating it.
‐ The survival rate, the time schedule and the reasons for the animal model choice have to be indicated and justified.
‐ A better understanding of the similarities and differences between pulmonary hypertension groups 1, 2, 4 and 5 is needed.
Conclusion
This task force statement summarises key elements of the current state in modelling lung disease using animals, tissues and cell cultures. The effort of many generations of scientists and the sacrifice of countless laboratory animals has increased our knowledge of lung health and disease enormously. One must, however, not deny the presence of failures in experimental research, notably the optimistic nature of researchers as they strive to translate biology from animal models to humans, which may lead to a number of possible biases that may misinform the outcomes. The task force emphasises the need for scientists and physicians to have an accurate and complete knowledge of the available models. The task force highlights the importance of standard operating procedures, data quality and research repositories in order to ensure that the experimental conditions are always rigorously described, ensuring their repeatability for other groups. It is of particular relevance to acknowledge the specific benefits and limitations of experimental models and, in most instances, avoid claiming to have “The Best Model of Disease X”. This will result in the more efficient use of resources, reduction in the numbers of animals, and will permit enhancement of the ethical standards of experimental pulmonary research. It is crucial to utilise the complementarity between in vivo, ex vivo and in vitro models to translate experimental findings to human disease. The scientific community has to acknowledge that major breakthroughs in experimental research do not guarantee successful translation to humans.
An important future task is to facilitate and increase the availability of human tissues. Sharing data from patient cohorts (clinical data, samples, “omics”, etc.) in order to compare and translate results from models to human tissue, as well as between research groups, is instrumental if we want to do better. This process requires the support of patients to contribute to this challenging research field.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERJ-02133-2017_Supplement
Reference list for the tables ERJ-02133-2017_Supplementary_bibliography
Acknowledgements
We thank Thomy Tonia and David Rigau, ERS methodologists, for their help with the methodological overview, Valérie Vaccaro for organising the task force meetings, and François Daubeuf (Laboratoire d'Innovation Thérapeutique, Université de Strasbourg, France) for his help with the section on asthma. We thank also OrphaLung and the Filière de santé des maladies respiratoires rares RespiFIL, CRISALIS F-CRIN French network for severe asthma, ANR-11-BSV-011–01 meso-IPF, ANR-16-CE14-0004-01 SHOT-IPF and Investissement d'Avenir ANR-11-LABX-0021-01-LipSTIC LabEx, LABEX ANR-10-LABX-0034_Medalis.
Footnotes
This article has supplementary material available from erj.ersjournals.com
This document was endorsed by the by the ERS Science Council and Executive Committee in April 2018.
Conflict of interest: P. Bonniaud reports personal fees (board/advice) from Roche, Boehringer, Novartis, TEVA and AstraZeneca, and travel reimbursement (ERS meetings) from Chiesi, outside the submitted work.
Conflict of interest: A. Fabre reports grants from Pfizer, reagents from Roche, and personal fees from MSD (Merck Sharp & Dohme Corp.), outside the submitted work.
Conflict of interest: T. Maes reports grants from Belgian Science Policy (Federal Government Belgium-Interuniversity attraction Poles), Ghent University (Concerted Research Action and Spearhead Immunology) and Novartis, and personal fees (GSK Clinical Science award: prize for best abstract presentation at Belgian Pulmonology Society Meeting 2015) and non-financial support (travel/accommodation/meeting expenses) from GlaxoSmithKline, outside the submitted work; and is shareholder of Oryzon Genomics.
Conflict of interest: W. Shi reports grants from National Institute of Health and Department of Defense, outside the submitted work.
Conflict of interest: M. Stampfli reports grants from RespiVert and MedImmune, and personal fees from AstraZeneca and Boehringer Ingelheim, outside the submitted work.
Conflict of interest: S. Uhlig reports grants from Germany Research Foundation (DFG), during the conduct of the study.
Conflict of interest: E. White reports grants and other support from NIH, personal fees for consulting from Akcea Therapeutics and Kadmon Pharmaceuticals, and research grants and personal fees for consulting from Boehringer-Ingelheim, outside the submitted work.
