





Abstract
Preventing the occurrence of acute exacerbations of chronic obstructive pulmonary disease (AECOPD) is a major therapeutic goal. We hypothesise that persistently increased levels of exhaled nitric oxide (FeNO) during follow-up can identify a group of COPD patients at higher risk of AECOPD.
To test this hypothesis, we measured FeNO levels (HypAir FeNO®, Medisoft; Sorinnes, Belgium) prospectively in 226 clinically stable COPD outpatients at recruitment and during follow-up (at 6 and 12 months). Patients were stratified according to the number of visits with FeNO ≥20 ppb.
FeNO was <20 ppb in all three visits in 44.2% of patients, 29.6% in visit 1 and 26.1% in visit 2 or 3. These three groups suffered progressively higher AECOPD rates during follow-up (0.67, 0.91 and 1.42, respectively, p<0.001). After adjusting for potential confounding variables (log-rank test), the hazard ratio for AECOPD was higher in the latter group (1.579 (95% CI 1.049–2.378), p=0.029). Likewise, time to first moderate and severe AECOPD was shorter in these patients. Finally, there was no relationship between FeNO levels and circulating eosinophils.
Persistent FeNO levels ≥20 ppb in clinically stable COPD outpatients are associated with a significantly higher risk of AECOPD.
Abstract
Persistently elevated FeNO levels in COPD are associated with a higher risk of exacerbation http://ow.ly/fdPy30hdBzo
Introduction
Chronic obstructive pulmonary disease (COPD) is a major health-problem worldwide [1, 2]. Acute exacerbations of COPD (AECOPD) represent important events in the course of the disease because they accelerate the decline of lung function [3] and worsen the prognosis [4] and health status [5] of these patients. Hence, prevention of AECOPD is a major therapeutic goal in COPD [6].
So far, the best predictor of future AECOPD events is past history of AECOPD [7]. More recently, post-hoc analysis of large studies suggest that high circulating eosinophil counts are also associated with increased AECOPD frequency [8], which, importantly, can be prevented and treated with inhaled corticosteroids (ICS) [9, 10] These observations could reflect a predominant T-helper 2 cell (Th2) inflammatory response in the airways of these patients since peripheral blood eosinophils relate to airway eosinophilia [11], which, in turn, is a marker of ICS response in COPD [12].
The exhaled nitric oxide fraction (FeNO) is a well recognised and widespread used biomarker of Th2 airway inflammation in asthma [13, 14] The role of FeNO in COPD is less well established, but it appears to relate to airway eosinophilia [15, 16], bronchial responsiveness [17] and response to ICS treatment [18]. In fact, FeNO has been proposed as a potential biomarker of ACO (Asthma–COPD overlap) [19]. In a previous cross-sectional study we showed that using a cut-off point of 20 parts per billion (ppb), FeNO could effectively distinguish different COPD phenotypes [20]. Yet, the longitudinal reproducibility of FeNO in COPD and its potential relationship with COPD outcomes (AECOPD in particular) has not been explored and remain unclear. We hypothesised that there is a subgroup of COPD patients with FeNO levels persistently >20 ppb that are at an increased risk of AECOPD. We tested this hypothesis in a prospective, longitudinal, observational study.
Methods
Study design and ethics
This prospective 1-year follow-up, observational study recruited patients who attended our outpatient tertiary clinic. Patients visited three times, at recruitment and at 6- and 12-months follow-up. Patients who experienced an AECOPD during follow-up were asked to delay their clinical visit for at least 4 weeks, until completion of treatment with oral corticosteroids and/or antibiotics.
The main outcomes were as follows. 1) Distribution of patients stratified by the reproducibility of FeNO measurements during follow-up. As in our previous publication [20], patients were stratified into three groups according to the number of visits with FeNO ≥20 ppb (0, 1 or ≥2 visits). 2) Annualised exacerbation rate and time to first moderate AECOPD (i.e. treatment with oral corticosteroids and/or antibiotics) and/or severe (hospitalisation or emergency room visit for >24 h) [6].
The study was conducted in accordance with the Declaration of Helsinki of 1975, and was approved by the Ethics Committee of Clinical Research at our Institution (PEIBA). All participants gave informed consent.
Study population
We included adults (≥40 years of age) who were current or former smokers with a cumulative smoking exposure ≥10 pack-years, and who had COPD according to international diagnostic criteria [6] capable of performing lung function tests serially. Exclusion criteria were as follows: occurrence of AECOPD during the previous 4 weeks, presence of chronic respiratory diseases other than COPD, such as asthma, tuberculosis or α1-antitrypsin deficiency, or current participation in another research study.
