





Abstract
Eosinophilic inflammation in chronic obstructive pulmonary disease (COPD) predicts response to treatment, especially corticosteroids. We studied the nature of eosinophilic inflammation in COPD prospectively to examine the stability of this phenotype and its dynamics across exacerbations, and its associations with clinical phenotype, exacerbations and infection.
127 patients aged 40–85 years with moderate to very severe COPD underwent repeated blood and sputum sampling at stable visits and within 72 h of exacerbation for 1 year.
Blood eosinophils ≥2% was prevalent at baseline, and predicted both predominantly raised stable-state eosinophils across the year (area under the curve 0.841, 95% CI 0.755–0.928) and increased risk of eosinophilic inflammation at exacerbation (OR 9.16; p<0.001). Eosinophils ≥2% at exacerbation and eosinophil predominance at stable visits were associated with a lower risk of bacterial presence at exacerbation (OR 0.49; p=0.049 and OR 0.25; p=0.065, respectively). Bacterial infection at exacerbation was highly seasonal (winter versus summer OR 4.74; p=0.011) in predominantly eosinophilic patients.
Eosinophilic inflammation is a common and stable phenotype in COPD. Blood eosinophil counts in the stable state can predict the nature of inflammation at future exacerbations, which when combined with an understanding of seasonal variation provides the basis for the development of new treatment paradigms for this important condition.
Abstract
Blood eosinophil levels in COPD predict the nature of inflammation at future exacerbations and may guide therapy http://ow.ly/W10o30dNQiq
Introduction
Chronic obstructive pulmonary disease (COPD) is an established cause of global mortality and morbidity, predicted to be the third leading cause of death by 2030 [1]. Current guidelines for COPD management are based on airway obstruction, symptoms and exacerbation frequency [2]. The guidelines advise on stepwise management, but do not fully account for the biological heterogeneity of this debilitating condition.
Eosinophilic inflammation was historically thought to be a feature of asthma, with neutrophilic inflammation being a classical hallmark of COPD. However, recent studies have demonstrated that eosinophilic inflammation is present in a subset of COPD patients both at exacerbations and during clinical stability [3, 4]. A sputum eosinophil differential count of >3% is an accepted marker of airway eosinophilic inflammation and is derived from the reported enhanced response of this group of patients to corticosteroids [5, 6]. Moreover, a good relationship has been demonstrated between airway and systemic eosinophil counts [3, 4, 7]. It was previously reported that a >2% blood eosinophil cut-off had a high sensitivity in identifying >3% airway eosinophils during acute exacerbations of COPD (AECOPD) [3], suggesting that peripheral eosinophils are a clinically accessible marker to predict inflammatory phenotype.
Using 2% blood eosinophils as a cut-off in the longitudinal ECLIPSE cohort, persistent elevation of blood eosinophils was reported as a common finding [4], especially in milder disease, but exacerbations were not sampled. Reports of relationships between eosinophils and forced expiratory volume in 1 s (FEV1) and exacerbation frequency vary [4, 8–12], but emerging evidence suggests measurement of eosinophils has clinical relevance. For example, severe AECOPD with eosinophilic inflammation are associated with a shorter length of hospital stay [13]. Furthermore, there is an association between eosinophilic inflammation with a greater response to steroid therapy in both stable COPD and during exacerbations [5, 6, 14–16].
Management of asthma stratified by airway eosinophilic inflammation has led to a reduced rate of exacerbations [17]. Siva et al. [14] demonstrated that COPD treatments targeting airway eosinophils were associated with a significant reduction of severe exacerbations.
Hence, eosinophilic inflammation is an important COPD endotype, but little is known about its stability over time or its relationships to the inflammatory nature and aetiology of exacerbations. To improve our understanding, we investigated these factors in a secondary analysis of the AERIS (Acute Exacerbation and Respiratory InfectionS in COPD) cohort, a prospective, longitudinal study of patients with COPD [18].
