





Abstract
Epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) are approved for second-line treatment of EGFR wild-type (EGFR-wt) nonsmall cell lung cancer (NSCLC). However, results from randomised trials performed to compare EGFR-TKIs with chemotherapy in this population did not show any survival benefit. In the era of immunotherapy, many drugs are approved for second-line treatment of EGFR-wt NSCLC and there is a need to reassess the role of EGFR-TKIs in this setting.
The Biomarkers France study is a large nationwide cohort of NSCLC patients tested for EGFR mutations. We used this database to collect clinical, biological, treatment and outcome data on EGFR-wt patients who received second-line treatment with either EGFR-TKIs or chemotherapy.
Among 1278 patients, 868 received chemotherapy and 410 received an EGFR-TKI. Median overall survival and progression-free survival were longer with chemotherapy than with an EGFR-TKI. Overall survival was 8.38 versus 4.99 months, respectively (hazard ratio 0.70, 95% CI 0.59–0.83; p<0.0001) and progression-free survival was 4.30 versus 2.83 months, respectively (hazard ratio 0.66, 95% CI 0.57–0.77; p<0.0001).
This study is helpful to guide a multiline treatment strategy for EGFR-wt NSCLC patients. Immunotherapy is approved for second-line treatment. For third-line treatment, chemotherapy results in longer overall survival and progression-free survival, and should be preferred to EGFR-TKIs.
Abstract
Biomarkers France study: second-line chemotherapy gave longer PFS and OS than TKI in NSCLC EGFR-wt patients http://ow.ly/rEXk30b3tak
Introduction
Increasingly comprehensive knowledge has emerged on the molecular pathways regulated by driver oncogenes [1]. This has resulted in the development of matched targeted therapies in patients with metastatic nonsmall cell lung cancer (NSCLC), leading to substantial clinical benefits. However, the majority of tumours lack known actionable molecular alterations. The most frequent driver mutation is that of EGFR (epidermal growth factor receptor), with a prevalence of 15% in Caucasian populations and 40–62% in Asian populations [2]. The use of EGFR tyrosine kinase inhibitors (EGFR-TKIs) is now common practice for first-line treatment of patients with EGFR sensitising mutations, leading to longer progression-free survival (PFS) intervals with fewer or at least different side-effects than chemotherapy [3–5]. Nevertheless, beyond first-line and especially for EGFR wild-type (EGFR-wt) NSCLC, the role of EGFR-TKIs is more controversial.
EGFR-TKIs were first compared with placebo in second- or third-line treatment for EGFR-wt NSCLC patients. Gefitinib did not improve overall survival in comparison with placebo in the overall population of previously treated NSCLC patients (5.6 versus 5.1 months, respectively; hazard ratio (HR) 0.89, 95% CI 0.77–1.02; p=0.087) [6]. Conversely, in unselected patients, Shepherd et al. [7] demonstrated that erlotinib could provide clinically meaningful prolongation of survival in comparison with placebo (6.7 versus 4.7 months, respectively; HR 0.70, 95% CI 0.58–0.85; p<0.001). This benefit could derive from a subset of EGFR-mutated patients, even though a benefit was shown in squamous cell carcinoma patients. More recently, afatinib showed clinical efficacy as a second-line treatment for patients with squamous cell carcinoma devoid of an activating EGFR mutation. Although the effect size was modest, afatinib did significantly reduce the risk of death compared with erlotinib and improved PFS. The median PFS was 2.6 months with afatinib compared with only 1.9 months with erlotinib (HR 0.82, 95% CI 0.68–1.00; p=0.0427) [8].
The outcomes of EGFR-wt NSCLC patients after second- or third-line treatment with gefitinib and erlotinib have also been compared with outcomes of patients who received chemotherapy. Between 2008 and 2010, three phase III randomised controlled trials compared gefitinib with docetaxel in unselected patients with previously treated advanced NSCLC. The ISTANA trial reported longer PFS, higher objective response rate (ORR), better tolerance and similar quality of life improvement with gefitinib in a population of Asian patients [9]. Although the Maruyama et al. [10] study did not meet its primary end-point of noninferiority in overall survival according to predefined criteria, the difference between gefitinib and docetaxel was not clinically significant (p=0.330). Finally, the INTEREST trial demonstrated noninferiority in overall survival of gefitinib compared with docetaxel, with a better safety profile (8.5% of patients experienced any adverse event with gefitinib versus 40.7% with docetaxel) and improvements in quality of life [11].
Conversely, Zhou et al. [2] studied the efficacy and safety of pemetrexed or gefitinib as second-line treatments for advanced EGFR-wt nonsquamous NSCLC in Asian patients. Pemetrexed showed significant improvement in PFS compared with gefitinib. However, several additional randomised trials compared erlotinib with docetaxel or pemetrexed in second-line treatment of EGFR-wt NSCLC with contrasting results. In the DELTA and TAILOR trials, erlotinib failed to improve overall survival in comparison with docetaxel [12, 13], whereas erlotinib and pemetrexed demonstrated similar overall survival (p=0.986) in a third phase III trial [14]. Finally, the TITAN trial compared erlotinib with chemotherapy in a population of EGFR-wt NSCLC patients with poor prognosis and progressive disease during or immediately after first-line chemotherapy. This trial showed no significant difference in overall survival between the two groups either (5.3 versus 5.5 months, respectively; HR 0.96, 95% CI 0.78–1.19; log-rank p=0.73) and the safety profile favoured erlotinib [15].