Conflict of interest: M. Witzenrath reports grants and personal fees from Bayer Health Care, Boehringer Ingelheim, Biotest and Vaxxilon, and personal fees from Actelion, Berlin Chemie, AstraZeneca, GlaxoSmithKline and Novartis, outside the submitted work.
Conflict of interest: B. Crestani has receieved an honorarium for speaking from Aventis, honoraria for speaking, grants for research and congress travel support grants from Boehringer Ingelheim and Roche, grants for research from CARDIF and LVL, an honorarium for speaking and congress travel support from AstraZeneca, and a grant for research and congress travel support from MedImmune, outside the submitted work.
Conflict of interest: O. Eickelberg reports grants from the Helmholtz Association, the German Center of Lung Research, Roche, and Bayer and consultancy/lecture fees from BMS, Novartis, Bayer, Intermune, McKinsey, and MorphoSys.
Conflict of interest: A. Guenther reports research funding, and compensation for lectures and consulting from Roche, compensation for lectures and consulting from Boehringer Ingelheim and Teva, and research funding from Sanofi, outside the submitted work.
Conflict of interest: G. Jenkins reports grants from GlaxoSmithKline (institutional funding for the PROFILE study) and the Medical Research Council (co-funder of the PROFILE study with GSK through MICA award), during the conduct of the study; grants from Biogen (SRA for work on integrins in IPF), personal fees (consulting and data monitoring committees on lung fibrosis) from Boehringer Ingelheim, grants (PhD studentship) from Galecto, personal fees (advisory board on IPF) from GlaxoSmithKline and Intermune, grants and personal fees (consulting on IPF, PhD studentship) from MedImmune, personal fees (consulting on IPF) from PharmAkea, personal fees (advisory board on IPF and lecture fees) from Roche, consulting on IPF (with no payment received to date) for Pliant Therapeutics, participating in scientific advisory boards (with no payment received to date) for NuMedii, and personal fees from Pulmatrix, outside the submitted work; and is a trustee for the charities Action for Pulmonary Fibrosis and the British Thoracic Society.
Conflict of interest: G. Joos reports grants, personal fees and non-financial support from AstraZeneca, grants and personal fees from Boehringer Ingelheim, Chiesi, GlaxoSmithKline and Novartis, and personal fees from Mundipharma, Sandoz and Teva, outside the submitted work.
Conflict of interest: U.A. Maus reports grants from Federal Ministry of Education and Research, German Research Foundation and Lower Saxony Society for the Control of Tuberculosis and Bronchial Diseases, outside the submitted work.
Conflict of interest: L. Richeldi reports grants and personal fees (for advisory board membership) from InterMune, personal fees (for advisory board membership) from Medimmune, Roche and FibroGen, personal fees (for consulting activity) from Biogen, Sanofi-Aventis, ImmuneWorks, Celgene and Nitto, personal fees (for speaking) from Shionogi, and personal fees (for membership of steering committee) from Boehringer Ingelheim, outside the submitted work.
Conflict of interest: M. Kolb reports grants and personal fees from Roche, Boehringer Ingelheim, GSK, Gilead, Prometic and Alkermes, grants from Actelion, Respivert and Synairgen, and personal fees from AstraZeneca and Genoa, outside the submitted work.
This article has supplementary material available from erj.ersjournals.com
- Received October 16, 2017.
- Accepted April 2, 2018.
- Copyright ©ERS 2018
References











Jump To
- Article
- Abstract
- Abstract
- Introduction
- Methods
- Animal ethics
- Structure, function and imaging
- In vivo versus ex vivo models
- Gene editing
- Specific aspects about modelling individual pulmonary diseases
- Asthma
- COPD
- Pulmonary fibrosis
- Pulmonary infections
- Acute lung injury
- Pulmonary hypertension
- Conclusion
- Supplementary material
- Acknowledgements
- Footnotes
- References
- Figures & Data
- Info & Metrics