





Abstract
There is limited high-quality evidence available to inform the use of text messaging to improve latent tuberculosis infection (LTBI) treatment adherence.
We performed a parallel, randomised controlled trial at two sites to assess the effect of a two-way short message service on LTBI adherence. We enrolled adults initiating LTBI therapy from June 2012 to September 2015 in British Columbia, Canada. Participants were randomised in a 1:1 ratio to standard LTBI treatment (control) or standard LTBI treatment plus two-way weekly text messaging (intervention). The primary outcome was treatment completion, defined as taking ≥80% prescribed doses within 12 months (isoniazid) or 6 months (rifampin) of enrolment. The trial was unblinded except for the data analyst.
A total of 358 participants were assigned to the intervention (n=170) and control (n=188) arms. In intention-to-treat analysis, the proportion of participants completing LTBI therapy in the intervention and control arms was 79.4% and 81.9%, respectively (RR 0.97, 95% CI 0.88–1.07; p=0.550). Results were similar for pre-specified secondary end-points, including time-to-completion of LTBI therapy, completion of >90% of prescribed LTBI doses and health-related quality of life.
Weekly two-way text messaging did not improve LTBI completion rates compared to standard LTBI care; however, completion rates were high in both treatment arms.
Abstract
Weekly two-way text messaging did not improve latent tuberculosis treatment completion in a high-resource setting http://ow.ly/9gLA30hzSlE
Introduction
Successful treatment of latent tuberculosis infection (LTBI) is key to eliminating tuberculosis (TB) in low-incidence countries, and an essential tool for facilitating global TB elimination [1–3]. Unfortunately, LTBI therapy has historically low rates of treatment uptake and completion, and such deficiencies in the “LTBI care cascade” greatly limit the population impact of LTBI therapy [4, 5]. To optimise the impact of LTBI therapy, new strategies are needed.
Over the past decade, there has been growing interest in the use of mobile phones to improve outcomes in active TB care [6–8]. Recently, the European Respiratory Society and World Health Organization published a digital health strategy and performed a 2017 technical consultation, noting the potential for mobile phone-based interventions to improve TB surveillance, care, learning and connectivity [9, 10]. In addition, at least three systematic reviews have examined the role of mobile phones in improving active TB care, and a number of randomised control trials are underway [6, 7, 11]. To date, however, there is limited high-quality data to support the use of mobile phones in LTBI treatment.
One of the most common forms of mobile phone communication, short message service (SMS) messaging, is ubiquitous and potentially well-suited for improving communication between patients and healthcare providers. Enhanced communication through SMS messaging could potentially lead to improved health literacy, quality of care, and treatment outcomes for a number of medical conditions, including active TB and LTBI [12]. The SMS-based communication is relatively low-cost and commonly used in both high- and low-income regions. In recent years, several studies have been performed to evaluate the influence of SMS on treatment adherence in chronic disease [13, 14]. Evidence has been mixed depending on the condition, setting and type of SMS messaging [13]; however, two-way SMS communication, meaning a messaging format that includes both content sent by a healthcare provider and a reply from the patient, has been associated with improved medication adherence in multiple study settings [15].
In this study, we aimed to assess whether two-way SMS communication between healthcare providers and adults initiating LTBI therapy improved LTBI treatment completion, health-related quality of life (HRQoL) and satisfaction with LTBI care in a high-income setting.
Material and methods
Trial design
We conducted a parallel-group, randomised controlled trial comparing standard LTBI treatment (control arm) with weekly two-way SMS in addition to standard LTBI treatment (intervention arm). Details are provided in the published trial protocol [16].
Participants
Between June 2012 and September 2015, we recruited participants from two publicly funded, specialised TB clinics in Vancouver and New Westminster, British Columbia, Canada. Both clinics provide free screening, diagnostic treatment and support services for patients being evaluated for, or diagnosed with active TB or LTBI in the Greater Vancouver Area. Both clinic populations consist of primarily migrant and marginalised populations. LTBI was diagnosed by BC Centre for Disease Control (BCCDC) physicians based on demographic, clinical and radiological factors, in combination with a tuberculosis skin test and/or interferon-gamma release assay results.