Although EGFR-TKIs are approved for second- or third-line treatment of EGFR-wt NSCLC, randomised trials have not shown significant differences in survival between patients treated with EGFR-TKIs and chemotherapy, precluding their routine use in this subset of patients, especially given the availability of newer therapeutic options. Indeed, efforts have been made to improve outcomes in EGFR-wt NSCLC patients in second- and third-line settings, and more therapeutic agents are now available. Anti-angiogenic treatments were studied in association with chemotherapy. Both nintedanib [16] and ramucirumab [17] in association with docetaxel improved overall survival in comparison with docetaxel alone in phase III trials. Weekly paclitaxel–bevacizumab doublet therapy also prolonged PFS compared with docetaxel in the French Cooperative Thoracic Intergroup (Intergroupe Francophone de Cancérologie Thoracique (IFCT)) phase III trial [18]. Cabozantinib, a multitarget TKI, was also recently used in combination with erlotinib, showing promising PFS in a randomised phase II trial in patients with EGFR-wt NSCLC, although this was not compared with a docetaxel-treated group [19]. Moreover, immunotherapy is now approved for second- and third-line treatment of EGFR-mutated or EGFR-wt NSCLC. Several immune checkpoint inhibitors have been investigated in this field, including nivolumab [20, 21], pembrolizumab [22], durvalumab [23] and atezolizumab [24]. Nivolumab and pembrolizumab received US Food and Drug Administration approval for second- and third-line treatment of NSCLC on the basis of phase III clinical trials reporting better efficacy and safety profile than standard chemotherapy with docetaxel [20–22].
As more and more drugs are approved for second- and third-line treatment of EGFR-wt NSCLC, there is a need to reassess EGFR-TKIs in this setting. Recent studies are challenging the use of EGFR-TKIs and their indications have to be refined. The objective of this observational study in “real life”, at the scale of a whole European country, was to provide efficacy data of EGFR-TKIs versus chemotherapy for the second-line treatment of a routine large population of EGFR-wt previously treated advanced NSCLC patients.
Patients and methods
Study design and patients
The IFCT Biomarkers France study showed that genetic tumour profiling in patients with NSCLC is possible on a nationwide scale in routine practice and could help physicians to decipher the most suitable therapeutic sequence [25]. This analysis was performed using this massive French database [25]. In this study, all patients with advanced, mainly nonsquamous NSCLC who underwent molecular testing by the 28 French National Cancer Institute (Institut National du Cancer (INCa))-certified molecular genetics centres covering the whole French territory between April 2012 and April 2013 were included. The biological, clinical and outcome data were provided by clinicians who prescribed the molecular analysis [25]. Eligible patients for the current study had advanced NSCLC without detected EGFR mutations or ALK (anaplastic lymphoma kinase) rearrangements in their tumour samples. Patients must have previously received one first-line chemotherapy regimen and a second-line treatment at time of progression, and they must have had available outcome data. Exclusion criteria were as follows: age <18 years, no first-line chemotherapy, no second-line EGFR-TKI or chemotherapy and enrolment in clinical trials.
The study was approved by a national ethics committee for observational studies (Comité d'Evaluation des Protocoles de Recherche Observationnelle) on September 28, 2011, the French Advisory Committee on Information Processing in Material Research in the Field of Health on September 22, 2011, and the National Commission of Informatics and Liberty on December 18, 2011, according to French laws; and was registered at ClinicalTrials.gov (identifier NCT01700582). All patients received information from their institution or referring clinician as recommended by competent authorities, specifying that, according to French laws, they could ask for complete access to or removal of their own collected data.
The study was funded by an unrestricted grant from the INCa to the IFCT, which did not interfere with the study design and conduct, and was sponsored by the IFCT.
Data collection
Potential prescribers of NSCLC molecular testing in one of the 28 INCa-certified molecular genetics centres certified between April 2012 and April 2013 were identified. They received written information about the study protocol and database, as well as a password to access the Biomarkers France secured online electronic Case Report Form. Patients were treated on a routine basis following national (INCa) and international (American Society of Clinical Oncology) guidelines [26]. The following data were collected: age, sex, ethnicity, smoking history, disease stage at the time of molecular testing (defined by the International Association for the Study of Lung Cancer TNM classification [27]), Eastern Cooperative Oncology Group (ECOG) performance status, type of treatment, and outcomes (best response to treatment, date of end of treatment and cause) according to RECIST (Response Evaluation Criteria in Solid Tumours [28]), PFS and overall survival.