Methods
Study design and study population
The AERIS study is a prospective, observational cohort study based at University Hospital Southampton (Southampton, UK) and registered with ClinicalTrials.gov (identifier NCT01360398). The study protocol and full inclusion/exclusion criteria have been previously published [18]. The protocol summary is available at www.gsk-clinicalstudyregister.com (identifier 114378). AERIS was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice, and was approved by the Southampton and South West Hampshire Research Ethics Committee. All participants provided written informed consent. Only patients with a confirmed diagnosis of COPD based on post-bronchodilator spirometry with FEV1 ≤80% of predicted and FEV1/forced vital capacity (FVC) <0.7, and ex-smokers or current smokers with significant smoking history (≥10 pack-year history) were included in the cohort, with no patients having diagnosis of asthma at the time of recruitment [18].
Patients were followed monthly in the stable state and reviewed within 72 h of onset of AECOPD symptoms. Exacerbations were detected using daily electronic diary cards. Definitions of AECOPD and severity were as previously described [18, 19].
Procedures
Blood and sputum analyses were performed as previously described [18, 19]. Further methodological details are provided in the supplementary material.
Criteria for eosinophilic groups and seasonality
Eosinophilic inflammation was defined as sputum eosinophils >3% and blood eosinophils ≥2%, in line with previous studies [3, 5, 6, 14, 20]. To investigate the stability of blood eosinophilic inflammation over time we divided subjects into three groups: predominantly (PE), intermittent (IE) and rarely (RE) eosinophilic groups. Only those subjects who had at least three (out of five potential) stable visits with valid blood results over 12 months were included in the group analyses (n=99). The PE group was defined as blood eosinophils ≥2% at either all visits or all but one visit where blood eosinophils were <2%; the RE group was defined as blood eosinophils <2% at all visits or all but one visit where blood eosinophils were ≥2%; the IE group was defined when none of the above-mentioned criteria were met.
To investigate an impact of seasonality on exacerbations we divided the year into two seasons: winter (October–March) and summer (April–September).
Statistical analysis
Bivariate analyses testing for differences between eosinophilic groups were conducted using two-tailed, Kruskal–Wallis, ANOVA, Chi-squared or Fisher's exact tests, as appropriate. Receiver operator curves were used to assess the predictive ability of different cut-offs to correctly identify presence of sputum eosinophilic inflammation. Intraclass correlation coefficients (ICCs) were used to assess the reliability of measures within individuals over time. As some subjects were represented multiple times in exacerbation analysis, descriptive analyses were conducted only for the first exacerbation occurring for each subject and multivariate analyses with binary outcomes (presence/absence of different conditions at exacerbation) were conducted using conditional logistic regression, including the subject number as a random effect. SPSS version 22 (IBM, Armonk, NY, USA) was used for all analyses with the exception of ICCs and conditional logistic regression, which were analysed using Stata version 14 (StataCorp, College Station, TX, USA). All of these analyses should be considered post hoc as they were not pre-specified in the AERIS statistical analysis plan.
Results
General characteristics of the cohort
152 patients were screened, but only 127 patients were included in the AERIS cohort (figure 1). The cohort consisted of patients with moderate to very severe airway obstruction; the majority (87.3%) were receiving inhaled corticosteroids and had a substantial smoking history (mean±sd pack-years 50.3±28.2) (table 1). Only patients who experienced at least one moderate to severe exacerbation in the last 12 months were included in the cohort (median (interquartile range (IQR)) rate 2.00 (2.00)).