Inclusion criteria were as follows: participants were diagnosed with LTBI by a BCCDC physician and ≥19 years of age; owned or shared access to a mobile phone; were able to use simple text messaging in English or have someone (e.g. a friend, partner or relative) respond on their behalf; were able and willing to provide informed consent to participate. Participants were excluded if they previously started LTBI therapy, were diagnosed with active TB, or were enrolled in another study that could have influenced LTBI treatment adherence.
Initially, only patients starting 9 months of daily isoniazid (9INH) therapy were eligible for recruitment, but due to a change in clinical practice during the trial period, from October 2014 onwards, patients starting 4 months of daily rifampin (4RIF) were also eligible.
Eligible participants provided written consent at enrolment. The study protocol was approved by the University of British Columbia Ethics Board (H11-02216) and is registered with ClinicalTrials.gov (NCT01549457).
Randomisation and masking
Simple randomisation was performed at a 1:1 allocation ratio, based on a computer-generated randomisation list. Written allocation of assignments was sealed in individual, sequentially numbered, non-resealable, opaque envelopes distributed to both clinics. After meeting the inclusion criteria, consenting to participate and completing a baseline questionnaire, participants were randomly assigned to a study arm.
Standard care
Participants in the control and intervention arms received standard LTBI care, which was initiated with a 30-day supply of medication (9INH or 4RIF daily) and baseline bloodwork. Participants were then seen on a monthly basis for the first 3 months, and depending on adherence and tolerance, subsequent visits were extended to every 2 months for 9INH (see supplementary material for details on treatment monitoring). Clinic visits consisted of a symptom screen and medication review by a nurse and pharmacist. Participants who experienced adverse events were referred to the TB clinic physician for evaluation and further management. Between clinic visits, participants with urgent medical issues (e.g. new adverse event) were able to contact the clinic during normal business hours; however, all medication interruptions or changes required a clinic visit. All treatment changes were recorded. At the final scheduled clinic visit, participants met with the TB clinic physician to review treatment, which could have been extended if poor adherence or tolerance was noted. The study treatment protocol continued until treatment was deemed “complete” or “discontinued”. All participants were followed for 12 months or until treatment completion.
Intervention
The SMS intervention involved a weekly text message to “check-in” with participants and provide them with an opportunity to identify any concerns. Each Monday at noon, an automated SMS message from a central clinic computer was sent to the intervention arm participants’ mobile phones asking “Are you OK?” Participants were instructed to respond within 48 h, whether they were well (e.g. yes) or had an issue to discuss (e.g. no). A clinic nurse reviewed incoming texts and called participants who identified issues. Participants who did not respond within 48 h received a second text message stating “Haven't heard from you. How's it going?” A clinic nurse called participants who did not respond within 48 h of the second SMS message. Participants received automated texts every Monday until treatment completion, discontinuation of LTBI therapy or study withdrawal. Participants were informed that the SMS service did not replace existing clinical services and that urgent matters should be handled by usual means.
Outcomes
The primary outcome was treatment completion, defined as the proportion of participants who completed ≥80% of prescribed 9INH doses within 12 months, or ≥80% of prescribed 4RIF doses within 6 months. Treatment adherence was measured by participant self-reporting, and confirmed with a pill count at each clinic visit. Secondary outcomes included the percentage of missed doses; treatment completion at a 90% threshold (i.e. ≥90% doses within the same time intervals); time to treatment completion; and HRQoL using the Short Form 12 (SF-12) questionnaire. In addition, participant satisfaction with the SMS intervention was measured using Likert-type questions at the end of the study period. Demographic and clinical information were recorded in the clinic's electronic medical records at baseline (time 0), and updates on clinical status were recorded in the clinic's electronic medical records after clinic visits or telephone interactions. All SMS communications were recorded by WelTel software.
