





Abstract
A resting mean pulmonary artery pressure (mPAP) of 21–24 mmHg is above the upper limit of normal but does not reach criteria for the diagnosis of pulmonary hypertension (PH). We sought to determine whether an mPAP of 21–24 mmHg is associated with an increased risk of developing an abnormal pulmonary vascular response during exercise.
Consecutive patients (n=290) with resting mPAP <25 mmHg who underwent invasive exercise haemodynamics were analysed. Risk factors for pulmonary vascular disease or left heart disease were present in 63.4% and 43.8% of subjects. An abnormal pulmonary vascular response (or exercise PH) was defined by mPAP >30 mmHg and total pulmonary vascular resistance >3 WU at maximal exercise.
Exercise PH occurred in 74 (86.0%) out of 86 versus 96 (47.1%) out of 204 in the mPAP of 21–24 mmHg and mPAP <21 mmHg groups, respectively (OR 6.9, 95% CI: 3.6–13.6; p<0.0001). Patients with mPAP of 21–24 mmHg had lower 6-min walk distance (p=0.002) and higher New York Heart Association functional class status (p=0.03). Decreasing levels of mPAP were associated with a lower prevalence of exercise PH, which occurred in 60.3%, 38.7% and 7.7% of patients with mPAP of 17–20, 13–16 and <13 mmHg, respectively.
In an at-risk population, a resting mPAP between 21–24 mmHg is closely associated with exercise PH together with worse functional capacity.
Abstract
Resting mean PAP between 21–24 mmHg predicts abnormal exercise pulmonary haemodynamics and impaired functional capacity http://ow.ly/YfSuG
Introduction
Normal mean pulmonary artery pressure (mPAP) is 14±3 mmHg with an upper limit of 20 mmHg [1]. At present, the haemodynamic definition of pulmonary hypertension (PH) is an mPAP ≥25 mmHg at rest when measured invasively by right heart catheterisation (RHC) [2, 3]. Thus, patients who present with a resting mPAP between 21–24 mmHg do not fulfil a diagnosis of PH but fall outside the limits of normality. The recent 5th World Symposium on PH [2] and the current 2015 European Society of Cardiology/European Respiratory Society Guidelines for the diagnosis and treatment of PH [4] have both recommended that further research is required to phenotype this group of patients with resting mPAP between 21–24 mmHg.
Although it is recognised that an abnormal pulmonary haemodynamic response during exercise can develop in patients with pulmonary vascular disease (PVD) or left heart disease (LHD), the previous definition of exercise PH (mPAP >30 mmHg) was abandoned in 2008 [5]. In part, this was related to uncertainty regarding the normal limits of exercise mPAP and that healthy individuals can apparently exceed the mPAP threshold of 30 mmHg at high cardiac output (CO) [6, 7]. Recently, there is accumulating evidence to support that an abnormal pulmonary vascular response during exercise or exercise PH may be defined by a mPAP >30 mmHg and total pulmonary vascular resistance (TPVR) >3 WU at maximal exercise [6, 8, 9]. The combined use of mPAP and TPVR was demonstrated to significantly reduce the number of false positive cases compared to the old exercise PH criterion [8].
Limited studies have characterised the relationship between resting and exercise haemodynamics using gold standard invasive measurements in patients at risk for PH [10–18]. Previous studies have suggested that resting and exercise haemodynamics might be correlated [10, 11] but these studies have universally defined exercise PH using the now abandoned haemodynamic criteria, rendering the interpretation of such data difficult. Recently, Kovacs et al. [14] showed that patients with resting mPAP between 21–24 mmHg have higher mPAP–CO slopes during exercise and reduced exercise capacity compared with those with strictly normal mPAP.
In the present study, we sought to characterise the invasive exercise haemodynamic response of consecutive patients with resting mPAP <25 mmHg who have presented to our institution for evaluation of suspected PH or unexplained effort intolerance. Specifically, our aim was to evaluate whether an abnormal exercise response of the pulmonary circulation is more prevalent in patients with resting mPAP between 21–24 mmHg (mPAP21–24) compared with those with resting mPAP ≤20 mmHg (mPAPnormal).