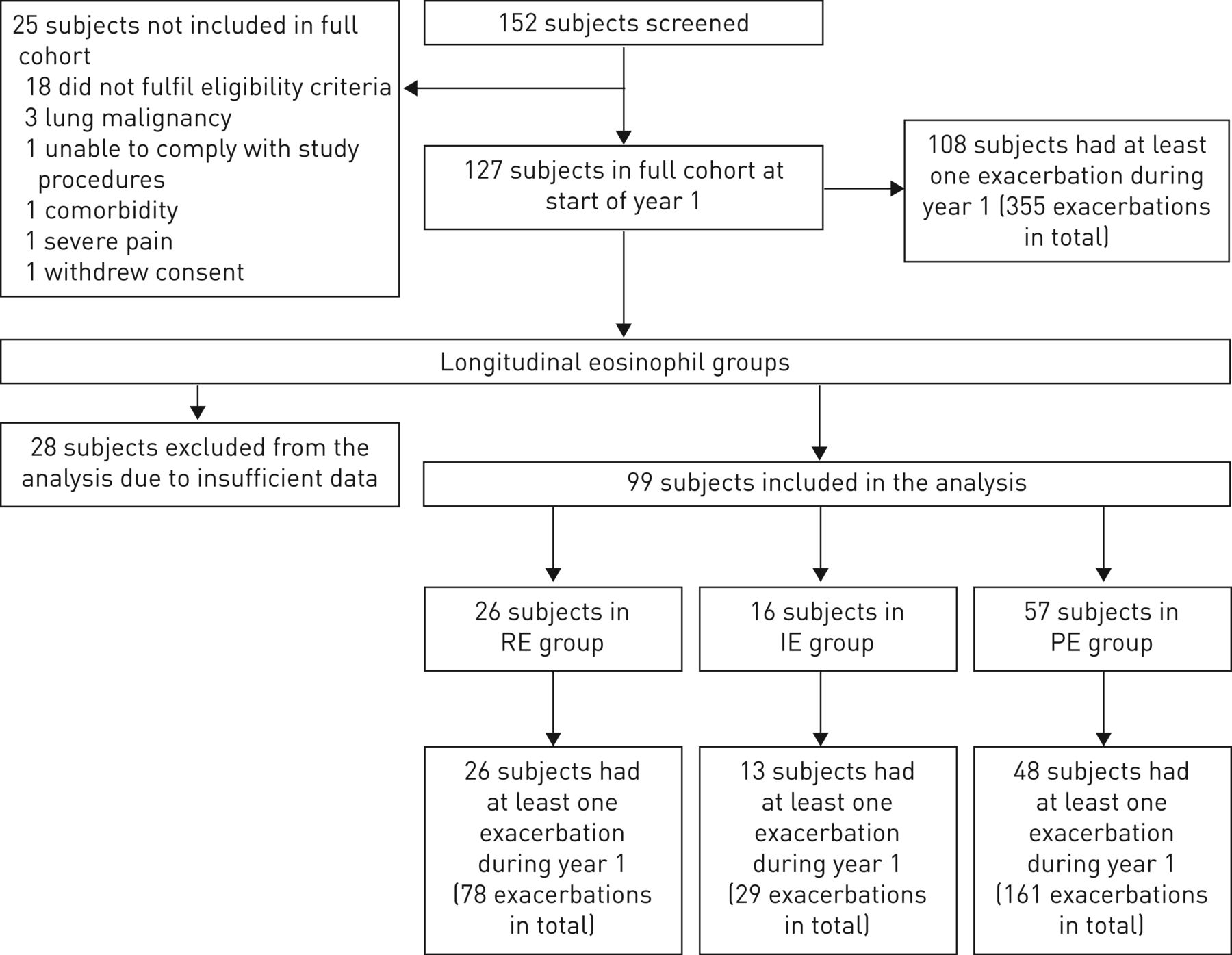
Flow diagram of the subjects screened and included in the full cohort at the start of year 1 and the number of exacerbations in year 1. RE: rarely eosinophilic; IE: intermittently eosinophilic; PE: predominantly eosinophilic.
Baseline characteristics of the total chronic obstructive pulmonary disease (COPD) cohort
Clinical and inflammatory characterisation at enrolment
The prevalence of eosinophilic inflammation ≥3% in sputum in our cohort at enrolment was 33% (n=27) and in blood ≥2% was 68% (n=86). Blood eosinophils (percentage and count) displayed moderately strong positive correlations with sputum eosinophil percentage (ρ=0.463 and 0.581, respectively, at enrolment; p<0.001) and were predictive of sputum eosinophils >3% (area under the curve (AUC) 0.851, 95% CI 0.750–0.951 and AUC 0.768, 95% CI 0.651–0.884, respectively) (figure 2). This ≥2% blood eosinophil cut-point was 95.8% sensitive and 31.8% specific. Using absolute cell numbers (≥200 cells·μL–1) rather than percentages gave similar results (table 1).

Receiver operating characteristic curve with area under the curve (AUC) for blood eosinophils (count and percentage) at enrolment predicting sputum eosinophilia >3% at enrolment (n=68). Blood eosinophil count: AUC 0.768, 95% CI 0.651–0.884; blood eosinophil percentage: AUC 0.851, 95% CI 0.750–0.951.