Molecular data were provided directly by the certified molecular genetics centres to the IFCT. Molecular analyses of EGFR (exons 18–21), HER2 (human epidermal growth factor receptor 2; exon 20), KRAS (KRAS proto-oncogene, GTPase; exon 2), BRAF (B-Raf proto-oncogene, serine/threonine kinase; exon 15) and PI3KCA (phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit α; exons 9–20) mutations as well as ALK rearrangements were performed on a routine basis, as funded and recommended by the INCa. Mutations were confirmed using Sanger sequencing or more sensitive techniques, such as pyrosequencing, allele-specific PCR, fragment analysis assays, TaqMan probes or Snapshot, and a certified break-apart fluorescence in situ hybridisation assay (Vysis LSI ALK Dual Color; Abbott Molecular, Abbott Park, IL, USA) or the Ventana ALK-D5F3 immunohistochemistry assay (Ventana Medical Systems, Tucson, AZ, USA) was used to assess ALK rearrangements. Molecular genetics centres also provided the IFCT with data regarding histology, as evaluated by the referring pathologist in the sample used for molecular testing. The IFCT recorded and monitored the data.
Statistical analysis
Data were submitted for descriptive analysis. Second-line PFS was defined as the time from initiation of second-line therapy to disease progression or of death from any cause. Overall survival was measured from the date of molecular analysis to the date of death or last follow-up. Survival curves were estimated using the Kaplan–Meier method and presented as a median value with a range and a two-sided 95% confidence interval. The survival curves from the Kaplan–Meier analyses were adjusted with inverse probability weights using the methodology developed by Cole and Hernán [29], which is equivalent to direct standardisation of survival curves to distribution of patient characteristics in the combined study population (EGFR-TKI group+chemotherapy group). Briefly, all covariates measured during the baseline period or at the time of the NSCLC diagnosis were used. First, a multivariate logistic