Statistical analysis
A detailed description of the analytical methods used can be found in the published trial protocol [16]. We calculated that approximately 175 people per study arm would be required to detect a 12% improvement in adherence, with 80% power and α=0.05. This calculation assumed that 72% of the individuals in the control arm and 84% of the individuals in the intervention arm would meet the definition of treatment completion. The estimated improvement in adherence was based on a trial that examined the effect of two-way SMS messaging on HIV treatment adherence [14]. No interim analysis was planned.
We reported primary and secondary outcomes based on an intention-to-treat analysis. The primary outcome and binary secondary outcomes were compared using the Chi-squared test. We also analysed outcomes per intervention received and per protocol.
Missing items on the SF-12 questionnaire were imputed using multiple iterations (m=5) of chained equations, after confirming that responses were missing at random, based on pattern analysis (data not shown). If a participant had six or more missing items, their SF-12 scores were excluded from the analysis, as the quality of imputation can be reduced, past this threshold.
Data monitoring
This trial did not have a data and monitoring committee, as it was deemed minimal risk.
Role of the funding source
The trial sponsors had no role in the design of the study protocol, data collection, analysis, interpretation, writing of the report or decision to submit the manuscript for publication.
Results
From June 2012 to September 2015, we enrolled and randomised 358 participants; 170 to the SMS intervention arm and 188 to the control arm (table 1). Follow-up continued until September 2016. Of those randomised, 22 participants crossed over; 17 participants randomised to the intervention arm erroneously received control treatment and five participants randomised to the control arm received the intervention. In addition, 18 participants were lost to follow-up; nine in the intervention arm and nine in the control arm (figure 1). Demographic and clinical characteristics of both groups are presented in table 1.
Baseline characteristics of study participants
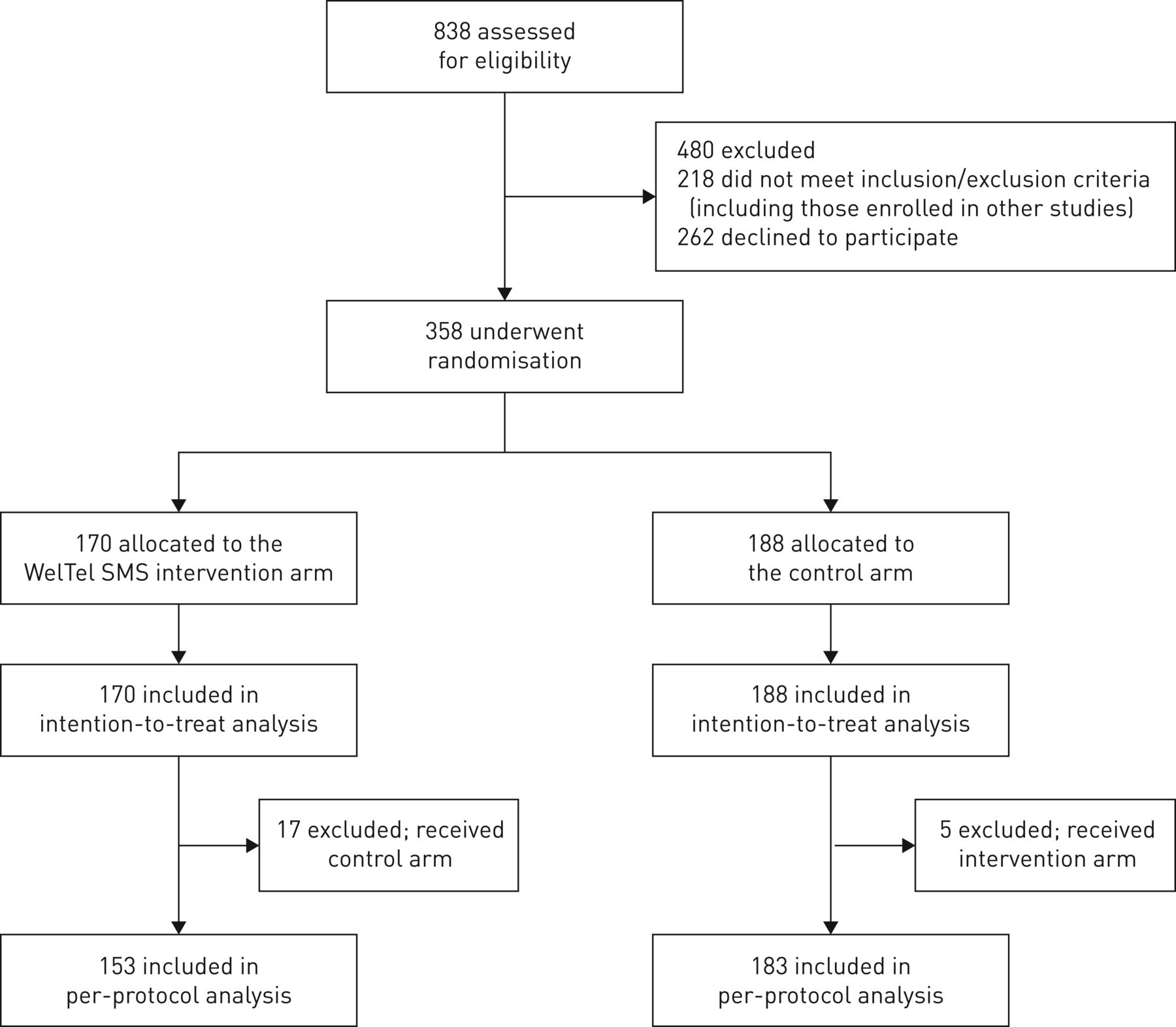
Screening, randomisation and analysis.