Measurements
At recruitment, data on cumulative smoking exposure, previous medical history, concomitant diseases [21], usual treatment and number and severity of AECOPD in the previous year were collected from medical records in each participant. Circulating eosinophils counts were recorded if they had been obtained under conditions of clinical stability during the previous 3 months. The Spanish version of the COPD Assessment Test (CAT) questionnaire was self-administered [22]. The clinical investigator and patients were blinded to FeNO results. Spirometry (before and after the administration of 400 g of salbutamol) was measured following international recommendations [23]. FeNO was measured at a constant flow (50 mL·s−1) with a chemiluminescence nitric oxide analyser (HypAir FeNO®; Medisoft, Belgium), also following international recommendations [24, 25].
At each follow-up visit (6 and 12 months), patients completed the CAT questionnaire, moderate and severe AECOPD were registered and spirometry and FeNO measurements were determined.
Statistical analysis
Results are presented as sample size, range, median (interquartile range) or mean±sd. Categorical variables were compared using the Chi-squared test, whereas continuous variables were compared using ANOVA, the t-test or Mann–Whitney U-test, as required. To account for multiple comparisons, statistical significance was defined as p<0.01. We used Cox regression analysis to compare time to first AECOPD in each group, after adjusting for age, sex, smoking status, previous AECOPD history and ICS use. Analyses was performed using SPSS version 20.0 (IBM corporation, Armonk, NY, USA).
Results
Characterisation of patients
Figure 1 presents the consort diagram of the study. We screened 314 patients, of whom 244 were included in the study. 18 were lost to follow-up; therefore, data from 226 patients was analysed. Table 1 shows their baseline characteristics. Participants were predominantly males of ∼70 years of age, with significant smoking exposure (46 pack-years); approximately 25% of participants were current smokers. Most patients had moderate airflow limitation and the most frequent Global Initiative for Obstructive Lung Disease (GOLD) 2017 groups were B and D. Most patients were treated with long-acting bronchodilators and about half were treated with ICS. The mean exacerbation rate in the previous year was 1.7 events. In 230 (95.5%) patients, circulating eosinophil counts during clinical stability were available; 65% showed eosinophil counts >2%.

Consort diagram of the study.
Baseline characteristics of 244 study participants
