





Figures
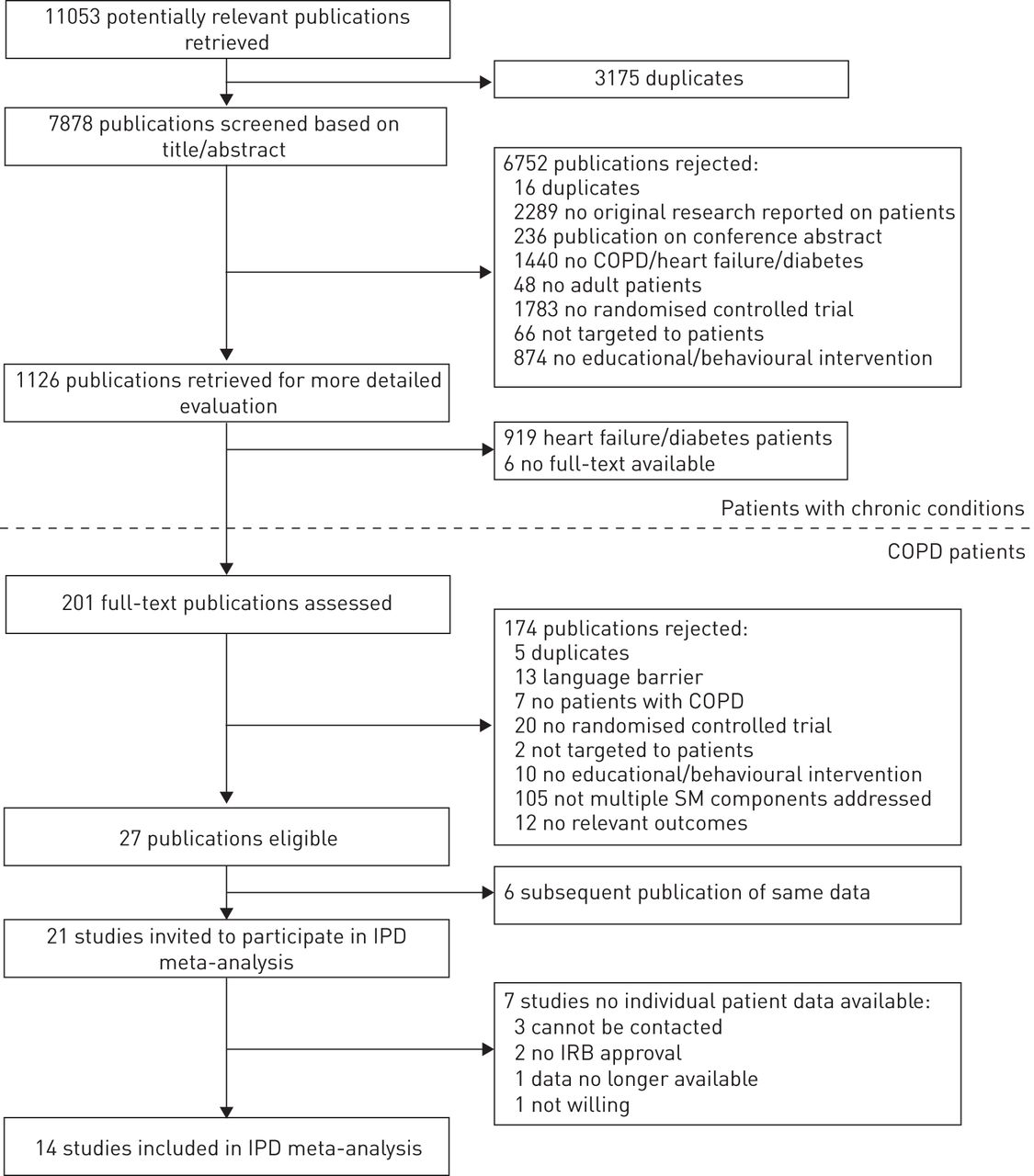
- FIGURE 1
Flowchart of study selection for individual patient data meta-analysis. The present study was conducted as part of a larger project including patients with other chronic conditions (i.e. patients with heart failure or type 2 diabetes mellitus). COPD: chronic obstructive pulmonary disease; SM: self-management; IPD: individual patient data; IRB: institutional review board.