The median age of the study population was 43 years (interquartile range (IQR) 33–52); 119 out of 358 (33.2%) participants were ≥50 years of age (table 1). The majority of participants were born outside of Canada (294 out of 355, 82.8%), with most born in South Asia or Southeast Asia (202 out of 355, 56.9%). A total of 82 out of 350 (23.4%) participants self-reported English as their first language, although 273 out of 348 (78.5%) participants were most comfortable communicating in English, and 325 out of 344 (94.5%) preferred to send and receive SMS messages in English.
Over the course of the study period, the median response to the automated weekly SMS message was 93.7% (IQR 90.6–96.0), with a median of 91.2% (IQR 88.3–93.8) responding “okay” and 2.0% (IQR 0–3.7) responding “not okay” (supplementary material).
Primary outcome
No significant difference was observed between the proportions of participants meeting the primary end-point in the intervention (135 out of 170, 79.4%) or control (154 out of 188, 81.9%) arms (RR 0.97, 95% CI 0.88–1.07; p=0.550). Results were similar in the per protocol analysis and when analysed by intervention received (table 2). Participants that met the primary end-point had similar characteristics to participants that did not meet the primary end-point (supplementary material).
Primary and pre-specified secondary outcomes
Pre-specified secondary outcome: adherence measures
No significant differences were noted in the pre-specified secondary outcomes for adherence. Participants missed a median of 0 (IQR 0–3) doses in the intervention arm, and 0 (IQR 0–3) in the control arm (p=0.971); 77.1% and 80.9% completed 90% of the doses in the intervention (n=131) and control (n=152) arms, respectively (RR 0.95, 95% CI 0.86–1.06; p=0.381) (table 3; figure 2).
Reason for treatment end and adverse events

{kind=link}
{kind=link}
Time to treatment completion for isoniazid (INH) and rifampin (RIF).
Pre-specified secondary outcome: HRQoL and satisfaction with care
Overall, we received 138 (81.2%) completed end-of-study questionnaires from participants in the intervention arm, and 128 (73.9%) in the control arm, with the remaining questionnaires in each arm not completed, missing or status unknown (table 3). Secondary outcomes measuring HRQoL showed no association with the intervention. At end of treatment, the median SF-12 physical composite score was 54.9 (IQR 47.6–57.0) in the intervention arm and 54.1 (IQR 46.3–57.1) in the control arm (p=0.823). The median SF-12 mental composite score was 53.7 (IQR 48.7–58.6) in the intervention arm and 53.5 (IQR 47.9–57.7) in the control arm (p=0.471).