model of EGFR-TKI treatment was fitted using all baseline covariates (sex, age class, ethnicity (Asian versus Caucasian), tobacco smoking, ECOG performance status, TNM stage, type of first-line treatment, fist-line discontinuation for toxicity, first-line discontinuation for tumour progression and response to first-line treatment) in order to estimate the probability pi for a patient i being treated with EGFR-TKI, knowing the patient's baseline characteristics. Then, patients were weighted by their inverse treatment probability, i.e. 1–pi for patients treated with EGFR-TKI and 1/(1–pi) for patients treated with chemotherapy. Stabilisation of weights wi was finally achieved by replacing the numerator with the marginal probability of receiving the exposure observed, which was estimated by treatment group frequency.
For all tests, p<0.05 was considered statistically significant. Analyses were performed with SAS version 9.3 (SAS Institute, Cary, NC, USA).
Results
Patients
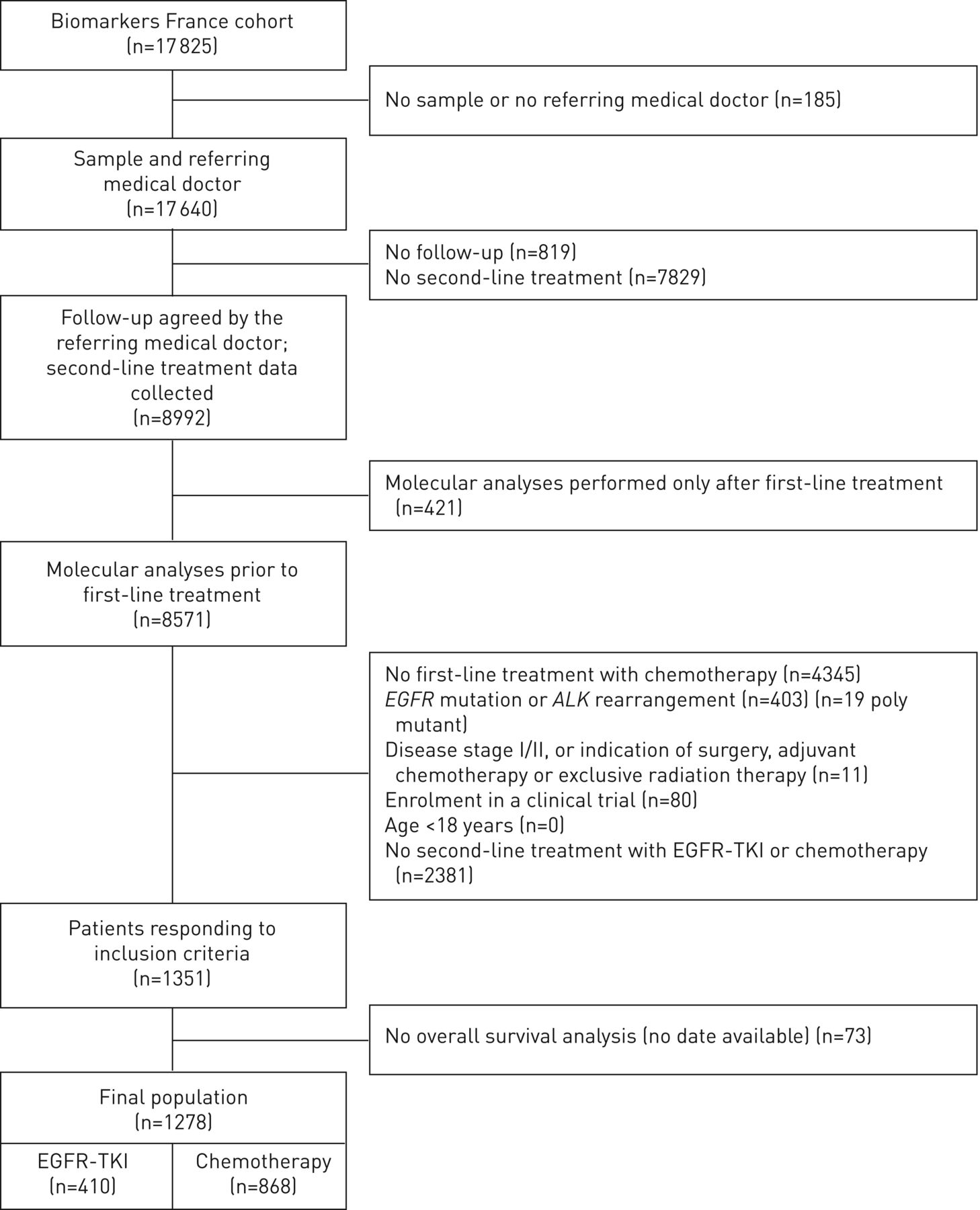
At the last monitoring data-lock on July 1, 2015, 17 640 NSCLC patients for whom a molecular test was routinely performed at the INCa-certified French genetic centres, with an identified referring practitioner, were included in the Biomarkers France study. A total of 403 patients were excluded because of EGFR mutations or ALK rearrangements and 4345 patients were excluded because they did not received first-line chemotherapy. Some of them (n=662) received targeted therapies, some of them were enrolled in clinical trials (n=239), some of them received other treatments (n=715) and some others (n=2592) were not treated. Data regarding first-line treatment were missing for 137 patients. Among 1351 patients who met the inclusion criteria, survival data were available for 1278 patients who were eventually included in the current study for efficacy and safety analyses. In total, 410 patients received second-line EGFR-TKI and 868 received second-line chemotherapy (figure 1). The baseline characteristics of these two groups of patients are