





Abstract
Pulmonary arteriovenous malformations (PAVMs) are associated with severe neurological complications in hereditary haemorrhagic telangiectasia (HHT). Transthoracic contrast echocardiography (TTCE) is recommended for screening of pulmonary right-to-left shunts (RLS). Although growth of PAVMs is shown in two small studies, no studies on follow-up with TTCE exist.
All HHT patients underwent a second TTCE 5 years after initial screening. Patients with a history of PAVM embolisation were excluded. Pulmonary RLS grade on TTCE after 5 years was compared to the grade at screening.
200 patients (53.5% female, mean±sd age at screening 44.7±14.1 years) were included. Increase in RLS grade occurred in 36 (18%) patients, of whom six (17%) underwent embolisation. The change in grade between screening and follow-up was not more than one grade. Of patients with nontreatable pulmonary RLS at screening (n=113), 14 (12.4%) underwent embolisation. In patients without pulmonary RLS at initial screening (n=87), no treatable PAVMs developed during follow-up.
Within 5 years, no treatable PAVMs developed in HHT patients without pulmonary RLS at initial screening. Increase in pulmonary RLS grade occurred in 18% of patients, and never increased by more than one grade. Of patients with nontreatable pulmonary RLS at initial screening, 12% underwent embolisation.
Abstract
Within 5 years, no treatable PAVMs developed in HHT patients who did not have pulmonary RLS at initial screening http://ow.ly/XoZLQ
Introduction
Pulmonary arteriovenous malformations (PAVMs) are abnormal vessels that replace the normal capillaries between the pulmonary arterial and venous circulation [1]. Up to 90% of PAVMs are associated with hereditary haemorrhagic telangiectasia (HHT), a rare autosomal dominant inherited disorder [2–4]. HHT is characterised by the presence of direct artery-to-vein communications, which vary from small telangiectasia (dilated microvessels) in skin and mucous membranes to large arteriovenous malformations, predominantly localised in the brain, liver and lungs [1, 5]. HHT consist of two main types: HHT type 1 and HHT type 2, which are caused by mutations in the ENG and ACVRL1 genes, respectively [6, 7].
PAVMs bypass the normal pulmonary capillary filter and result in a permanent anatomic right-to-left shunt (RLS). PAVMs are therefore associated with severe neurological complications due to paradoxical emboli of both thrombotic and septic origin [1]. Depending on HHT type, the prevalence of a pulmonary RLS is 35–85% [1, 8]. In order to reduce the risk of neurological complications, patients can be safely treated with transcatheter embolotherapy, an endovascular intervention that occludes the feeding artery of the PAVM with a vascular plug or coils [9, 10].
Transthoracic contrast echocardiography (TTCE) has an excellent sensitivity and negative predictive value for the presence of PAVMs with low risks and costs. It is therefore recommended as the first-line screening technique for PAVMs in all persons with suspected HHT [3, 8, 11, 12]. Importantly, two recently published studies by Velthuis and colleagues [1, 13] demonstrated that small pulmonary RLS are not associated with neurological complications and that pulmonary RLS on TTCE predicts the size of PAVMs on chest computed tomography (CT), and their feasibility for subsequent transcatheter embolisation.
Unfortunately, the recommendations for follow-up of pulmonary RLS are mainly based on expert opinion and there is no literature on long-term follow-up with TTCE. However, there are a few small studies, which included patients after embolisation, that demonstrate growth of PAVMs despite embolisation [9, 10]. Besides, HHT is known for its age-related penetrance. Therefore we hypothesised that in HHT patients without treatable PAVMs at screening, an increase in pulmonary RLS may occur during follow-up. We present the first study on the 5-year follow-up of pulmonary RLS with TTCE in HHT patients.
Methods
Study population
All patients with a definite HHT diagnosis who were screened for PAVMs using TTCE between September 2004 and June 2010 were invited for 5-year follow-up at the St Antonius Hospital (Nieuwegein, the Netherlands), an HHT centre of excellence. The HHT diagnosis was based on genetic testing or presence of three or more clinical criteria [3], which consist of spontaneous and recurrent epistaxis, telangiectasia at characteristic sites, visceral lesions and a first-degree relative with HHT. Patients with history of PAVM embolisation were excluded.
The study was approved by the institutional medical ethics committee (R&D/Z14.059).