Clinic visits, adverse events
By the time of treatment completion, 43 out of 131 (32.8%) and 28 out of 136 (20.6%) participants in the intervention and control arms, respectively, reported one or more adverse events related to LTBI treatment. Among these participants, 27 out of 43 (62.8%) in the intervention arm and 25 out of 28 (89.3%) in the control arm visited a healthcare facility for treatment. Details are provided in table 3.
Communication with healthcare providers
Using a Likert-type scale, ranging from 1 to 5 (with 1 corresponding to not at all; 5 to very much so), participants reported similar ability to contact their healthcare practitioners (mean±sd 4.5±0.9 (intervention) and 4.4±0.9 (control arm); p=0.999), and similar levels of communication with their healthcare practitioners (mean±sd 4.5±0.8 (intervention) and 4.6±0.8 (control); p=0.542). A trend was observed towards participants in the intervention arm contacting healthcare providers more frequently in relation to medication side effects, and contacting the clinic less frequently regarding appointment confirmation/rescheduling (table 3).
Comparison with the provincial treatment programme
Over the course of the study period, 262 people starting LTBI therapy declined to participate in the trial. Of those that declined participation, 77 out of 262 (29.0%) stated that they were too busy to participate in the study, whereas 47 out of 262 (17.9%) did not routinely text or had difficulty with texting; 139 out of 262 people (53.0%) were not interested or declined study participation for unknown reasons. We were unable to ascertain the demographic data and LTBI treatment outcomes of people that refused to participate in the trial. However, we did compare participant treatment outcomes with the provincial LTBI treatment statistics [17]. From 2012–2014, the median age of a person starting LTBI therapy in British Columbia was 45.0 years, and LTBI treatment completion (similarly defined) in British Columbia was 76.3%, increasing from 72.4% in 2012 to 78.6% in 2014.
Discussion
Our study showed that weekly two-way SMS did not improve LTBI treatment completion rates compared to standard LTBI care. High treatment completion rates were achieved in both treatment arms, with nearly 80% of participants completing ≥80% of prescribed LTBI doses within 6 months (4RIF) or 12 months (9INH). When we analysed the data per protocol and per intervention received, no significant differences were noted between treatment arms.
Pre-specified secondary outcomes were also comparable, including the proportion of participants with >90% treatment completion, time to treatment completion and HRQoL. One potential difference in outcomes between treatment arms was in the proportion of participants with adverse events and healthcare facility visits. A greater number of participants in the intervention arm experienced adverse effects related to LTBI treatment, whereas a higher proportion of control arm participants experiencing adverse events visited health facilities during treatment. This suggests that weekly two-way SMS messaging might enhance adverse event reporting; however, this difference was identified in post hoc analysis, and ultimately, a similar proportion of participants in each arm visited healthcare facilities for adverse events. Further study will be required to understand the significance of this finding.
A second potential difference between study arms was the proportion of participants completing end-of-study questionnaires. In per intervention received analysis, 85.9% of intervention participants and 69.7% of control arm participants completed end-of-study questionnaires. This could have biased reporting results, and may reflect improved healthcare engagement at the end of therapy. Whether this engagement is clinically relevant is unclear, as there were no significant differences in treatment outcomes, participant satisfaction or quality of life between the two arms.
To our knowledge, this is the first randomised trial to report the effect of mobile phone technology on improving LTBI treatment adherence. The importance of LTBI therapy has been increasingly recognised in global TB elimination [1, 2, 3]. At this point, however, deficiencies in the LTBI care cascade remain a significant barrier to the population-based impact of LTBI therapy, even in well-resourced TB care and prevention programmes. Indeed, a recent systematic review by Alsdurf et al. [4] noted that only 19% of individuals with an indication for LTBI therapy complete an adequate course of therapy. With new efforts to increase LTBI uptake in high TB burden regions, low-cost, high-impact strategies to improve LTBI uptake and completion are needed.