{kind=link}
Tables
- TABLE 1
Baseline characteristics of chronic obstructive pulmonary disease patients in control and self-management intervention arm included in the individual patient data meta-analysis
Characteristic Control Intervention Total Patients n 1492 1790 3282 Sex Male 999 (67.0) 1151 (64.3) 2150 (65.6) Female 492 (33.0) 639 (35.7) 1131 (34.5) Age 68.3±9.6 67.9±9.6 68.1±9.6 FEV1 % predicted 47.3±18.8 48.0±18.9 47.7±18.9 Dyspnoea# Low level of breathlessness 151 (37.4) 275 (50.2) 426 (44.7) High level of breathlessness 253 (62.6) 273 (49.8) 526 (55.3) Level of education Primary education or below 313 (39.6) 391 (38.3) 704 (38.9) Secondary education 351 (44.4) 456 (44.7) 807 (44.6) Higher education 127 (16.1) 173 (17.0) 300 (16.6) Smoking status Current nonsmoker 1036 (71.8) 1225 (71.1) 2261 (71.4) Current smoker 407 (28.2) 499 (28.9) 906 (28.6) Data are presented as n (%) or mean ±sd. FEV1: forced expiratory volume in 1 s. #: based on score (modified) Medical Research Council (MRC) dyspnoea scale [31] and categorised according to Global Initiative for Chronic Obstructive Lung Disease guidelines [2], MRC ≥3 or mMRC ≥2 indicates high level of breathlessness.
- TABLE 2
Description of trials on self-management in COPD patients included in the individual patient data meta-analysis
Author [ref] Country Sample size Recruitment year Setting Patient population Control group Intervention group Duration of intervention months Outcomes collected Time-point months Bischoff [5] The Netherlands 165 2004 General practice 0.3 ≤FEV1/FVC <0.7, no stability criteria Usual care (contact with general practitioner) 1) 2–4 individual sessions by nurse, action plan, follow-up 6 telephone calls
2) 2–4 routine monitoring sessions by nurse24 HRQoL 6, 12 Bourbeau [8] Canada 191 1998 Clinic/ hospital 0.25 <FEV1 % pred <0.7, ≥1 exacerbation in last year Usual care (contact with general practitioner or specialist, access to provincial health programme) 7 individual sessions by nurse/respiratory therapist/physiotherapist, 1 physical exercise session, workbook, action plan, follow-up monthly telephone calls 12 HRQoL, hospitalisations (AC and respiratory related) 12 Bucknall [6] UK 464 2007 Clinic/ hospital FEV1/FVC <0.7, post-exacerbation hospitalisation Usual care (contact with general practitioner, specialists or both, access to 24 h helpline) 4 individual home visits by nurse, action plan, follow-up by home visits at least every 6 weeks 12 HRQoL, hospitalisations (AC and respiratory related), mortality 6, 12 Casas [33] Belgium/Spain 155 2005 Clinic/ hospital Confirmed COPD, post-exacerbation hospitalisation Usual care (contact with general practitioner) 1 individual session, minimally 1 home visit by nurse/physician, action plan, follow-up 4 telephone calls 1 HRQoL, hospitalisations (respiratory related), mortality 6, 12 Coultas [28] USA 217 2000 General practice FEV1/FVC <0.7, no stability criteria Enhanced usual care (two additional educational booklets for COPD) 1) 1 individual session by nurse, follow-up 6 telephone calls
2) 1 individual session by nurse, follow-up 7 telephone calls6 HRQoL, hospitalisations (AC and respiratory related), mortality 6 Effing [29] The Netherlands 153 2004 Clinic/ hospital 0.25 ≤FEV1 % pred <0.8, stable for ≥1 month Enhanced usual care (4 group sessions on self-management, booklet on self-management, access to helpline) 1) 4 group sessions by nurse/physiotherapist, action plan, physical training for 11 months, follow-up 3 telephone calls
2) 4 group sessions by nurse/ physiotherapist, action plan, follow-up 3 telephone calls