Methods
We reviewed the haemodynamic database of the Centre National de Référence de l'Hypertension Pulmonaire Sévère, Le Kremlin Bicetre, France (formerly at Clamart, France) for exercise RHC performed between January 2005 and September 2014. Consecutive patients referred for suspected PH or investigation of undifferentiated dyspnoea who underwent invasive exercise testing were included if resting mPAP was <25 mmHg and PAWP ≤15 mmHg. A subset of patients with resting mPAP ≤20 mmHg) has previously been reported in a separate study [8]. At our institution, it is usual practice to perform exercise haemodynamic whenever feasible for patients who are discovered to have a resting mPAP <25 mmHg. The study was approved by the local ethics review committee (approval no. 9708, Hôpital Bicêtre, Université Paris-Sud) and all patients provided informed consent for RHC.
Pulmonary haemodynamics were acquired with a balloon-tipped, double-lumen, fluid-filled 7 Fr Swan Ganz catheter (Corodyn TD; Braun Medical, Bethlehem, PA, USA) via either the jugular or brachial vein approach. Zero reference was set at the midchest level [19]. Dynamic exercise was performed with an electronically braked lower limb cycle ergometer (Cyline 100; HEF Medical Developpement, Andrezieux-Boutheon, France) with subjects in supine position. mPAP, pulmonary artery wedge pressure (PAWP), and cardiac output (CO) were obtained at baseline and at the following stages every 3–5 mins: legs on cycle pedal, unloaded pedalling (0W) and at constant workload increments of 10–30W depending on estimated exercise capacity of subjects, as described previously [20]. Measurements were taken after stabilisation of mPAP and HR at each exercise stage. mPAP were averaged over the respiratory cycle [21] and cardiac output was recorded by thermodilution. Subjects were encouraged to cycle until exhaustion or appearance of exercise-limiting symptoms (severe dyspnoea, chest pain, leg pain or dizziness). Transpulmonary gradient (TPG) was calculated as mPAP−PAWP, total pulmonary vascular resistance (TPVR) as mPAP/CO, pulmonary vascular resistance (PVR) as (mPAP−PAWP)/CO, mPAP–CO slope as (peak mPAP−rest mPAP)/(peak CO−rest CO) and total power delivered to the pulmonary circulation by the right ventricle as 1.25×mPAP×CO [22].
Risk factors for PVD were recorded and they included connective tissue diseases, history of thromboembolic disease, history of anorexigen intake, familial history of pulmonary arterial hypertension (PAH), liver disease, HIV infection, congenital heart disease and sickle cell disease. We defined the presence of a risk factor for LHD as having one or more of age >65 years, body mass index (BMI) >30 kg·m−2, systemic hypertension, diabetes, ischaemic heart disease or atrial fibrillation.
An abnormal pulmonary vascular response during exercise or exercise PH was defined by mPAP >30 mmHg and TPVR >3 WU at maximal exercise, as previously described [8]. Exercise PH was divided into 1) a precapillary pattern when mean PAWP at peak exercise was ≤20 mmHg; and 2) a postcapillary pattern when mean PAWP at peak exercise was >20 mmHg [8, 15].
For our primary analysis, patients were stratified according to resting mPAP values of ≤20 mmHg and 21–24 mmHg. To further analyse the relationship between resting and exercise haemodynamics, we also considered resting mPAP over regular decreasing mPAP intervals of 21–24, 17–20, 13–16 and <13 mmHg in order to test the pathophysiological hypothesis that higher resting mPAP within the normal range are associated with the occurrence of exercise PH.
Statistical methods
All data are presented as mean and standard deviation, unless otherwise stated. Group comparisons were made using t-tests, Mann-Whitney U-test, Fisher's exact test or Chi-squared test as appropriate. One-way ANOVA or the Kruskal–Wallis test were used when comparisons were performed for three or more groups. Within-group comparisons of resting and exercise parameters were conducted with paired t-test. Multivariate logistic regression analysis and receiver–operating characteristic analysis were used to identify baseline clinical characteristics associated with the development of exercise PH. A p-value of <0.05 was considered significant. Statistical analyses were performed with SPSS Version 22 (IBM, Chicago, IL, USA).