There appears to be considerable interest in mobile health technologies for improving TB and LTBI care [9]. With mobile phone penetration exceeding 90% globally, SMS messaging is an appealing, relatively low-cost intervention that could be brought to scale for LTBI therapy, using pre-existing frameworks for HIV and other chronic diseases [18]. Reflecting this, we are aware of at least two randomised control trials, and additional qualitative work evaluating the role of SMS in LTBI adherence [19–21]. The rapidly expanding literature evaluating SMS messaging and treatment adherence likely reflects a health system response to patient populations that is increasingly relying on SMS messaging for mobile communication. Other more intensive forms of adherence support, such as electronic pillboxes and video directly observed therapy have been used in active TB treatment and may also play a role in supporting LTBI adherence [22, 23]. The exact roles of different types of mobile technology in LTBI adherence support remains uncertain, and thus far, the evidence does not clearly support the use of SMS alone to improve LTBI treatment adherence.
This study has several potential limitations. First, we reported unexpectedly high proportions of LTBI treatment completion, which might have affected the primary outcome. There are several potential explanations for such high proportions of treatment completion. The intensive monitoring schedule in our standard care included monthly clinic appointments; this may be difficult to improve upon with mobile technology support. In addition, during the study period new LTBI diagnostic protocols emerged, and could have improved adherence [17]. Indeed, we noted a significant increase in LTBI treatment completion in British Columbia from 2012 through 2015, with 77.7% of LTBI clients completing therapy under routine conditions in 2015 [24].
A second explanation for the high proportions of LTBI treatment completion could be related to measurement of the primary outcome. Self-reported adherence was used to measure the primary outcome and might have overestimated true adherence; however, self-reported adherence has been shown to be a robust measure of adherence in other infectious diseases [25]. In addition, only 80% of the doses were required within a given time-frame to be considered “treatment complete”. When examining a more strict definition of treatment completion (>90% treatment completion) and time to treatment completion, however, we noted no significant difference in treatment outcomes (figure 2). Lastly, the Hawthorne effect might have played a small role in treatment outcomes in both study arms.
Another limitation in this study is the exclusive use of an English language SMS messaging. Less than a quarter (23.4%) of participants identified English as their first language, raising concerns that English language messaging might have been insufficient for some participants. Interestingly, however, the majority (78.5%) of participants identified English as their preferred language of communication and 94.5% of the participants preferred sending SMS texts in the English language (table 4).
Self-reported language preferences and comfort with English language texting
We also noted a relatively low participation rate in this study, which could potentially influence the generalisability of our results. A large number of people were excluded from this study because of competing studies addressing LTBI adherence. Other reasons for non-participation are less clear; over half of the potential participants declined to participate without providing a reason for non-participation. Nonetheless, only 17.9% of the participants cited limited ability to send and receive SMS messages, and focus group work performed by our team in 2011 noted that the majority of LTBI clinic patients were receptive to weekly SMS messaging [26].
Lastly, we noted significant unintentional crossover in this study, with 22 participants erroneously receiving the wrong treatment post allocation. After analysing the results in per-protocol and per-intervention analysis, no significant differences were noted between treatment arms, and as a result, we do not believe that this crossover was a major source of bias in our results.
Conclusion
In this study, a two-way SMS messaging service did not increase adherence in participants initiating LTBI therapy. Other parameters, such as the HRQoL and perceived healthcare communication also showed no improvement. However, there was a trend towards improved adverse event reporting, a finding that requires exploration. Further research is required to understand the exact role of this common form of communication in the management of LTBI therapy.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERJ-01488-2017_Supplement
Disclosures
Supplementary Material
R.T. Lester ERJ-01488-2017_Lester
Footnotes
This article has supplementary material available from erj.ersjournals.com
Support statement: This study was supported by the Canadian Institutes of Health Research (Institute of Health Services and Policy Research) and the Michael Smith Foundation for Health Research. Funding information for this article has been deposited with the Crossref Funder Registry.
Conflict of interest: Disclosures can be found alongside this article at erj.ersjournals.com
The study is registered with ClinicalTrials.gov (NCT01549457).
- Received July 21, 2017.
- Accepted November 17, 2017.
- Copyright ©ERS 2018
References