described in table 1. Among the 1278 patients, 67.8% were male and 32.1% were female. There were more nonsmokers in the EGFR-TKI group than in the chemotherapy group (16.7% versus 8.8%, respectively; p<0.001) and fewer patients with KRAS-mutated tumours (24.9% versus 33.8%; p=0.001). There were more patients with ECOG performance status ≥2 and more elderly patients (≥65 years) in the EGFR-TKI group than in the chemotherapy group (27.1% versus 18.2%; p=0.001 and 46.8 versus 32.7%; p<0.001, respectively). The two groups of patients did not differ according to the type of first-line cisplatin-based doublet (taxane or pemetrexed) or ORR and disease control rate after first-line chemotherapy (disease control rate 58.9% versus 60.2% and ORR 37.7% versus 36% in chemotherapy and EGFR-TKI groups, respectively).
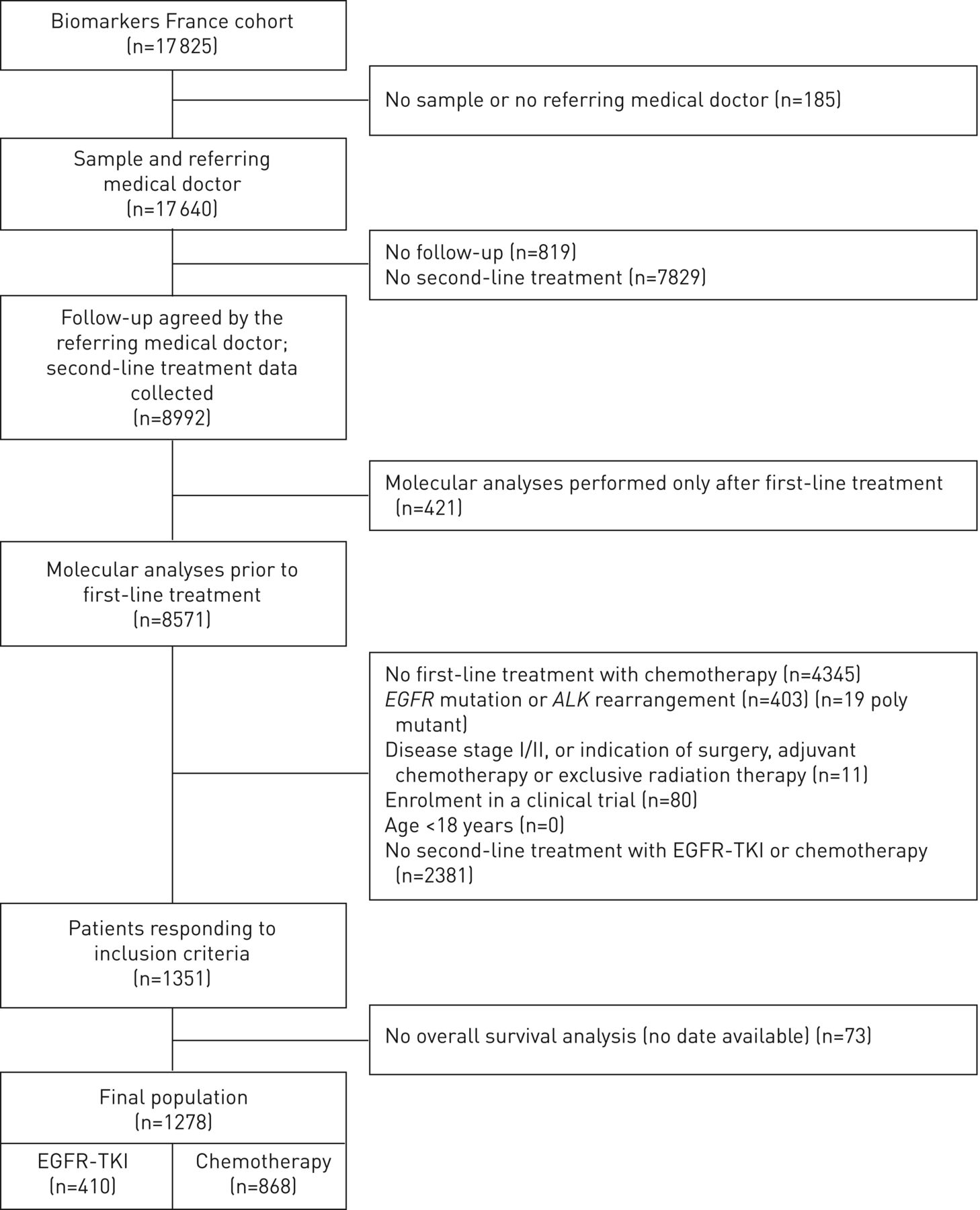
Population flowchart. EGFR-TKI: epidermal growth factor receptor tyrosine kinase inhibitor.
Baseline characteristics of the chemotherapy and epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) groups
Outcomes
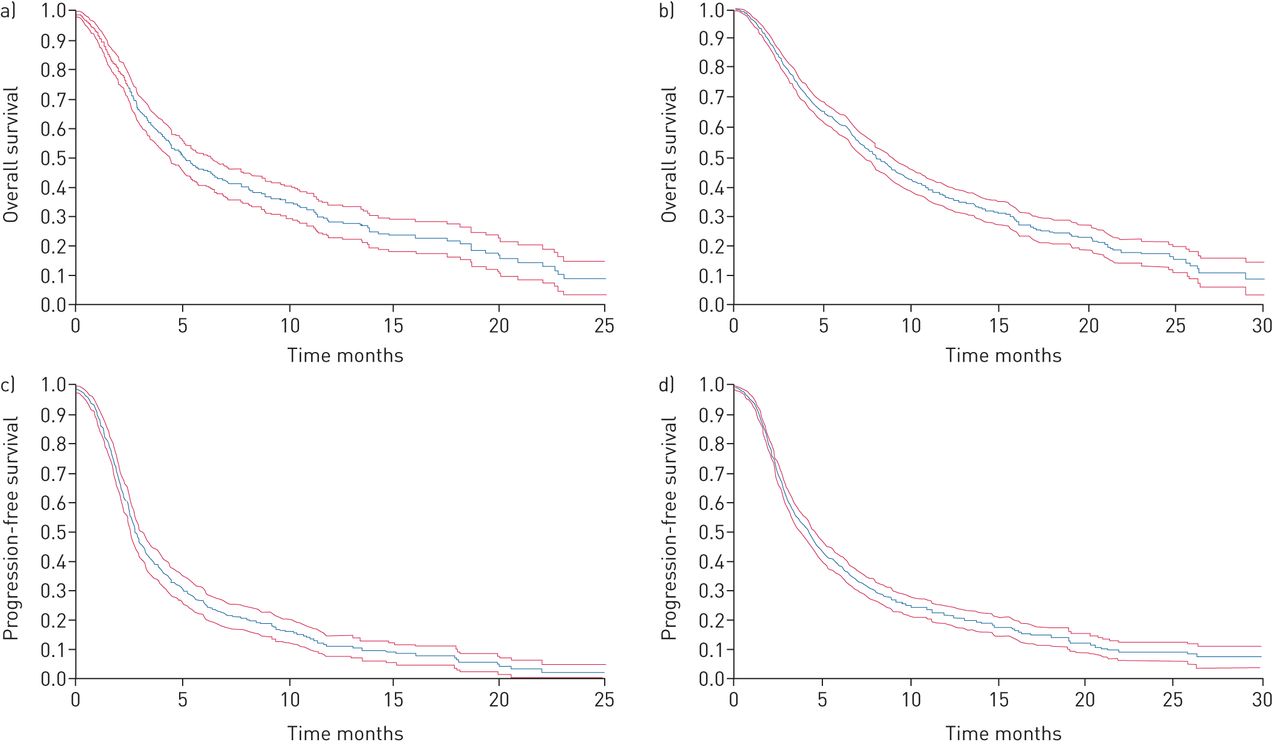
The median (range) follow-up time was 11.4 (10.3–12.4) months. Overall survival and PFS are reported in figure 2. In the group of patients treated with second-line EGFR-TKI, median (range) overall survival was 5.09 (4.44–6.37) months and PFS was 2.83 (2.60–3.15) months. In the group of patients treated with second-line chemotherapy, median (range) overall survival was 7.98 (7.33–8.87) months and PFS was 4.21 (3.81–4.60) months. Prognostic factors associated with overall survival in the two groups are reported in table 2. In multivariate analyses, only smoking status (p<0.001) and response to first-line chemotherapy (p<0.001) were associated with a longer overall survival with EGFR-TKI. ECOG performance status (p<0.001), discontinuation of first-line therapy without progression (p<0.001) and objective response or stabilisation with first-line chemotherapy (p<0.001) were associated with a longer overall survival when patients received chemotherapy.