Stability of eosinophilic phenotype over time
We categorised our patients into three longitudinal eosinophilic inflammation phenotypic groups based on blood eosinophils ≥2% and found that, out of the 99 patients with sufficient data, 57 (58%) were in the PE group, 16 (16%) were in the IE group and 26 (26%) were in the RE group over the 12 months examined (table 2). Between the three longitudinal groups, the only significant differences observed at enrolment were age, blood neutrophils and presence of sputum eosinophils >3% (table 2). There were also significant differences in the PE group exacerbation rate over the first year. Significant differences between patients included and excluded from this analysis were seen for C-reactive protein (CRP), 6-min walk test (6MWT) and length of follow-up (supplementary table E2). In order to assess the longitudinal stability of blood eosinophilic inflammation, we analysed the reliability of the marker in defining a longitudinal phenotype and found blood eosinophils to be relatively stable within individuals across the 12 months examined, including enrolment (ICC 0.66, 95% CI 0.58–0.74).
Baseline characteristics by longitudinal blood eosinophil group over 12 months for the 99 patients with sufficient data
We next examined whether blood eosinophils at a single time-point (enrolment) were a useful predictor of being in the PE group over time (categorisation for the eosinophilic inflammation groups excluding enrolment, n=78). Blood eosinophils (percentage and count) at enrolment were predictive of being in the PE group over the next 12 months (AUC 0.841, 95% CI 0.755–0.928 and AUC 0.806, 95% CI 0.710–0.901, respectively) (figure 3). A blood eosinophil cut-off of ≥2% was 84.3% sensitive and 48.1% specific in identifying those in the PE group over the next 12 months.

Receiver operating characteristic curve with area under the curve (AUC) for blood eosinophils (count and percentage) at enrolment predicting the predominantly eosinophilic group over 12 months following enrolment (n=78). Blood eosinophil count: AUC 0.806, 95% CI 0.710–0.901; blood eosinophil percentage: AUC 0.841, 95% CI 0.755–0.928.
Blood eosinophilic inflammation groups at exacerbation and exacerbation rates
Across all exacerbations with valid data, the prevalence of eosinophilic inflammation in sputum and blood was 23.9% (52 out of 218) and 49.7% (168 out of 338), respectively. Blood eosinophils (percentage and count) were again predictive of sputum eosinophils ≥3% at exacerbation (AUC 0.735, 95% CI 0.654–0.817 and AUC 0.729, 95% CI 0.650–0.809, respectively) (supplementary figure E1).
The median (IQR) total exacerbation rate in the first year of the study was similar in the RE and PE groups, but lower in the IE group (PE 2.04 (3.95), IE 1.02 (2.00) and RE 2.47 (3.22)). There was a significant difference in the rate of exacerbations with blood eosinophils ≥2%, with the PE group having a higher eosinophilic exacerbation rate (PE 1.38 (2.99), IE 0.00 (0.99) and RE 0.00 (0.99); p<0.001).
Longitudinal eosinophilic groups did not differ symptomatically at first exacerbation (COPD Assessment Test (CAT) and EXACT-PRO (www.exactproinitiative.com)), but there was a significant difference in blood neutrophils at exacerbation between these groups (p=0.045) and the PE group was less likely to have bacteria present (p=0.044) (table 3). There was an association between longitudinal eosinophilic phenotype and eosinophils at exacerbation, with the odds of eosinophils ≥2% at exacerbation much higher in the PE group compared with the RE group (OR 11.16, 95% CI 5.26–23.68; p<0.001). Similarly, the odds of an exacerbation being eosinophilic were nine times higher in those who had blood eosinophils ≥2% than in subjects with blood eosinophils <2% at enrolment (OR 9.16, 95% CI 4.10–20.47; p<0.001).