Contrast echocardiography
TTCE at screening was performed using a Philips Sonos 7500 ultrasound instrument and a S3 transducer or a Philips IE33 ultrasound instrument and a S5–1 transducer (Philips Medical Systems, Best, the Netherlands). The TTCE at follow-up was performed using a Philips IE33 ultrasound instrument and a S5–1 transducer or a General Electronic Vivid S6 ultrasound instrument and a 3S transducer (General Electric Healthcare, Wauwatosa, WI, USA).
An intravenous line was placed in the right antecubital vein and to which two 10 mL syringes were connected. One syringe was filled with 8 mL physiological saline solution and the other with 1 mL air. Subsequently, 1 mL blood was drawn into the air-filled syringe and mixed with the saline by reverse flushing between both syringes, creating agitated saline, which contains microbubbles [1, 13, 14].
All TTCEs were performed by echocardiographers trained in contrast echocardiography. The patient was positioned in the left lateral position and 5 mL agitated saline was injected within 3 s while projecting the four-chamber apical view. When possible the pulmonary veins were visualised. This procedure was repeated while the patient performed a Valsalva manoeuvre.
All shunts visualised through a pulmonary vein were classified as pulmonary RLS and all shunts through the septum as patent foramen ovale. When shunt origin was not visible, a delay of four cardiac cycles was used to distinguish between a pulmonary and a cardiac shunt. The TTCE was considered positive for a pulmonary RLS if microbubbles appeared in the left atrium after four or more cardiac cycles [1, 8, 11, 13]. The RLS grade was based on the maximum number of microbubbles counted in the left side of the heart in one still frame. The RLS was graded as 1 (1–29 microbubbles), 2 (30–100 microbubbles) or 3 (>100 microbubbles), as described previously [11, 12, 15].
Shunt interpretation was performed by two independent cardiologists with expertise in HHT who were blinded to the individual patient characteristics. In case of disagreement on the presence, origin or grade of the RLS, the TTCE was reviewed again by both cardiologists together until final agreement was reached. When the quality of the TTCE was too poor for shunt interpretation, the patient was excluded from further analysis.
PAVM diagnosis and embolisation
At follow-up, chest CT was advised in all patients with a pulmonary RLS grade ≥2 [1, 13] and was performed using a ≥16-detector CT scanner (Philips Medical Systems) with a dedicated high-resolution algorithm and maximum slice thickness of 1 mm.
All chest CT images were evaluated by an interventional radiologist and pulmonologist with expertise in HHT and were discussed in a multidisciplinary consensus meeting in which the radiologists and pulmonologists were unaware of the results of TTCE. All PAVMs with a feeding artery diameter of ≥3 mm were considered accessible for transcatheter embolotherapy. For PAVMs with a smaller diameter, feasibility for embolisation was based on the anatomy and location of the PAVM. Increase in PAVM was defined as increase of the PAVM feeding artery and/or presence of new PAVMs. When more than one PAVM was present, the feeding artery of the largest PAVM was measured.
Statistical analysis
Descriptive statistics were used to describe patient characteristics. Continuous variables were reported as mean±sd. Proportions were given by numbers and corresponding percentages. Cohen's κ coefficient was calculated to assess inter-observer and inter-injection (between two repeating contrast injections in one particular patient) agreements. Statistical analysis was performed using a statistical software package (SPSS, version 22; SPSS Inc., Chicago, IL, USA).
Results
Study population
Between September 2004 and June 2010 TTCE screening was performed in 351 HHT patients. 148 patients were excluded because of prior embolisation (n=80), death (n=9) or other reasons (n=59; e.g. follow-up in other hospitals or follow-up without TTCE). Between February 2010 and June 2015 follow-up using TTCE was performed in 203 patients. Three patients were excluded because the quality of the TTCE at follow-up was not sufficient for RLS gradation. Patient selection is summarised in figure 1.