Results
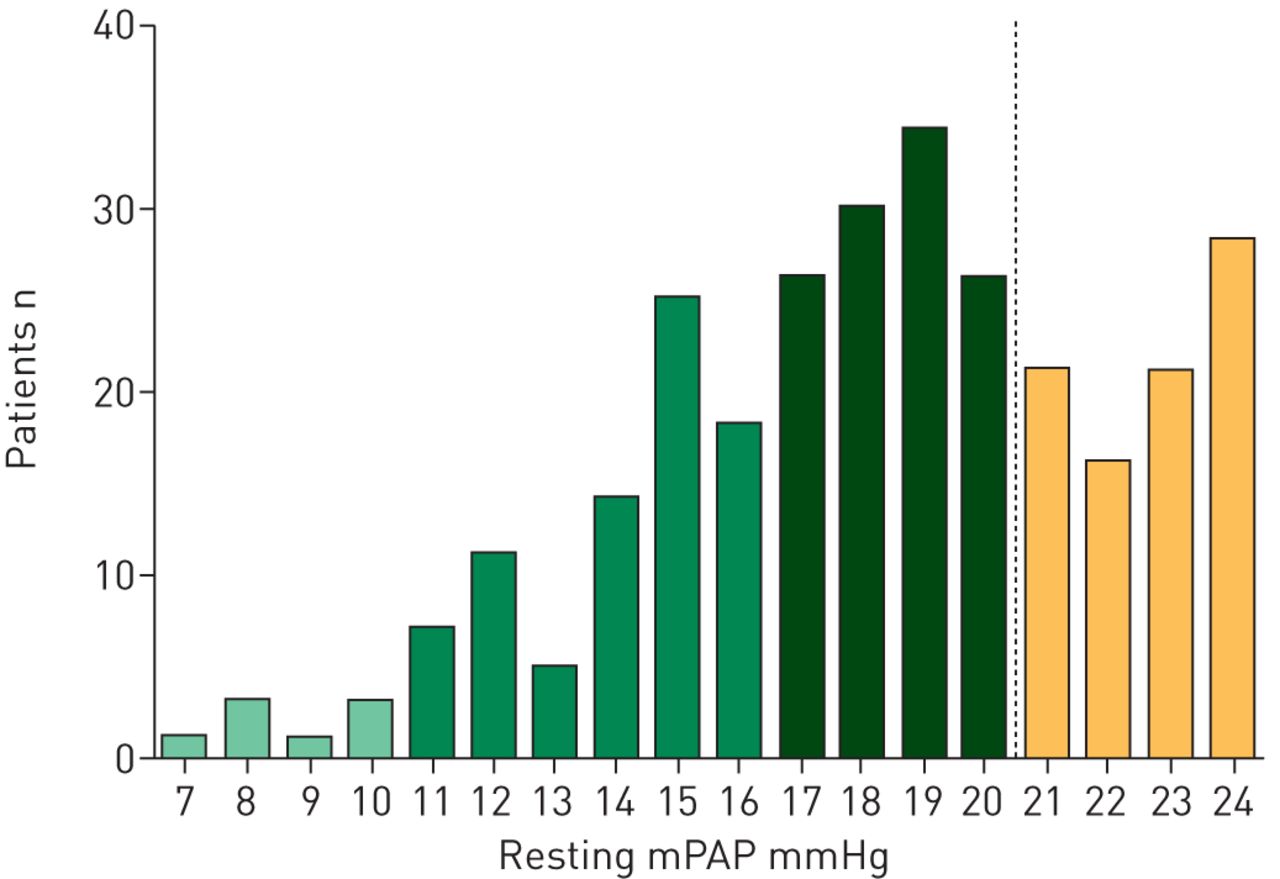
The entire study population consisted of 290 patients with resting mPAP <25 mmHg and PAWP ≤15 mmHg, of whom 86 (29.7%) patients had a resting mPAP between 21–24 mmHg. The distribution of resting mPAP values is shown in figure 1.

Distribution of resting mean pulmonary artery pressure (mPAP) in study population. The dotted line indicates the boundary between mPAP <21 mmHg and 21–24 mmHg.
The mean age of the total study population was 53±15 years with a female:male ratio of 2:1. The majority of patients had at least one risk factor for PVD (63.4%), with connective tissue disease (17.9%) and history of thromboembolic disease (17.6%) being the most common risk factors. The presence of a risk factor for LHD was documented in 43.8% of patients, with 23.4% above the age of 65 years, 15.9% with a BMI above 30 kg·m−2, and 19.3% with systemic hypertension. Baseline characteristics of study subjects are summarised in table 1.