Characteristics at first exacerbation overall# and by longitudinal blood eosinophil groups over 12 months¶
Seasonality of eosinophilic exacerbations
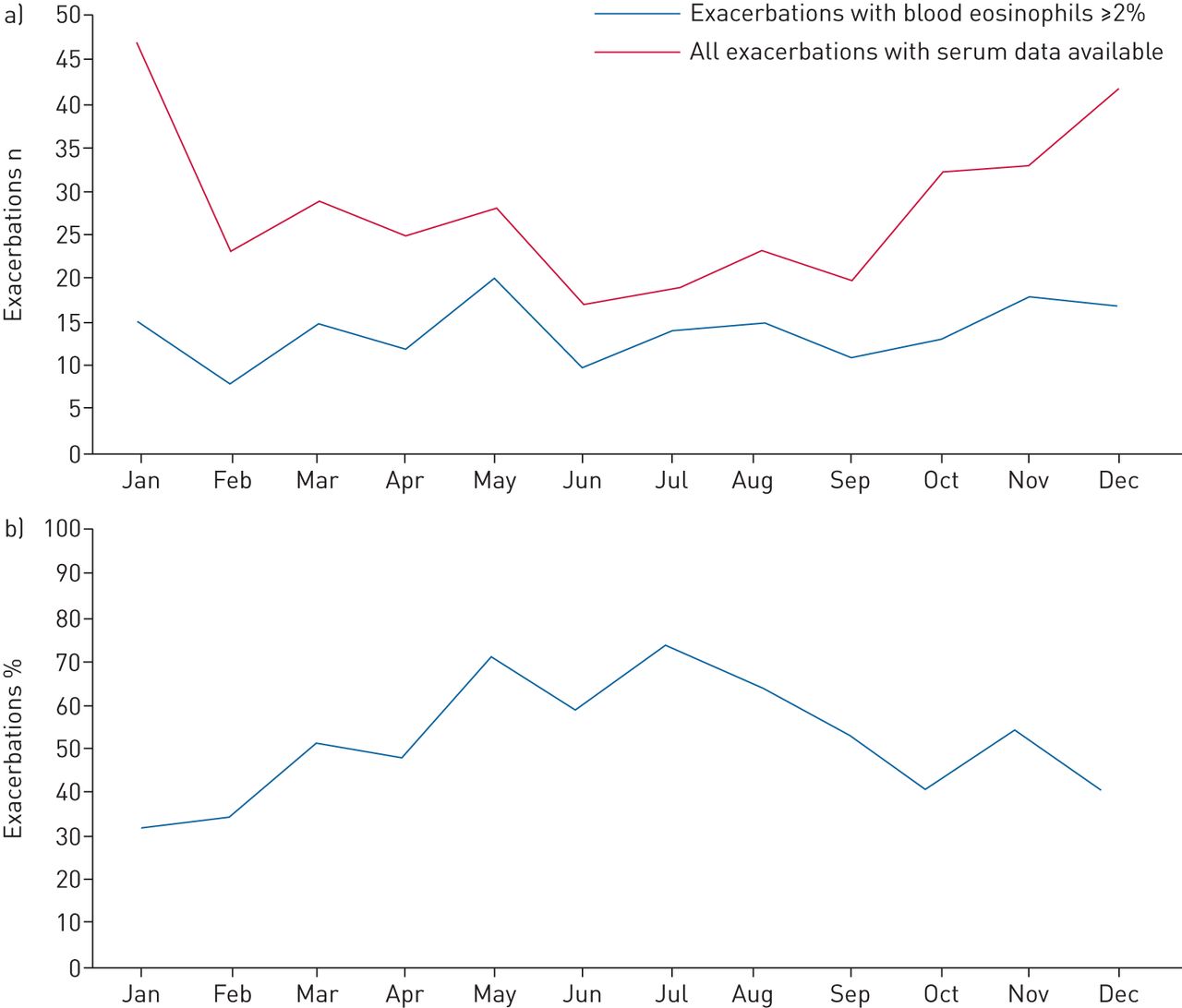
Exacerbations were more common in the winter season than in the summer season (217 and 138, respectively). The proportion of exacerbations with eosinophils ≥2% was higher in the summer season than in the winter season; however, the number of eosinophilic exacerbations per season was similar (86 out of 217 in winter and 82 out of 138 in summer) (figure 4). The PE group had similar exacerbation rates in the summer and winter seasons, while the IE and RE groups had higher exacerbation rates in the winter season (supplementary table E3).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Seasonal distribution of total and eosinophil-associated exacerbations. a) Number of total and exacerbations with blood eosinophils ≥2%. b) Proportion of exacerbations with blood eosinophils ≥2% defined as exacerbations with blood eosinophils ≥2% to total exacerbation rates in the predominantly eosinophilic, intermittent eosinophilic and rarely eosinophilic groups.