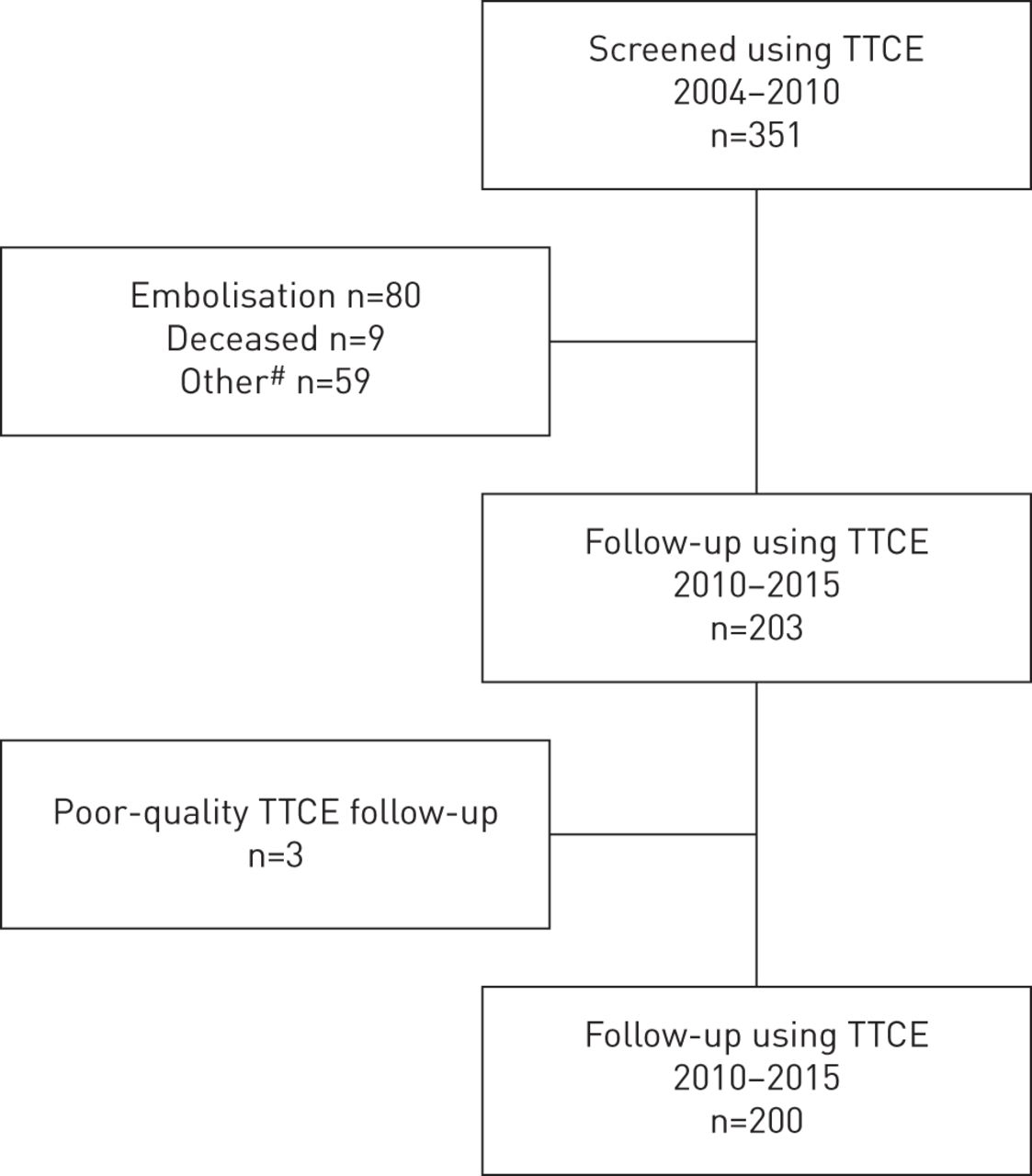
Patient selection. TTCE: transthoracic contrast echocardiogram. #: e.g. loss to follow-up or follow-up without TTCE.
200 patients (53.5% female, mean age at screening 44.7±14.1 years) were included for further analysis. HHT type 1, HHT type 2 and SMAD4 were found in 66 (33.0%), 130 (65.0%) and two (1.0%) patients, respectively. In two (1.0%) patients the HHT type was unknown. The mean follow-up time was 5.6±0.9 years. In 37 patients macroscopic PAVMs were visualised on chest CT, of whom none were embolised (too small n=36, declined embolisation n=1). Patient characteristics are summarised in table 1, characteristics of PAVMs at screening are described in table 2 and figure 2.

Diameter of feeding artery at screening and follow-up. When more than one pulmonary arteriovenous malformation (PAVM) is present, the feeding artery of the largest PAVM is described.
Baseline characteristics
Presence of one or more pulmonary arteriovenous malformations (PAVMs) on chest computed tomography at screening
Pulmonary RLS on TTCE
A pulmonary RLS was present in 113 (56.5%) patients at screening and 130 (65.0%) patients at follow-up (figure 3).