{kind=link}
{kind=link}
a, b) Overall survival and c, d) progression-free survival of patients treated with a, c) epidermal growth factor receptor tyrosine kinase inhibitor or b, d) chemotherapy. Data are presented as median and range.
Prognostic factors of overall survival of patients treated with epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) and chemotherapy: uni- and multivariate analyses
Using the inverse probability matching method to generate adjusted survival curves, median (range) overall survival and PFS in patients treated with chemotherapy were longer than those in patients receiving EGFR-TKI: overall survival 8.38 (7.46–9.36) versus 4.99 (4.40–6.37) months, respectively (HR 0.70, 95% CI 0.59–0.83; p<0.0001) and PFS 4.30 (3.88–4.83) versus 2.83 (2.56–3.12) months, respectively (HR 0.66, 95% CI 0.57–0.77; p<0.0001). Additionally, median (range) 1-year overall survival was 37.8% (33.7–42.3%) in the chemotherapy group versus 28.0% (22.6–34.6%) in the EGFR-TKI group, leading to a clinically meaningful 10% difference in survival (p=0.002).
Finally, discontinuation of the second-line treatment for toxicity did not significantly differ between groups (6.9% and 7.1% for chemotherapy and EGFR-TKI groups, respectively; HR 0.66, 95% CI 0.57–0.77; p<0.0001).
Discussion
In the era of immunotherapy and because of the recent advances made in second-line treatment of patients with EGFR-wt NSCLC, there was a need to reassess the role of EGFR-TKIs in this field, taking into account the controversial data from early trials. The Biomarkers France study [25] is the largest nationwide cohort of NSCLC patients screened for EGFR mutations and ALK rearrangements, and provided us with clinical, biological and outcome data from a daily practice population of NSCLC patients. We were able to identify a large cohort of 868 patients treated with second-line chemotherapy and 410 patients treated with second-line EGFR-TKI, and to describe the clinical characteristics and outcomes of these two groups of patients. Although these data do not come from a randomised trial, leading to different characteristics between the groups, with slightly more nonsmoking patients with ECOG performance status ≥2 and elderly patients treated with EGFR-TKIs, the size of these two groups supported reliable data. Furthermore, the inverse probably matching method confirmed clinically significant survival differences. PFS and overall survival of EGFR-wt patients treated with second-line EGFR-TKI were shorter than those observed in patients receiving second-line chemotherapy when survival was adjusted for confounding characteristics. A major issue in the current study is the fact that EGFR-wt patients in this study had no ALK rearrangement and their KRAS status (wild-type or mutated) consisted of one of the adjustment variables in the adjusted survival analysis. In trials comparing second-line EGFR-TKI with either placebo or chemotherapy (pemetrexed or docetaxel) in patients with EGFR-wt tumours, KRAS status was not systematically assessed to check whether there was an imbalance between therapeutic arms with respect to KRAS-activating mutations. Only the BR.21 INTEREST and TAILOR trials reported either that patients with mutant KRAS tumours actually did not benefit from erlotinib [30] or that KRAS mutation had no impact on survival with EGFR-TKI treatment [11]. Here, the poor outcomes with second-line EGFR-TKIs could not be attributed to the KRAS-mutated subset, supporting intrinsic superiority of second-line chemotherapy in EGFR-wt Caucasian patients compared with EGFR-TKIs. Noticeably, in both groups of patients, those who derived a substantial benefit from first-line therapy also benefited from second-line therapy independent of what the second-line regimen was. We were also able to identify prognostic factors of overall survival in each group that could be helpful to guide second-line treatment and to plan a multiline strategy. Indeed, nonsmoking patients treated with EGFR-TKIs derived a significant benefit in terms of overall survival (HR 0.43, 95% CI 0.28–0.66; p<0.001), whereas, not surprisingly, response to first-line chemotherapy and good performance status were associated with better outcomes with both treatments.