Baseline demographics of study population
Clinical characteristics and resting haemodynamics: mPAPnormal versus mPAP21–24
No significant differences in age, sex ratio, BMI or risk factor profiles were seen between the mPAPnormal and mPAP21–24 groups. The mPAP21–24 group displayed significantly higher resting PAWP, TPG, PVR and TPVR, whilst resting CO was similar between the two groups. Functional capacity was significantly more impaired in the mPAP21–24 group as evidenced by lower 6-min walk distance (423±110 versus 471±109 m; p=0.002) and more advanced New York Heart Association (NYHA) functional class (p=0.03) (table 2).
Clinical characteristics and haemodynamic findings
Exercise haemodynamics: mPAPnormal versus mPAP21–24
Exercise induced significant increases in mPAP, PAWP, TPG, and CO in both the mPAPnormal and mPAP21–24 groups (all p<0.001). In contrast, exercise induced TPVR increases in both groups (both p<0.05) whereas PVR remained unchanged (table 2). However, individual responses of TPVR and PVR during exercise were heterogeneous.
The mPAP21–24 group achieved lower peak workload compared to the mPAPnormal group during supine cycle ergometry (p=0.002). Peak exercise mPAP, TPG, PVR and TPVR were all significantly higher in the mPAP21–24 group whereas peak CO was significantly lower (table 2).
Increasing resting mPAP strata from <13, 13–16, 17–20 to 21–24 mmHg were associated with a stepwise increase in peak exercise mPAP, peak TPG, peak PVR and peak TVPR (all p<0.001) (figure 2a). Similarly, exercise mPAP–CO slopes increased from 2.3±1.9, 3.8±2.8, 4.1±2.3 to 5.0±3.1 WU, respectively, for resting mPAP <13, 13–16, 17–20 to 21–24 mmHg (p<0.001) (figure 2b).
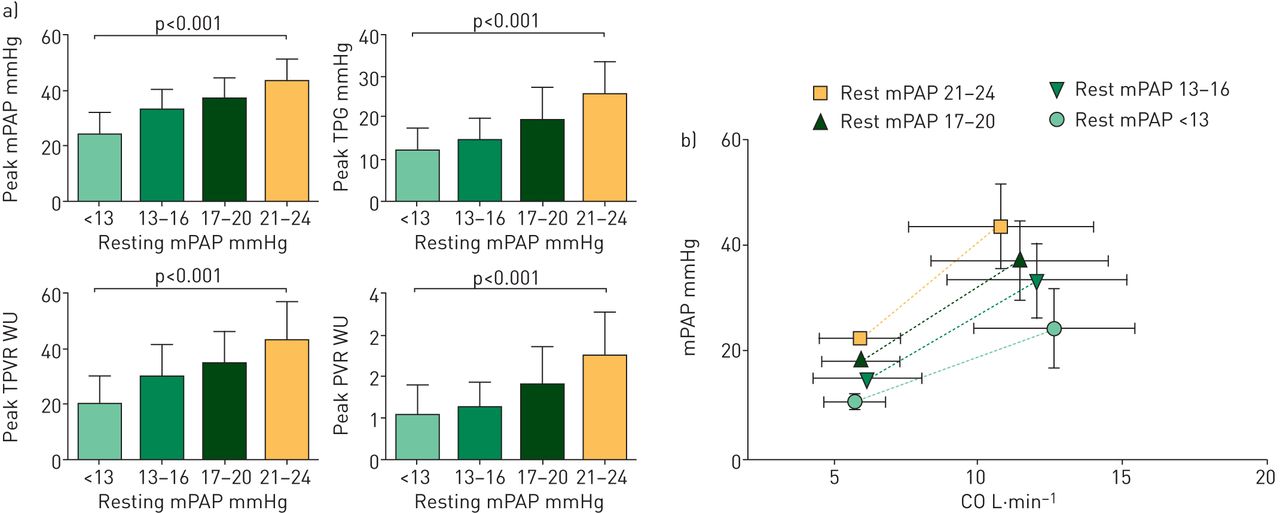
a) Relationships between resting mean pulmonary artery pressure and exercise haemodynamic parameters. Increasing resting mean pulmonary artery pressure strata was associated with higher values of peak exercise hemodynamic parameters. Patients with resting mean pulmonary artery pressure (mPAP) of 21–24 mmHg displayed the highest values of exercise mean pulmonary artery pressure, transpulmonary gradient (TPG), pulmonary vascular resistance (PVR) and total pulmonary vascular resistance (TPVR). b) Relationship between resting mPAP and mPAP–cardiac output (CO) slopes during exercise. Patients with mPAP between 21–24 mmHg displayed the steepest exercise mPAP–CO slopes. mPAP–CO slopes were 2.3±1.9, 3.8±2.8, 4.1±2.3 and 5.0±3.1 WU for resting mPAP values of <13, 13–16, 17–20 and 21–24 mmHg, respectively (p<0.001).