After adjusting for the contribution of multiple exacerbations by some subjects, the odds of an exacerbation having blood eosinophils ≥2% were 2.65 times higher in the summer season than in the winter season (supplementary table E4).
Both being in the PE compared with the RE group and summer season compared with winter season were independently associated with the odds of an exacerbation having blood eosinophils ≥2% (OR 11.39, 95% CI 4.68–27.72; p<0.001 and OR 2.57, 95% CI 1.37–4.85; p=0.003, respectively).
We then repeated these analyses, stratifying by eosinophilic inflammation longitudinal phenotypes. The odds of an exacerbation having eosinophils ≥2% in the summer season compared with the winter season tended to be stronger in the PE group (OR 3.73, 95% CI 1.56–8.91; p=0.003) than in the IE and RE groups (OR 2.00, 95% CI 0.32–12.59; p=0.460 and OR 1.36, 95% 0.42–4.44; p=0.606, respectively).
Airway infection and eosinophilic inflammation
The increase in the number of noneosinophilic exacerbations during the winter season may indicate underlying changes in the lung microbiome as a result of the known seasonal effects of viral and bacterial infections [19]. We therefore examined whether the association between seasonality and prevalence of blood eosinophils ≥2% at exacerbation persisted when accounting for the presence of potentially pathogenic microorganisms (PPMs) at exacerbation and found that this association did not diminish when accounting for PPMs (OR 2.39, 95% CI 1.29–4.41; p=0.005).
PPMs were present in 59% of all exacerbations with valid data (n=320) and 61% of first exacerbations (n=98). We studied PPM prevalence at first exacerbation in the longitudinal eosinophilic groups and found a significant difference in PPM prevalence; PPMs were more prevalent in the RE group (86%) than in the other two groups (PE and IE: 57% and 55%, respectively; p=0.044) (table 3). There was no such association in microbiology found between the three groups at enrolment (n=99; p=0.952) (table 2). Respiratory viruses were detected at 41% of all exacerbations with valid data (n=305) and 43.3% of first exacerbations (n=90) (table 3). We found no significant difference between the eosinophilic groups in the prevalence of the respiratory viruses either at enrolment or first exacerbation (tables 2 and 3).
The odds of having a PPM present at an exacerbation were 75% lower in the PE group compared with the RE group, but this association was of borderline significance (OR 0.25, 95% CI 0.06–1.09; p=0.065). The odds of having a PPM present were 55% lower in eosinophilic AECOPD compared with exacerbations with blood eosinophils <2%, but this was also of borderline significance (OR 0.450, 95% CI 0.240–0.998; p=0.049).
The odds of having a PPM present at exacerbation were higher in the winter season than in the summer season (OR 2.51, 95% CI 1.27–4.96; p=0.008). This seasonal effect was apparent in the PE group (OR 4.74, 95% CI 1.43–15.71; p=0.011), but no statistically significant seasonal variations in PPMs at exacerbation were detected in the IE and RE groups (OR 4.42, 95% CI 0.01–3476.74; p=0.662 and OR 1.15, 95% CI 0.29–4.56; p=0.838).
Discussion
Eosinophilic inflammation is a stable longitudinal phenotype in a substantial proportion of COPD patients, which can be predicted over 12 months by an initial blood level measurement. We report for the first time that eosinophilic inflammation was more prevalent at exacerbation in those with predominantly raised eosinophils at stable state. In the summer season, a larger proportion of exacerbations were eosinophilic, although this was driven by fewer noneosinophilic exacerbations in the summer season compared with the winter season. We also report evidence that eosinophilic exacerbations are less frequently associated with airway bacterial infection, with the prevalence of airway bacterial infection at exacerbations greater among the group who rarely had raised eosinophils over time. These findings have a potential implication for future therapeutic clinical trials and eosinophil targeted treatment with a view to stratifying patient care.