This retrospective “real-life”, large study provides clues to improve the management of EGFR-wt NSCLC patients treated with EGFR-TKIs. As encouraging results have also been observed with immune checkpoint inhibitors in this group of patients, a phase IB trial was designed to study the combination of gefitinib (EGFR-TKI) and durvalumab (anti-PD-L1) in the second-line setting. The preliminary results of the TATTON study were presented recently [31]. Unfortunately, this study had to be stopped prematurely due to a high rate of toxicity; up to 64% of patients in the expansion cohort experienced treatment-induced pneumonitis. This again highlights the need for a better knowledge of clinical factors associated with EGFR-TKI efficacy in order to guide the prescription of EGFR-TKIs and the prognostic factors identified in the current study should be used to design new trials in this group of patients when testing EGFR-TKI-containing therapeutic combinations.
A possible limitation of our study, which is also its strength, is that data were collected prospectively during a period of time when immune checkpoint inhibitors were not yet approved. For this reason, clinical characteristics, outcomes and prognostic factors of EGFR-TKIs in this population could not be compared directly with those of patients treated with second-line immunotherapy. Although we cannot exclude that imbalance in third-line treatments could have induced overall survival differences, this hypothesis is unlikely because of their modest efficacy in the pre-immunotherapy era, actually strengthening our results.
Therefore, we feel that this study is helpful to guide multiline treatment strategies for EGFR-wt NSCLC patients, especially the rare subgroup of never-smoker, KRAS-wt patients. While chemotherapy remains the standard first-line approach with immunotherapy recently becoming the standard second-line therapy, it is not yet clear whether patients should receive chemotherapy or EGFR-TKI in the third-line setting. Whereas the current study was performed in the second-line setting, we can hypothesise from the results that EGFR-TKIs should be chosen preferentially for nonsmokers. Conversely, for all other patients, the Biomarkers France study suggests that chemotherapy should be favoured and a switch to EGFR-TKIs could be performed as fourth-line treatment, although no clear data are available yet in this setting.
Disclosures
Supplementary Material
C. Audigier-Valette ERJ-00514-2017_Audigier-Valette
F. Barlesi ERJ-00514-2017_Barlesi
D. Moro-Sibilot ERJ-00514-2017_Moro-Sibilot
V. Westeel ERJ-00514-2017_Westeel
M. Wislez ERJ-00514-2017_Wislez
G. Zalcman ERJ-00514-2017_Zalcman
Acknowledgements
The Biomarkers France contributors listed here are the treating physicians who provided data for five or more patients for the current study, not included in the list of authors: Faraj Al Freijat (CHBM, Service de Pneumologie, Belfort), Jean Bernard Auliac (CH François Quesnay, Hôpital de Mantes, Service de Pneumologie, Mantes la Jolie), Laurence Bigay Game (Hôpital Larrey, Service de Pneumologie, Toulouse), Anne-Sophie Blanchet-Legens (Hôpital St Joseph St Luc, Service de Pneumologie, Lyon), Sonia Blandin (CHU Villefranche, Service de Pneumologie, Villefranche sur Saône), Jacques Cadranel (AP-HP, Hôpital Tenon, Service de Pneumologie, Paris), Juliette Camuset (CH Victor Dupouy, Service de Pneumologie, Argenteuil), Thierry Chinet (AP-HP, Hôpital Ambroise Paré, Service de Pneumologie, Boulogne Billancourt), Alexis Cortot (CHRU Lille, Hôpital Albert Calmette, Service d'Oncologie Thoracique, Lille), Bruno Coudert (Centre Georges François Leclerc, Service d'Oncologie Médicale, Dijon), Catherine Daniel (Institut Curie, Service d'Oncologie Médicale, Paris), Chantal Decroisette (CH Annecy, Service de Pneumologie, Pringy), Toufik Didi (CH Annecy, Service de Pneumologie, Pringy), Frédérique Duboeuf (CHU Saint Etienne, Service de Pneumologie, Saint Etienne), Pascale Dubray-Longeras (Centre Jean Perrin, Service d'Oncologie Médicale, Clermont Ferrand), Elizabeth Fabre (AP-HP, HEGP, Service d'Oncologie Médicale, Paris), Pascal Foucher (CHU Bocage Central, Hôpital de Semaine Cardio-Pneumologie, Dijon), Séverine Fraboulet-Moreau (Hôpital Foch, Service de Pneumologie, Suresnes), Cédric Galichet (CH Robert-Pax, Service de Pneumologie, Sarreguemines), Georges Garnier (CH Princesse Grace, Service Médecine Interne, Hématologie, Oncologie, Monaco), Jean-Pierre Gury (CHI Haute-Saône-Vesoul, Service de Pneumologie et Allergologie, Vesoul), Khaldoun Hakim (CH Auxerre, Service de Pneumologie, Maladies Respiratoires, Auxerre), Werner Hilgers (Institut Sainte Catherine, Service d'Oncologie, Médecine interne, Avignon), Isabelle Huet (Hôpital Larrey, Service de Pneumologie, Toulouse), Henri Janicot (CHU, Hôpital Gabriel Montpied, Service de Pneumologie, Clermont Ferrand), Sylvie Julien (Hôpital Combarel, Service de Pneumologie, Rodez), Lise Kiakouama (Hôpital Croix Rousse, Service de Pneumologie, Lyon), Stephano Chong Hun Kim (CHBM, Service d'Oncologie, Montbeliard), Régine Lamy (CH Bretagne Sud, Service d'Oncologie, Lorient), Thierry le Chevalier (Gustave Roussy, Comité de Pathologie Thoracique, Villejuif), Jacques le Treut (CH Pays d'Aix, Service de Pneumologie, Maladies Respiratoires, Aix en Provence), Julien Legodec (HIA Sainte Anne, Service de pneumologie, Toulon), Hervé Lena (CHU Pontchaillou, Service de Pneumologie, Rennes), Anne Madroszyk-Flandin (Institut Paoli Calmettes, Service Cancérologie Médicale, Marseille), Marie Marcq (CHD La Roche sur Yon Les Oudairies, Service de Pneumologie, La Roche sur Yon), Michel Martin (Hôpital de Girac, Service de Pneumologie, Saint Michel), Yves Martinet (CHRU Nancy, Hôpital Brabois, Service de Pneumologie, Vandoeuvre Les Nancy), Bénédicte Mastroianni (Hôpital Louis Pradel, Service de Pneumologie, Bron), Olivier Menard (CHRU Nancy, Hôpital Brabois, Service de Pneumologie, Vandoeuvre Les Nancy), Patrick Merle (CHU, Hôpital Gabriel Montpied, Service de Pneumologie, Clermont Ferrand), Isabelle Monnet (CHIC Créteil, Service de Pneumologie, Créteil), Lionel Moreau (Hôpitaux Civils, Service de Pneumologie, Colmar), Pierre Morinet (Clinique Pasteur, Service de Pneumologie, Toulouse), Jean Loup Mouysset (Clinique Parc Rambot, Service d'Oncologie Médicale, Aix en Provence), Jean-Marc Naccache (AP-HP Hôpital Tenon, Service de Pneumologie, Paris), Cécilia Nocent Ejnaini (CH Côte Basque, Service de Pneumologie, Bayonne), Luc Odier (CH Villefranche sur Saône, Service de Pneumologie, Gleizé), Dominique Paillotin (CHU Rouen, Hôpital de Bois-Guillaume, Service de Pneumologie, Bois-Guillaume), Gavin Plat (Hôpital Larrey, Service de Pneumologie, Toulouse), Alain Poisson (Hôpital Saint Joseph, Service de Pneumologie, Allergologie et Oncologie Thoracique, Marseille), Michel Poudenx (Centre Antoine Lacassagne, Service de Pneumologie, Nice), Alain Prevost (Institut Jean Godinot, Service d'Oncologie Médicale, Reims), Nathalie Prim (Nouvel Hôpital Civil, Service de Pneumologie, Strasbourg), Christophe Raspaud (Clinique Pasteur, Service d'Oncologie Thoracique, Toulouse), Patrice Ray (CHU Carémeau, Service de Pneumologie, Nimes), Jean-Michel Rodier (AP-HP, Hôpital Bichat, Service de Pneumologie, Paris), Philippe Romand (Hôpital Georges Pianta, Service de Pneumologie, Thonon les Bains), Daniel Sandron (CH Saint Nazaire, Service de Pneumologie, Saint-Nazaire), Pierre-Jean Souquet (CH Lyon-Sud, Service de Pneumologie, Pierre-Bénite), Georges Thomas (Hôpital Saint Joseph, Service de Pneumologie, Allergologie et Oncologie Thoracique, Marseille), Julie Tillon-Strozyk (Hôpital Charles Nicolle, Service de Pneumologie, Rouen), Thierry Urban (CHU Angers, Service de Pneumologie, Angers), Fabien Vaylet (HIA Percy, Service de Pneumologie, Clamart), Rémi Veillon (Hôpital du Haut Lévêque, Service des Maladies Respiratoires, Pessac) and Annie Wdowik (CH Bretagne Atlantique Site de Vannes, Service d'Oncologie, Vannes).
Footnotes
Clinical trial: This study is registered at www.clinicaltrials.gov with identifier number NCT01700582.
Support statement: This study was funded by the Institut National du Cancer. Funding information for this article has been deposited with the Crossref Funder Registry.
Conflict of interest: Disclosures can be found alongside this article at erj.ersjournals.com
- Received March 13, 2017.
- Accepted April 18, 2017.
- Copyright ©ERS 2017
References