Exercise PH: mPAPnormal versus mPAP21–24
Using the criteria of peak mPAP >30 mmHg and peak TPR >3 WU as indicative of an abnormal pulmonary exercise response, exercise PH was diagnosed in 74 (86.0%) out of 86 of the mPAP21–24 group versus 96 (47.1%) out of 204 of the mPAPnormal group (OR 6.9, 95% CI: 3.6–13.6; p<0.0001). Within the mPAPnormal group, increasing mPAP strata was also associated with increasing prevalence of exercise PH; such that exercise PH was present in 2 (7.7%) out of 26, 24 (38.7%) out of 62, and 70 (60.3%) out of 116 of patients with resting mPAP <13, 13–16, and 17–20 mmHg, respectively (figure 3). On multivariable analysis, higher resting mPAP remained an independent predictor of exercise PH following adjustment for age, sex, presence of risk factors, 6-min walk distance and other resting haemodynamic variables (supplementary table S1).

Resting mean pulmonary artery pressure (mPAP) and the occurrence of exercise pulmonary hypertension (PH). Exercise PH (defined by a peak mPAP >30 mmHg and peak total pulmonary vascular resistance >3 WU) was present in 7.7%, 38.7%, 60.3% and 86.0% of patients with resting mPAP <13, 13–16, 17–20, and 21–24 mmHg, respectively. Patients with exercise PH were further stratified according to precapillary or postcapillary type response.
A precapillary pattern was found in 48 (64.9%) out of 74 of patients with exercise PH in the mPAP21–24 group compared with 53 (55.2%) out of 96 in the mPAPnormal group (p=0.27). In the overall population, patients with a precapillary pattern of exercise PH were significantly younger (56±14 versus 61±14 years; p=0.011), had a lower BMI (24.1±4.5 versus 26.5±5.7 kg·m−2; p=0.003) and were less likely to have a risk factor LHD (21.8% versus 44.9; p=0.001) compared with those with a postcapillary exercise PH pattern. NYHA functional class or 6-min walk distance were not significantly different between those classified with precapillary and postcapillary exercise PH. The exercise haemodynamic response according to different underlying risk factors is provided in supplementary table S2
Predictors of exercise PH in the mPAP21–24
As the majority of patients in the mPAP21–24 group fulfilled criteria for exercise PH, we performed further analysis in order to define the haemodynamic characteristics of mPAP21–24 patients with and without co-existent exercise PH. Patients in the mPAP21–24 group without exercise PH had higher resting CO (7.9±1.6 versus 5.6±1.1 L·min−1; p<0.001), lower resting PVR (1.7±0.6 versus 2.7±0.8 WU; p<0.001), lower resting TPVR (2.9±0.5 versus 4.2±0.8 WU; p<0.001) but similar resting TPG and PAWP. Resting and exercise mPAP–CO relationships, according to the presence or absence of exercise PH in the mPAP21–24 group are summarised in figure 4. Receiver–operating characteristics analysis showed that both resting mPAP and TPG could not identify mPAP21–24 patients without co-existent exercise PH (both AUC <0.75). On the other hand, resting TPVR (AUC=0.94), resting PVR (AUC=0.84) and resting CO (AUC=0.92) provided predictive information (figure 5). A resting TPVR of >3.4 WU had sensitivity of 87% and specificity of 92% for presence of exercise PH in the mPAP21–24 group.

Mean pulmonary artery pressure (mPAP)–cardiac output (CO) relationships in mPAP 21–24 mmHg group according to presence of exercise pulmonary hypertension (PH). Compared with those without exercise PH (n=12), patients with exercise PH (n=74) had higher resting mPAP (22.8±1.2 versus 21.9±1.0 mmHg; p=0.02), lower resting CO (5.6±1.1 versus 7.9±1.6 L·min−1; p<0.0001) and higher mPAP–CO slopes (5.6±3.0 versus 2.3±0.6 mmHg·L−1·min−1; p<0.0001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristics analysis for predicting exercise pulmonary hypertension (PH) in mean pulmonary artery pressure (mPAP) 21–24 mmHg group (mPAP21–24). Resting mPAP and transpulmonary gradient (TPG) provided poor identification of mPAP21–24 patients with co-existent exercise PH (both AUC <0.75). However, resting total pulmonary vascular resistance (TPVR) (AUC 0.94), resting pulmonary vascular resistance (PVR) (AUC 0.84) and resting cardiac output (CO) (AUC 0.92) provided improved predictive information.