Reproducibility of FeNO during follow-up
Figure 2 presents the reproducibility of FeNO measurements during follow-up. At baseline, 32% of patients had FeNO levels ≥20 ppb, 46% had levels of 10–20 ppb and 21% had levels <10 ppb. During follow-up, the reproducibility of these measurements were 9% for FeNO ≥20 ppb, 24% for levels of 10–20 ppb and 2% for levels <10 ppb; thus, FeNO measurements were reproducible in 35% of the patients. The intra-class correlation coefficient (ICC) between FeNO measurements during the study was low (ICC 0.387, 95% CI 0.234–0.513). Supplementary figure S1 shows Bland–Altman plots comparing measurements between visits.
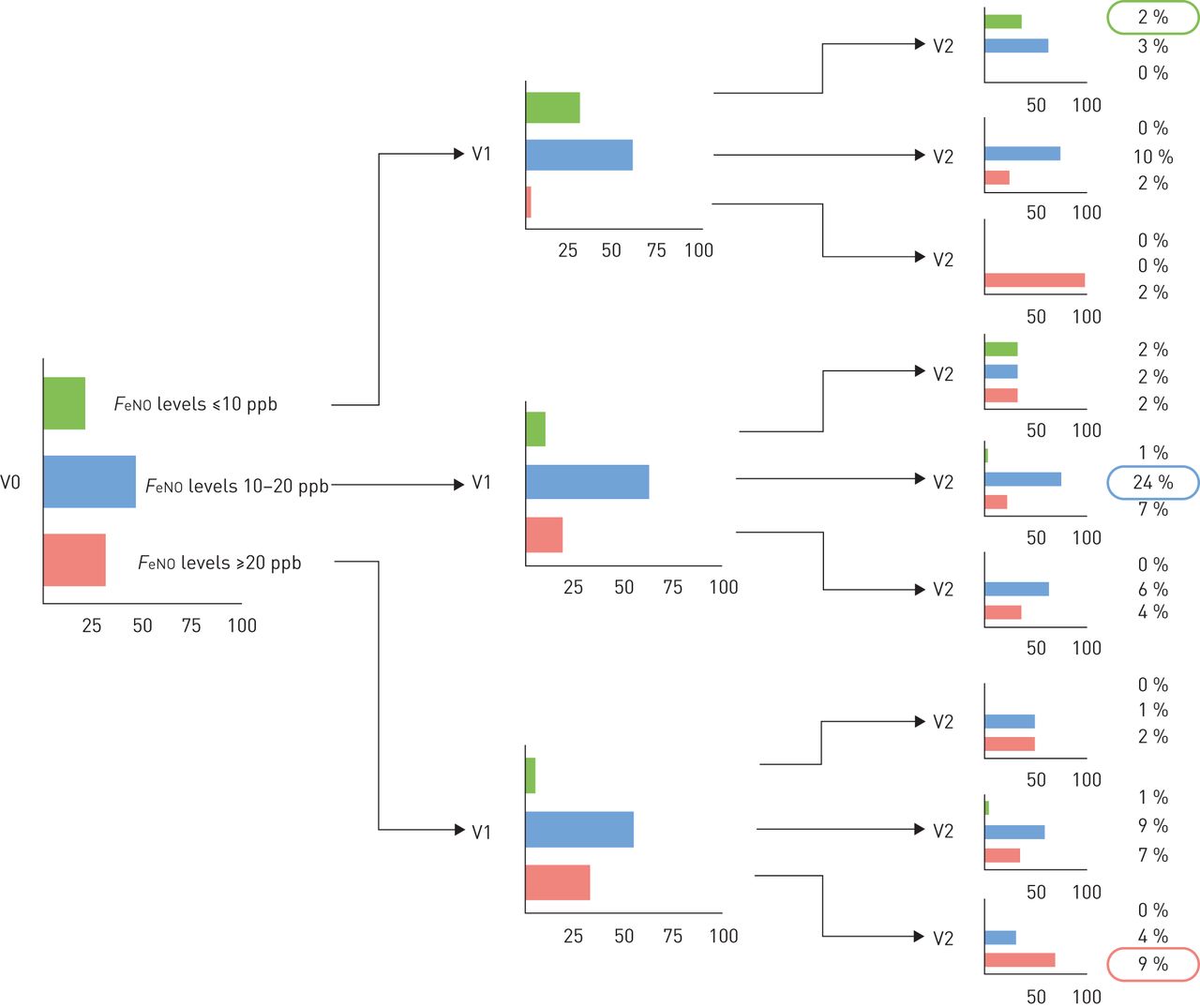
Reproducibility of exhaled nitric oxide fraction (FeNO) measurement during 12-months follow-up. V0: recruitment; V1: 6 months; V2: 12 months.
Table 2 compares the clinical characteristics of patients with FeNO levels ≥20 ppb at no visit (n=100) and 1 (n=67) or ≥2 visits (n=59) during follow-up. At baseline, FeNO was higher (p<0.001) in patients with a larger number of visits with FeNO ≥20 ppb during follow-up. Generally, no differences were observed between groups in most demographic and clinical characteristics, with the exception of the group with repeatedly normal FeNO levels with a higher female prevalence and less severe airflow limitation. Of note, there were no significant differences in ICS usage, rate of previous exacerbations or circulating eosinophil levels between the three groups (table 2).
Characteristics of patients according to the number of visits with exhaled nitric oxide fraction (FeNO) levels ≥ 20 ppb during 12-months follow-up
AECOPD rates during follow-up and relationship with FeNO
Table 3 compares AECOPD rates and time to first AECOPD by AECOPD severity (moderate, severe and moderate and severe), according to the number of follow-up visits (0, 1 or ≥2) with FeNO levels ≥20 ppb. Patients with FeNO ≥20 ppb during ≥2 visits had a significantly higher rate of moderate, severe and moderate and severe AECOPD (figure 3). The trends towards a higher proportion of patients with ≥1 AECOPD (46.0% for zero visits versus 57.1% for one visit versus 61.6% for ≥2 visits; p=0.057) and a higher proportion of frequent exacerbations during follow-up (17.0% versus 25.7% versus 38.5%; p=0.015) were observed. The increased risk was mostly driven by severe exacerbations in patients with FeNO ≥20 ppb during ≥2 visits (table 3) after adjusting for confounding variables. Likewise, patients with FeNO ≥20 ppb during ≥2 study visits showed a shorter time to first AECOPD than the other groups (table 3 and figure 4).