Pulmonary right-to-left shunt (RLS) at a) screening and b) follow-up.
A change in RLS grade was seen in 51 (25.5%) patients. In 36 (18.0%) patients (55.6% HHT type 2) an increase in RLS grade was seen; in 10 (27.8%) of these patients there was an increase from pulmonary RLS grade 1 to grade 2. The change in RLS between screening and follow-up was never more than one grade. The other results are summarised in figure 4.

Change in pulmonary right-to-left shunt (RLS).
In 30 consecutive patients inter-injection agreement (κ coefficient 0.95) and inter-observer agreement (κ coefficient 0.92) were calculated.
PAVMs and embolisation
At follow-up, chest CT was performed in 52 out of 55 patients with a pulmonary RLS grade ≥2. Three patients declined chest CT. In 37 (71.2%) out of these 52 patients a PAVM was seen on chest CT and embolisation could be performed in 14 (26.9%) of them. In the subgroup of patients without pulmonary RLS at screening (n=87), no treatable PAVMs developed during follow-up. In the subgroup of patients with nontreatable pulmonary RLS at screening (n=113), 14 (12.4%) underwent embolisation during follow-up.
In the total cohort, increase of feeding artery diameter and/or new PAVMs was present in 21 (10.5%) patients (figure 2 and table 3). The flowchart for embolisation is described in figure 5.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Flowchart of pulmonary right-to-left shunt (RLS) and embolisation. TTCE: transthoracic contrast echocardiography. Data are presented as n (% total cohort; % subgroup).
Changes in pulmonary arteriovenous malformations (PAVMs) on chest computed tomography (CT)
Complications
Between initial screening and follow-up an ischaemic stroke was documented in one patient. This patient had no pulmonary RLS and had a history of atrial fibrillation. In another patient an old infarction was found incidentally on cerebral magnetic resonance imaging; this patient did have a pulmonary RLS grade 2 and macroscopic PAVMs which were treated with embolisation subsequently. TTCE caused no complications.
Discussion
This is the first study using TTCE for the long-term follow-up of pulmonary RLS in patients with HHT. An important finding of this study is that in patients with no pulmonary RLS at screening, no treatable PAVMs developed within 5 years. However, importantly, during follow-up, increase in pulmonary RLS grade occurred in a substantial number of patients (18%). This increase was present in patients with and without RLS at screening, although it increased never more than by one grade. In patients with nontreatable pulmonary RLS at screening, 12% underwent embolisation during follow-up. Therefore this study demonstrates that repeated screening with TTCE might be necessary in all HHT patients.
Growth of PAVMs has been described in a few studies. Mager et al. [9] described the long-term follow-up of 112 patients after embolisation; recanalisation occurred in 13% and growth of PAVMs in 11%. No new PAVMs developed during follow-up. Pollak et al. [10] described 155 patients with PAVMs who underwent embolisation, and found growth of small nonembolised PAVMs in 18%. However, since both studies included only patients treated with embolotherapy, follow-up was performed using chest CT instead of TTCE. Therefore these studies are not comparable to our current study.
In the current guideline for HHT [3], the recommendations for follow-up of PAVMs are scarce and based on small series or expert opinion. Patients with negative initial TTCE are advised to repeat screening every 5–10 years and more often after puberty or pregnancy. In patients with small untreated PAVMs or microscopic PAVMs (positive TTCE but negative chest CT), follow-up is using chest CT is advised every 1–5 years on a case-by-case basis [3].
The use of chest CT for the follow-up of HHT patients has a few limitations. First, chest CT remains negative in ∼55% and ∼8% of patients with a pulmonary RLS grade 2 and 3, respectively, on TTCE [13]. Therefore, follow-up with chest CT may result in many unrecognised moderate to large pulmonary RLS in patients that still have a risk of paradoxical cerebral complications [13]. Second, follow-up with chest CT causes radiation exposure in this (mainly) young population. In contrast, TTCE has an excellent sensitivity and negative predictive value for the presence of PAVMs and a very low incidence of minor and self-resolving side-effects [12, 16, 17]. Moreover, recently published findings of our centre demonstrated a good correlation between pulmonary RLS grade and the probability of detecting PAVMs on chest CT and the subsequent feasibility of transcatheter embolotherapy [1, 13]. Patients with a grade 1 RLS do not have PAVMs that are large enough for embolisation and these RLS are not associated with neurological complications [1, 13]. For follow-up of pulmonary RLS, the reproducibility of TTCE is of the uttermost importance. Although the high inter-observer variability has already been described in several studies (κ coefficient 0.85–0.94) [8, 12, 15], no previous reports describe the reproducibility of TTCE in one particular patient. In our experience, inter-injection agreement in a single patient is high (κ coefficient 0.95). Surprisingly, a decrease in pulmonary RLS grade was seen in 15 (7.5%) patients. Most patients showed only a mild decrease in number of microbubbles, which could be explained by a difference in the amount of contrast in the right ventricle, the quality of the TTCE or haemodynamic differences. However, as described earlier, the reproducibility of contrast injection seems excellent. Other explanations for this decrease in microbubbles could be fibrosis or thrombosis of small PAVMs.