Discussion
The present study analysed invasive pulmonary haemodynamic during exercise in 290 patients with resting mPAP <25 mmHg who had presented for investigation of suspected PH or unexplained dyspnoea. Increasing levels of resting mPAP independently predicted the development of exercise PH, reaching 86% in those with a resting mPAP between 21–24 mmHg. This association persisted even after adjustment for the presence of risk factors for PH. Importantly, patients with an mPAP between 21–24 mmHg displayed poorer functional capacity compared with those with strictly normal mPAP. The very high prevalence of abnormal exercise response together with increased functional limitation provide support that patients with a resting mPAP between 21–24 mmHg may represent a distinct phenotype with clinical relevance and should be viewed as a separate high-risk group between “normality” and overt PH.
Clinical significance of mPAP between 21–24 mmHg
A previous systematic review of all available invasive haemodynamic data published in the literature has shown that normal resting mPAP is 14±3 mmHg with an upper normal limit of 20 mmHg [1]. This value is independent of sex and ethnicity and relatively independent of age. Thus, there exists a “grey zone” in which patients with a mPAP between 21–24 mmHg cannot strictly be classified as normal but do not fulfil haemodynamic criteria for the diagnosis of resting PH (i.e. mPAP ≥25 mmHg). Our study, together with other accumulating data, suggests that patients with mPAP between 21–24 mmHg should be distinguished from those with strictly normal mPAP.
A number of studies have examined the clinical relevance of patients who present with mPAP between 21–24 mmHg. Heresi et al. [23] demonstrated that in patients who had undergone RHC for clinical indications, increasingly mPAP from normal, 21–24 mmHg to resting PH was associated with a progressively worse survival. In patients with systemic sclerosis, Valerio et al. [24] found that a baseline mPAP between 21–24 mmHg was associated with an increase risk developing resting PH on follow-up (HR 3.7, 95% CI 1.7–8.0), with 18.5% and 27.1% of patients developing resting PH by 3 and 5 years, respectively.
More recently, Kovacs et al. [14] examined 141 patients with resting mPAP <25 mmHg who underwent RHC for symptoms indicative of PH or due to underlying disease associated with an increased risk for PH. In this cohort, the mortality rates of patients with mPAP between 21–24 versus normal mPAP were 19% and 4%, respectively, at an average follow-up of 4.4±1.4 years. Patients with mPAP between 21–24 mmHg displayed higher mPAP-CO slopes during exercise and decreased exercise capacity. Furthermore, the mPAP21–24 group was older, had higher BMI and displayed an increased prevalence cardiorespiratory co-morbidities compared to those with normal mPAP. Our study demonstrated a very high prevalence of exercise PH in patients with mPAP 21–24 mmHg together with poorer functional class status and lower exercise capacity, and this corroborates the findings of Kovacs et al. [14] in a significantly larger cohort of patients. However, in contrast to Kovacs et al. [14], we did not observe any differences in terms of age, BMI or prevalence of comorbidities between the mPAP 21–24 mmHg and normal mPAP groups. The reasons for this are unclear and may reflect underlying differences in baseline demographic and risk factor profiles between the two study populations.
Relationship between mPAP21–24 and exercise PH
There is accumulating evidence to support that exercise PH is a clinically relevant haemodynamic syndrome associated with functional limitation and dyspnoea-fatigue symptoms [6, 7, 10, 11, 25–27]. Although no consensus definition currently exists for exercise PH, current evidence suggests that exercise PH may be better defined by using a combined criteria of mPAP >30 mmHg and TPVR >3 WU. These thresholds are based on exhaustive analysis of limits of normal in healthy individuals from available invasive and non-invasive data in the literature [6, 9]. Recently, these criteria have been demonstrated to provide high diagnostic accuracy for discriminating controls from patients with PVD or LHD with mPAP≤20 mmHg [8].