Comparison of acute exacerbation of chronic obstructive pulmonary disease (AECOPD) rate, time to first AECOPD and AECOPD severity levels according to number of follow-up visits with exhaled nitric oxide fraction (FeNO) levels ≥20 ppb

Annualised rate of acute exacerbations of chronic obstructive pulmonary disease among participants in the study, stratified by the number of visits during which exhaled nitric oxide fraction (FeNO) levels were ≥20 ppb. *: p<0.05; **: p<0.001.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier analysis of time to a) moderate and severe, b) moderate and c) severe acute exacerbations of chronic obstructive pulmonary disease (AECOPD) adjusted for age, sex, smoking, inhaled corticosteroids and previous exacerbation history, and stratified by the number of follow-up visits with exhaled nitric oxide fraction (FeNO) levels ≥ 20 ppb.
Discussion
This study shows that COPD patients with persistently (≥2 follow-up visits) elevated FeNO values (≥20 ppb) have a higher risk of AECOPD, irrespective of previous ICS use, smoking history or previous AECOPD, particularly for severe exacerbations requiring hospitalisation. Thus, monitoring FeNO in the clinic can provide useful information to determine the risk of AECOPD in these patients.
Previous studies
The clinical characteristics of the patients included in this study, as well as the FeNO levels determined here, are similar to those reported in previous studies of FeNO in COPD [18, 26]. Likewise, our observation that approximately one-third of the patients showed reproducible FeNO levels during follow-up is also in line with previous reports of smaller populations (n=70) [27].
Interpretation of findings
AECOPD, particularly those requiring hospitalisation (i.e. severe AECOPD), are important events during the course of the disease, because they are associated with increased lung function decline, higher mortality and worse health status [3–5]. Prevention of AECOPD episodes is, therefore, a major therapeutic goal in COPD [6]. So far, the best predictor of future AECOPD is the history of previous AECOPD episodes [28]. We hypothesised that persistent FeNO levels >20 ppb are associated with an increased risk for AECOPD because they are a well-established biomarker of Th2 inflammation in asthma, and it is known that patients with asthma-COPD overlap have frequent AECOPD [29, 30]. The results have confirmed this hypothesis because patients with FeNO ≥20 ppb during ≥2 study visits had a significantly higher risk of AECOPD, even after adjusting for other established risk factors, such as current smoking and previous history of AECOPD. Participants with persistently elevated FeNO levels showed a higher female prevalence and less severe airflow limitation is consistent with previous reports in patients with ACO [31]. Essentially, therefore, our results suggest that persistently increased levels of FeNO might be a favourable biomarker of ACO in clinical practice, although the optimal timing of these measurements has not been evaluated in this study.
However, despite recent observations indicating a relationship between circulating eosinophil counts and AECOPD [32], we found no significant differences in circulating eosinophil counts among groups. Given that the distribution of circulating eosinophils in our study population was similar to that reported in larger populations [8], there is a reasonable possibility that eosinophil count and FeNO could not predict exacerbations in a similar manner.
Strengths and limitations
Important strengths of our study include the large sample size and lengthy follow-up. However, some weaknesses deserve comment. First, it is a single-centre study, therefore, results need to be confirmed in other settings. Secondly, we collected data on pharmacological COPD treatments, but we did not record changes in these treatments during follow-up; thus, we cannot analyse the influence of this potential confounder. Finally, the design of the study provided exacerbations during visits and there was no follow-up period after visit 2 so we could not assess the risk of exacerbations occurring after visit 2.
Conclusions
This study shows that COPD patients with recurring FeNO levels ≥20 ppb during follow-up are at an increased risk of AECOPD exacerbations.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary figures ERJ-01457-2017_supplementary_figures
Disclosures
Supplementary Material
A. Agusti ERJ-01457-2017_Agusti
B. Alcazar-Navarrete ERJ-01457-2017_Alcazar-Navarrete
P.J. Romero-Palacios ERJ-01457-2017_Romero-Palacios
Acknowledgements
The authors thank the participants of the study for their willingness to contribute to medical research.
Footnotes
This article has supplementary material available from erj.ersjournals.com
Support statement: This study was supported by Fundacion Neumosur (grant number 01/2011). Funding information for this article has been deposited in the Crossref Funder Registry.
Conflict of interest: Disclosures can be found alongside this article at erj.ersjournals.com
- Received July 19, 2017.
- Accepted October 5, 2017.
- Copyright ©ERS 2018
References