To the best of our knowledge, this is the most detailed description of inflammatory phenotype at COPD exacerbations, seasonality and infectious aetiology in longitudinal groups stratified by eosinophil levels. The seasonality of exacerbations has been previously described [21–24]. In our analysis we saw a clear seasonal pattern for all exacerbations; however, when focused on eosinophil-associated exacerbations, we report that these did not appear to show much seasonal variation, resulting in a larger proportion of exacerbations being associated with eosinophilic inflammation in the summer season. The aetiology of eosinophilic inflammation in COPD would appear to be driven by factors other than atopy as, although not formally tested, our patients had no recorded manifestations of atopic disease. Furthermore, the stable incidence of eosinophil-associated AECOPD throughout the year may suggest an intrinsic factor in triggering their incidence and requires further study.
It was previously reported that blood eosinophils ≥2% identified sputum eosinophilic inflammation at exacerbation (>3%), and was 90% sensitive and 60% specific [3]. Using the same cut-off for blood eosinophilic inflammation at enrolment in our analysis, it corresponded to the >3% sputum cut-off with similar sensitivity, but lower specificity (sensitivity 95.8% and specificity 31.8%). One reason for this discrepancy in specificity might be due to the difference in clinical states at the time of analysis; Bafadhel et al. [3] conduced the analysis at exacerbations when sputum capture is greater, whereas in our study we conducted the analysis during clinical stability. We found that at exacerbation blood eosinophils ≥2% was 79.6% sensitive and 53.9% specific. In our study the blood eosinophil count was reported up to one decimal and therefore it was not possible to apply the cut-off of 150 cells·μL–1. Using the 200 cells·μL–1 cut-off offered a similar sensitivity (95.8%), but inferior specificity (27.3%). We conducted a sensitivity analysis with the ≥200 cells·μL–1 cut-off and found that there was a significant difference in age, smoking history, exacerbation rate with raised eosinophils in the first year and presence of sputum eosinophils >3% at enrolment.
The rationale of our method to describe the longitudinal eosinophilic phenotype was to focus the analysis on subjects who were predominantly eosinophilic (allowance of one noneosinophilic event) as opposed to persistently eosinophilic (all visits were eosinophilic). This rule, we feel, represents a more pragmatic and “real-world” approach. Applying this rule, we demonstrated that 58% of subjects in our cohort had predominantly raised eosinophils over the period of 12 months. These subjects in the PE group were slightly older than those in the RE group (p=0.034) and there were trends towards a lower prevalence of current smokers, but with a greater smoking history in the PE group. Singh et al. [4] studied longitudinal eosinophilic phenotype and reported that 37.4% of subjects had persistently elevated blood eosinophils ≥2% at all visits over a period of 3 years. In a previous asthma study, a 90% rule was applied to identify persistent eosinophilic inflammation in sputum [25]. However, this rule was not applied in our cohort due to the limited number of samples available (maximum five samples). A limitation of the longitudinal phenotype method was that individuals with three visits could not be classified as intermittent eosinophilic (20 out of 99 for blood and 14 out of 80 for sputum).
Bacteria play an important role in exacerbations of COPD [26–30]. Bacterial exacerbation had been previously reported to be rarely associated with sputum eosinophilic exacerbation [3]. We investigated the prevalence of PPMs at exacerbation in the prospective eosinophilic groups and found that PPMs were far less common in the eosinophilic group. When we analysed the presence of PPMs at exacerbation in combination with blood eosinophilic inflammation, we found eosinophilic inflammation to be associated with reduced odds of PPM presence; although the magnitude of the difference was large (55% less likely), this was again of borderline significance (p=0.049). Therefore, understanding the clinical phenotype of stable inflammation may be a useful tool to stratify bacterial aetiology of exacerbations and hence antibiotic use.
While our detection of respiratory viruses at AECOPD corresponded with previously reported findings [30, 31], we observed no significant difference in the prevalence of respiratory viruses between the three groups at enrolment and at first exacerbation. Previously, Papi et al. [30] reported airway eosinophilic inflammation to be a good predictor of viral infections. However, only severe exacerbations were included in their study, whereas we captured mild, moderate and severe events in our study. Further studies across the disease spectrum are required to ascertain the mechanisms linking infection and inflammatory patterns of disease. However, it is noteworthy that there was no significant difference in use of inhaled corticosteroids and bronchial reversibility across groups, similar to previously reported studies [3, 15].