We found that resting mPAP was an independent predictor for the development of exercise PH, suggesting that resting and exercise hemodynamic are correlated. As exercise PH may represent an early or latent form of resting PH [7, 11, 28, 29], the high prevalence of exercise PH documented in the patients with mPAP between 21–24 mmHg provides further support that these patients may be at an increased risk of evolution to overt PH over time. Thus, careful clinical follow-up should be considered in this group, particularly if strong risk factors for PH are present such as systemic sclerosis or carriers of PAH-causing mutations. However, the optimal approach on how these patients should be followed up is currently unclear and under investigation.
Although our results indicate that exercise PH is unlikely in cases of low resting mPAP (<13 mmHg) or very likely in cases of resting mPAP between 21–24 mmHg, there appears to be no minimum resting mPAP threshold at which exercise PH will not occur. It must be stressed that our results strictly apply to a high-risk population, many of whom had strong risk factors for PVD and left ventricular diastolic dysfunction. Thus, our results do not imply that exercise PH is a relatively common occurrence in a general unselected population.
Interestingly, in the minority of patients with resting mPAP between 21–24 who did not have exercise PH, close inspection revealed that many displayed a relatively hyperdynamic circulation at rest (with high normal or elevated cardiac output), resulting in a disproportionately low resting TPVR. Accordingly, we found that in patients with mPAP between 21–24 mmHg, resting TPVR provided some predictive value for the presence of co-existent exercise PH. It would be of interest to clarify in further studies whether the natural history of patients with mPAP between 21–24 mmHg with concurrent exercise PH is different compared to those without exercise PH.
Our study suggests that resting and exercise haemodynamics are correlated but there remains significant scatter in the exercise haemodynamic response for subjects with similar levels of resting mPAP. One cannot predict with certainly based on resting haemodynamics alone whether exercise PH will be present. Thus, exercise haemodynamic testing remains invaluable in clinical practice to determine whether an abnormal pulmonary vascular response is contributing to exercise limitation and symptoms.
Limitations
Due to the retrospective nature of the present study, systematic longitudinal follow-up with clinical assessment and repeat invasive haemodynamic evaluation were not available. Since our cohort did not have resting PH, the majority of patients did not undergo routine follow-up at our centre. Therefore, our study cannot provide reliable outcome data regarding the natural history of patients with resting mPAP between 21–24 mmHg (or those with exercise PH) and their future risk of progression to overt resting PH. Further prospective longitudinal studies are required to address this important question, and whether underlying disease aetiology or other factors influence the risk of progression.
We used the criteria of exercise mPAP >30 mmHg and TPVR >3 WU as case definition for exercise PH, with the acknowledgement that current guidelines have not adopted this proposed definition [4]. This definition of exercise PH is based on normative data derived from published invasive and non-invasive data in healthy subjects [6, 9, 26], and a recent retrospective study which demonstrated that this definition provided high accuracy for discriminating controls without heart or lung disease from those with pulmonary vascular disease or left heart disease. The validity of this exercise PH definition has not been well studied in the elderly (>70 years), obese and subjects with lung diseases, and further prospective validation studies are required [8]. Nevertheless, we have chosen to employ this definition of exercise PH based on currently available data and its demonstrated superiority over the old definition, with the acknowledgement of its potential limitations.
Finally, our population was enriched with patients with risk factors for PH such as connective tissue disease and history of previous venous thromboembolism. Therefore, our results may not be generalisable to other clinic populations. Our study does provide data of a sizeable real-life cohort of patients who were referred for invasive haemodynamic evaluation and reveals important insights regarding the relationship between resting and exercise pulmonary haemodynamics.
Conclusions
Patients presenting with a resting mPAP between 21–24 mmHg have a very high prevalence of an abnormal pulmonary vascular response during exercise, together with reduced exercise capacity and functional status, compared to those with normal mPAP. This provides further evidence to support the concept that patients with mPAP between 21–24 mmHg may represent a clinically relevant group between “normality” and overt PH.
Footnotes
Editorial comment in: Eur Respir J 2016; 47: 1315–1317.
This article has supplementary material available from erj.ersjournals.com
Conflict of interest: Disclosures can be found alongside the online version of this article at erj.ersjournals.com
- Received October 11, 2015.
- Accepted January 18, 2016.
- Copyright ©ERS 2016
References