3) 4 group sessions by nurse/ physiotherapist, physical training for 11 months12 HRQoL, hospitalisations (respiratory related), mortality 6, 12 Gallefoss [34] Norway 53 1994 Clinic/ hospital 0.4 ≤FEV1 % pred <0.8, no stability criteria Usual care (contact with general practitioner) 2 group sessions, minimally 2 individual sessions by multidisciplinary team, action plan 0.5 Hospitalisations (respiratory related) 12 McGeoch [35] New-Zealand 161 2002 General practice FEV1/FVC <0.7, ≥1 exacerbation in last year Usual care (contact with general practitioner, not standardised education by practices, access to action plan denied) 1 individual session by nurse, action plan 1 day HRQoL, Hospitalisations (AC and respiratory related), mortality 6, 12 Monninkhof [36] The Netherlands 248 1999 Clinic/ hospital 0.25 ≤FEV1 % pred <0.8, stable for ≥1 month Enhanced usual care (contact with general practitioner, smoking cessation programme, inhalation instructions, access to helpline) 5 group sessions by nurse/physiotherapist, action plan, physical training programme for 2 years 4 HRQoL, hospitalisations (respiratory related), mortality 6, 12 Nguyen [30] USA 125 2007 Combination FEV1/FVC <0.7, stable for ≥1 month Enhanced usual care (home visit, monthly group sessions on general health education, biweekly telephone calls) 1) 1 home visit, 6 group sessions by nurse, educational booklet, follow-up biweekly telephone calls
2) 1 home visit, 6 text chat sessions with nurse, digital learning modules, follow-up biweekly e-mails12 HRQoL 6, 12 Rice [9] USA 743 2004 Clinic/ hospital Confirmed COPD, ≥1 exacerbation in last year Usual care (including a hand-out on COPD and access to 24 h helpline) 1 group session by respiratory therapist, individualised action plan, follow-up monthly telephone calls 12 HRQoL, hospitalisations (AC and respiratory related), mortality 6, 12 Taylor [37] UK 116 2007 General practice FEV1 <0.8% pred, ≥1 exacerbation in last year Usual care (not standardised, contact with general practitioner or specialists) 7 group sessions by lay peer tutor, action plan 1.6 HRQoL, hospitalisations (respiratory related), mortality 6 Trappen-burg [38] The Netherlands 233 2008 Combi-nation FEV1/FVC <0.7, no stability criteria Usual care (not standardised, contact with respiratory nurse and general practitioner, possible referral to physiotherapist/dietician) 1 individual session by nurse, action plan, follow-up 2 telephone calls 4 HRQoL, hospitalisations (respiratory related), mortality 6 Zwar [39] Australia 258 2002 General practice FEV1/FVC <0.7, ≥1 exacerbation in last year Usual care (contact with general practitioner, written COPD guidelines) 2 home visits by nurse, 2 visits to physician, action plan, follow-up 5 telephone calls 6 HRQoL, hospitalisations (AC and respiratory related), mortality 6, 12 AC: all-cause; COPD: chronic obstructive pulmonary disease; FEV1: forced expiratory volume in 1 s; FVC: forced vital volume; HRQoL: health-related quality of life.
- TABLE 3
Programme characteristics of the self-management interventions in patients with chronic obstructed pulmonary disease included in the individual patient data meta-analysis
Author [ref] Recruitment year Standardised training Multidisciplinary team Peer contact Logs kept Goals set Problem solving Support allocation Easy telephone access Action plan with prescription Gallefos [34] 1994 + + + + + Bourbeau [8] 1998 + + + + + Monninkhof [36] 1999 + + + + + + + + Coultas [28] 2000 + Coultas [28] 2000 + McGeoch [35] 2002 + + Bischoff [5] 2004 + + + + Bischoff [5] 2004 Effing [29] 2004 + + + + + + + + + Effing [29] 2004 + + + + + + + + + Effing [29] 2004 + + + + + + Rice [9] 2004 + + + + Casas [33] 2005 + + + + + + Zwar [39] 2006 + + + + Bucknall [6] 2007 + + + + + + Nguyen [30] 2007 + + + + + Nguyen [30] 2007 + + + + + Taylor [37] 2007 + + + + + Trappenburg [38] 2008 + Totals# 15 8 9 9 7 10 9 8 11 +: characteristic present in intervention. #: interventions N=19.