It is important to recognise that these results are representative of a cohort of moderate to very severe COPD patients with frequent exacerbations receiving a high level of clinical intervention, including inhaled corticosteroids, as part of an intensive study. This might have had an impact on the severity of exacerbations and recovery, as previous reports indicate that early therapy improves exacerbation outcomes [32]. Thus, the number of potential severe exacerbations might be smaller. In addition, the AERIS study was not originally designed, and therefore was not powered, to specifically investigate longitudinal eosinophilic inflammation and hence the numbers that were included in each eosinophilic group were limited. Larger prospective studies are required to further understand the impact of eosinophilic inflammatory status on a range of clinical outcomes.
In summary, this is the first study to report that eosinophilic inflammation is a stable phenotype in COPD and predictive of eosinophilic exacerbations. These events are seasonal in nature and relate to bacterial aetiology. Our data suggest that stratifying COPD patients into eosinophilic groups to potentially aid management is clinically relevant and potentially important, as is the consideration of season in management of exacerbations. Whether oral corticosteroids should be administered during exacerbations of COPD to predominantly eosinophilic patients, particularly outside the winter season, requires further investigation along with other stratification paradigms through well-designed intervention studies.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERJ-00853-2017_Supplement
Supplement to figure 4 ERJ-00853-2017_Figure_4
Disclosures
Supplementary Material
Author disclosures ERJ-00853-2017_Disclosures
Acknowledgements
The AERIS Study Group: J. Alnajar, R. Anderson, E. Aris, W.R. Ballou, A. Barton, S.C. Bourne, M. Caubet, S.C. Clarke, D. Cleary, C. Cohet, N.A. Coombs, K. Cox, J-M. Devaster, V. Devine, N. Devos, E. Dineen, T. Elliott, R. Gladstone, S. Harden, J. Jefferies, V.L. Kim, S. Mesia Vela, P. Moris, K.K. Ostridge, T.G. Pascal, M. Peeters, S. Schoonbroodt, K.J. Staples, A.C. Tuck, L. Welch, V. Weynants, T.M.A. Wilkinson, A.P. Williams, N.P. Williams, C. Woelk, M. Wojtas and S.A. Wootton. All members of the AERIS Study Group were involved in the planning, conduct and/or reporting of the work described in the article.
The authors would like to thank all the study volunteers for their invaluable contribution towards furthering COPD knowledge and each team member for their assistance in conducting the study. We acknowledge all members of the AERIS study group. The authors would like to also thank Geraldine Drevon and Regis Azizieh (XPE Pharma & Science (Wavre, Belgium), on behalf of GSK Vaccines (Rixensart, Belgium)) for coordination and editorial support.
Author contributions: J-M. Devaster, E. Aris, S.C. Bourne, S.A. Wootton, A.C. Tuck, S.C. Clarke, V.L. Kim and T.M.A. Wilkinson were involved in the study conception and design. J-M. Devaster, E. Aris, S.C. Bourne, S.A. Wootton, A.C. Tuck, N.P. Williams, K.K. Ostridge, K.J. Staples, S.C. Clarke, V.L. Kim and T.M.A. Wilkinson were involved in acquisition and generation of data. J-M. Devaster, E. Aris, S.C. Bourne, S.A. Wootton, N.P. Williams, K.K. Ostridge, K.J. Staples, S.C. Clarke, N.A. Coombs, V.L. Kim and T.M.A. Wilkinson were involved in data analysis and data interpretation. All authors contributed substantially to the development of the manuscript and approved the final version.
Footnotes
This article has supplementary material available from erj.ersjournals.com
Support statement: The study funder, GlaxoSmithKline Biologicals SA, designed the study in collaboration with the investigators, and coordinated collection, analysis and interpretation of data. The investigators obtained data and cared for the study participants. The authors had full access to all data in the study, contributed to the writing of the report and had final responsibility for the decision to submit for publication. Funding information for this article has been deposited with the Crossref Funder Registry.
Conflict of interest: Disclosures can be found alongside this article at erj.ersjournals.com
- Received April 24, 2017.
- Accepted July 16, 2017.
- Copyright ©ERS 2017
References