In this study, all patients treated with embolisation after screening were excluded, since TTCE remains positive in 90% of these patients [18]. As a result, the majority of the patients in our study had no or a small RLS (73%) at screening. The result of this selection bias is the inability to extrapolate these present findings to patients with larger shunts.
Increase in pulmonary RLS can be due to both increase in (diffuse) microscopic PAVMs or growth of macroscopic PAVMs, which are visible on chest CT. However, the exact pathogenesis of growth of PAVMs is not completely understood. Theoretically, the high flow through PAVMs, due to the relatively low resistance compared to the capillary network, can result in growth of PAVMs. Furthermore, it is known that HHT has an age-dependent penetrance and that the prevalence of PAVMs depends on the genotype. Other factors such as female hormones (e.g. during pregnancy) have been shown to influence other characteristics of HHT such as epistaxis [3] and may thus be possibly related to the growth of PAVMs. In addition, an increase in cardiac output, due to hepatic arteriovenous malformations, pregnancy or anaemia, might theoretically cause growth of PAVMs. However, in this study, these factors seem to have had little influence on the difference in shunt grade, since pregnancy occurred in only one patient, HAVMs were present in two patients and no patients had severe anaemia (defined as haemoglobin ≤6.0 mmol·L−1) at time of follow-up. Therefore, future larger studies are necessary to find predictors for increase in pulmonary RLS size in order to develop a tailor-made approach for each individual HHT patient.
Interestingly, 12% of patients with nontreatable PAVMs at screening underwent embolisation during follow-up. This supports the concept of possible growth of PAVMs in HHT patients and provides justification for the recommendation to repeat screening in HHT patients with small or microscopic PAVMs. Moreover, in the subgroup of patients with no pulmonary RLS and a pulmonary RLS grade 1, increase was described in 25% and 17%, respectively. This implies that development of PAVMs can occur in all HHT patients. Therefore, repeated screening for PAVMs should be performed in every HHT patient. More research is necessary to determine the optimal time interval for different patient groups.
This study presents some limitations. First, not all TTCEs were performed using the same ultrasound machine, which could lead to difference in quality and interpretation of the RLS grade. However, a very good inter-observer agreement (κ coefficient 0.92) and inter-injection agreement (κ coefficient 0.95) was found. Second, this is a single-centre study in a hospital with high experience with both PAVMs and TTCE, therefore it is not known whether the results apply to patients screened in other hospitals. A prospective multicentre validation study will be of major importance to confirm our data. Third, information on other cardiac parameters (e.g. valvular heart disease, left ventricular function, right ventricular systolic pressure, heart rate and cardiac output) that might have influenced the pulmonary shunt grading is absent.
On the basis of the results of this study, we recommend follow-up of patients with a pulmonary RLS every 5 years using TTCE. In patients with no pulmonary RLS at screening a conservative management strategy with an interval of >5 years might be safe.
Conclusion
Within 5 years, no treatable PAVMs were found in HHT patients without pulmonary RLS at initial screening. Increase in pulmonary RLS grade occurred in 18%, both in patients with and without pulmonary RLS at screening, and increased never more than by one grade. In the subgroup of patients with nontreatable pulmonary RLS at initial screening, 12% underwent embolisation.
Acknowledgement
This study was communicated as an oral presentation at the 11th HHT International Scientific Conference, June 11–14, 2015, Captiva Island, FL, USA.
Footnotes
Editorial comment in Eur Respir J; 47: 1618–1621.
Conflict of interest: None declared.
- Received September 24, 2015.
- Accepted January 14, 2016.
- Copyright ©ERS 2016
References