- TABLE 4
Primary analysis of effects of self-management interventions and characteristics in patients with chronic obstructive pulmonary disease included in the individual patient data meta-analysis
Outcome Studies Events/patients control Events/patients intervention Analysis Effect measured Effect p-value# I2 % Health-related quality of life 6 months 9 811 1065 Intervention effect SMD 0.05 (−0.05–0.15) 0.0 No significant components 12 months 10 1233 1431 Intervention effect SMD 0.08 (0.00–0.16) 0.0 No significant components All-cause hospitalisation Time to first event 4 381/773 334/786 Intervention effect HR 0.80 (0.69–0.93) 51.0 4 381/773 334/786 Intensity (per contact) 0.99 (0.98–1.00) 0.007 4 381/773 334/786 Duration (per month) 0.98 (0.97–0.99) 0.002 6 months 6 282/959 256/1075 Intervention effect RR 0.81 (0.67–0.97) 47.8 6 282/959 256/1075 Intensity (per contact) 0.98 (0.96–1.00) 0.013 6 282/959 256/1075 Duration (per month) 0.96 (0.92–0.99) 0.025 12 months 5 398/886 351/931 Intervention effect RR 0.84 (0.73–0.96) 44.3 5 398/886 351/931 Intensity (per contact) 0.98 (0.97–1.00) 0.013 5 398/886 351/931 Duration (per month) 0.98 (0.96–1.00) 0.012 Respiratory-related hospitalisation Time to first event 6 276/928 218/944 Intervention effect HR 0.79 (0.66–0.94) 20.6 2 119/354 115/343 Keeping logs 0.99 (0.77–1.28) 0.015 4 157/574 103/601 Not keeping logs 0.64 (0.50–0.82) 6 months 8 200/1114 173/1233 Intervention effect RR 0.87 (0.69–1.09) 0.0 2 65/409 46/450 Peer contact 0.64 (0.45–0.92) 0.049 6 135/705 127/783 No peer contact 1.02 (0.76–1.38) 12 months 9 347/1163 268/1263 Intervention effect RR 0.77 (0.64–0.93) 0.0 No significant components Mortality Time to event 7 91/1049 91/1071 Intervention effect HR 1.02 (0.76–1.37) 0.0 4 39/481 52/502 Problem solving/ support skills 1.39 (0.91–2.11) 0.033 3 52/568 39/569 No problem-solving/support skills 0.73 (0.48–1.11) 6 months 9 52/1161 54/1329 Intervention effect RR 1.06 (0.62–1.82) 0.0 No significant components 12 months 7 95/1041 94/1141 Intervention effect RR 1.04 (0.64–1.69) 0.0 No significant components Data are presented as n, n/n or effect (95% CI), unless otherwise stated. Results are only presented if a programme characteristic showed an effect with p<0.05 in the primary analysis. CI: confidence interval, HR: hazard ratio, RR: risk ratio, SMD: standardised mean difference. #: p-value for Q-test for heterogeneity to test for modification of effect by the programme characteristic.
- TABLE 5
Secondary analysis of effects of programme characteristics in patients with chronic obstructive pulmonary disease included in the individual patient data meta-analysis adjusted for other characteristics
Outcome Studies Events/patients control Events/patients intervention Variable Effect measure Effect Health-related quality of life 6 months NA 12 months NA All-cause hospitalisation Time to first event 4 381/773 334/786 Intensity (per contact) HR 1.08 (1.02–1.14) 4 381/773 334/786 Duration (per month) 0.90 (0.83–0.97) 6 months 6 282/959 256/1075 Intensity (per contact) RR 1.26 (0.57–2.80) 6 282/959 256/1075 Duration (per month) 0.76 (0.31–1.86) 12 months 5 398/886 351/931 Intensity (per contact) RR 1.00 (0.61–1.64) 5 398/886 351/931 Duration (per month) 1.02 (0.47–2.24) Respiratory-related hospitalisation Time to first event 6 276/928 218/944 Keeping logs HR 0.47 (0.26–0.83) 6 months 8 200/1114 173/1233 Peer contact RR 0.74 (0.00–1119.00)# 12 months NA Mortality Time to event 7 91/1049 91/1071 Problem-solving/support skills HR 14.03 (0.23–851.99)# 6 months NA 12 months NA Data are presented as n, n/n or effect (95% CI), unless otherwise stated. Results are only presented if a programme characteristic showed an effect with p<0.05 in the primary analysis. CI: confidence interval; NA: not available; HR: hazard ratio; RR: risk ratio. #: over fitted model due to low number of cases, no interpretation possible.
Supplementary material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
- Supplementary tables and references - Tables S1-S5 and references
Disclosures










