





Abstract
Modafinil is used internationally to treat residual sleepiness despite continuous positive airway pressure in obstructive sleep apnoea (res-OSA). In 2011, the European Medicines Agency removed the indication based on an unfavourable risk–benefit profile in two trials for efficacy and all accumulated safety data. We performed a meta-analysis of all randomised controlled trials of modafinil (or armodafinil) in res-OSA to quantify efficacy and safety.
We systematically searched and assessed studies from major databases, conferences and trials registries to find randomised, placebo-controlled trials of modafinil/armodafinil for ≥2 weeks in adult res-OSA treating sleepiness.
We analysed 10 of the 232 articles identified that met inclusion criteria (1466 patients). Modafinil/armodafinil improved the Epworth Sleepiness Scale score (2.2 points, 95% CI 1.5–2.9) and the Maintenance of Wakefulness Test over placebo (3 min, 95% CI 2.1–3.8 min). Modafinil/armodafinil tripled adverse events and doubled adverse events leading to withdrawal but did not increase serious adverse events (hospitalisations or death).
Modafinil and armodafinil improve subjective and objective daytime sleepiness in res-OSA. We believe our analysis is a fairer analysis of the risk–benefit profile of this indication. Clinicians may want to use this data to balance the risks and benefits on a case-by-case basis with their patients.
Abstract
An EMA risk–benefit analysis of modafinil in OSA was negative. Does analysing extra trials change the conclusion? http://ow.ly/VYvO8
Introduction
In obstructive sleep apnoea, residual daytime sleepiness despite continuous positive airway pressure (CPAP) use (res-OSA) is commonly reported [1]. Modafinil is a wakefulness promoter approved for use in the USA, Canada, Australia and, until recently, Europe, for the treatment of excessive daytime sleepiness in narcolepsy, shift work sleep disorder (SWSD) and res-OSA. The R-isomer of modafinil, armodafinil, supposedly the active enantiomer, is also approved in the USA for these indications. However, in 2011, the European Medicines Agency (EMA) reviewed the use of modafinil, and removed the SWSD and res-OSA indications for the drug [2]. While the EMA safety review included all pre- and post-marketing safety data, including spontaneous reports, their efficacy data was based on only the two initial trials reported in three articles [3–5] submitted for the purpose of marketing approval for res-OSA. However, we are aware of the existence of a number of other trials addressing the efficacy of modafinil. We wondered whether the picture may have been different if we included all efficacy and safety data from just the placebo-controlled trials specifically within the indication. The only other medication class to treat this sort of problem is the amphetamines, which have well-known safety issues as well as tolerance problems [6].
For clinicians treating patients with res-OSA, a comprehensive analysis of all available randomised trial data for the indication would be useful. We aimed to systematically review and perform a meta-analysis of data from all randomised, placebo controlled trials using modafinil or armodafinil in adults to treat res-OSA in adult patients.
Methods
Search strategy
We searched three major databases (Scopus, PubMed and the Cochrane Register of Controlled Clinical Trials) for randomised placebo-controlled trials of modafinil or armodafinil being used to treat res-OSA in adults. (online supplementary material). We used no time or language limits. The last search was performed on October 24, 2014.
We also searched sleep conference abstracts from Australia (Sleep and Biological Rhythms, Australasian Sleep Association Conference abstracts), Europe (Journal of Sleep Research, European Sleep Research Society abstracts) and the USA (Sleep, Associated Professional Sleep Societies Conference abstracts) published after 2000. We searched the US, European, Japanese and Australian/New Zealand clinical trial registries. We also contacted Teva Cephalon (Frazer, PA, USA), the key trial sponsor, to confirm that they were not aware of any additional trials.
Study selection and data extraction
Studies were initially assessed via their abstracts, with subsequent reference to the full article where there was insufficient information to definitively rule in or rule out the study. The studies were reviewed and excluded (J.L. Chapman and A. Vakulin, with discrepancies adjudicated by N.S. Marshall) by the following criteria (in order) as per the PICOT (population/patient problem, intervention, comparison, outcome, time) format (www.prisma-statement.org). Included articles were required to present original research. P: included studies were in community-dwelling adults (≥18 years old) with CPAP-treated res-OSA (Epworth Sleepiness Scale (ESS) score ≥10 or clinically evident daytime sleepiness). I: active treatment was required to have been with modafinil/armodafinil at any dose for ≥2 weeks. C: included studies compared modafinil/armodafinil to matching placebo. O: included studies were required to report a recognised measurement of daytime sleepiness such as the ESS (a self-reported likelihood of falling asleep or dozing in eight common situations with a total score from 0 (not sleepy) to 24 (extremely sleepy)) [7], Maintenance of Wakefulness Test (MWT) (a measure of objective wakefulness or the ability to resist sleep, measured in minutes) [8], Multiple Sleep Latency Test (MSLT) (a measure of objective sleepiness measured in minutes) [9] or Functional Outcomes of Sleep Questionnaire (FOSQ) (self-reported sleep-related quality of life) [10]. T: included studies were required to be randomised clinical trials. A post hoc outcome measure was added during extraction as so many trials had reported it (Clinical Global Impression of Change (CGI-C) or Improvement (CGI-I) scale [11]). Eligible trials were then assessed for risk of bias using standard assessment criteria [12].
Study and patient characteristics were extracted (J.L. Chapman and A. Vakulin) and are presented in tables 1 and 2, respectively. Outcome variables were extracted by the same investigators into Revman (version 5.3) and reported in Forest plots. We (J.L. Chapman and N.S. Marshall) then extracted the number and type of serious adverse events (SAEs) (any untoward occurrence happening during the clinical trial, regardless of assumption of causality, resulting in inpatient hospitalisation, permanent disability or death), adverse events (AEs) requiring study withdrawal, number and proportion of participants who suffered any AE (any untoward occurrence happening during the clinical trial, regardless of assumption of causality), and the mean effects on blood pressure. When data could not be extracted from the published reports, online supplements or trial registries, authors were contacted by e-mail at least four times. When corresponding authors were unable to clarify ambiguous or missing data from their reports, the study author or sponsor (Teva Cephalon) was contacted. Publication bias was assessed using Funnel plots and Egger's test for asymmetry for outcomes measured in ≥10 studies. Where data were only available in a graphical form with no values, a plot digitiser was used to manually select the data points from the graph (PlotDigitizer 2.6.6; http://plotdigitizer.sourceforge.net/).
Characteristics of studies included in the meta-analysis
Patient characteristics
Data synthesis and statistical analysis
Continuous variables were analysed using the inverse variance method (RevMan) for a pooled mean effect and 95% confidence interval. Dichotomous variables (CGI-C, SAEs, AEs leading to withdrawal and number of patients suffering any AE) were analysed to obtain a pooled relative risk ratio and 95% confidence interval. Random effects models were used where at least moderate heterogeneity was observed (I2>40%) [12]. Where a study reported more than one dose of medication, we pooled the results from all active doses. Effect sizes for MWT and MSLT were calculated by dividing the mean size of the effect by the pooled standard deviation of each variable at baseline. As the patients were selected on ESS scores, it was inappropriate to use the pooled baseline standard deviation of this variable. Instead, a standard deviation of 4 was calculated from three reference populations [21–23]. The FOSQ effect size was calculated from a standard deviation sd from a reference population [24]. The events per patient year were calculated by dividing the number of events by the number of patient years across all studies.
Results
Systematic review
After duplicates were removed, 232 abstracts were identified (figure 1). The majority of abstracts was excluded as they did not contain original data; a few studies were excluded due to the patient population not meeting the criteria and one did not report a suitable outcome variable.
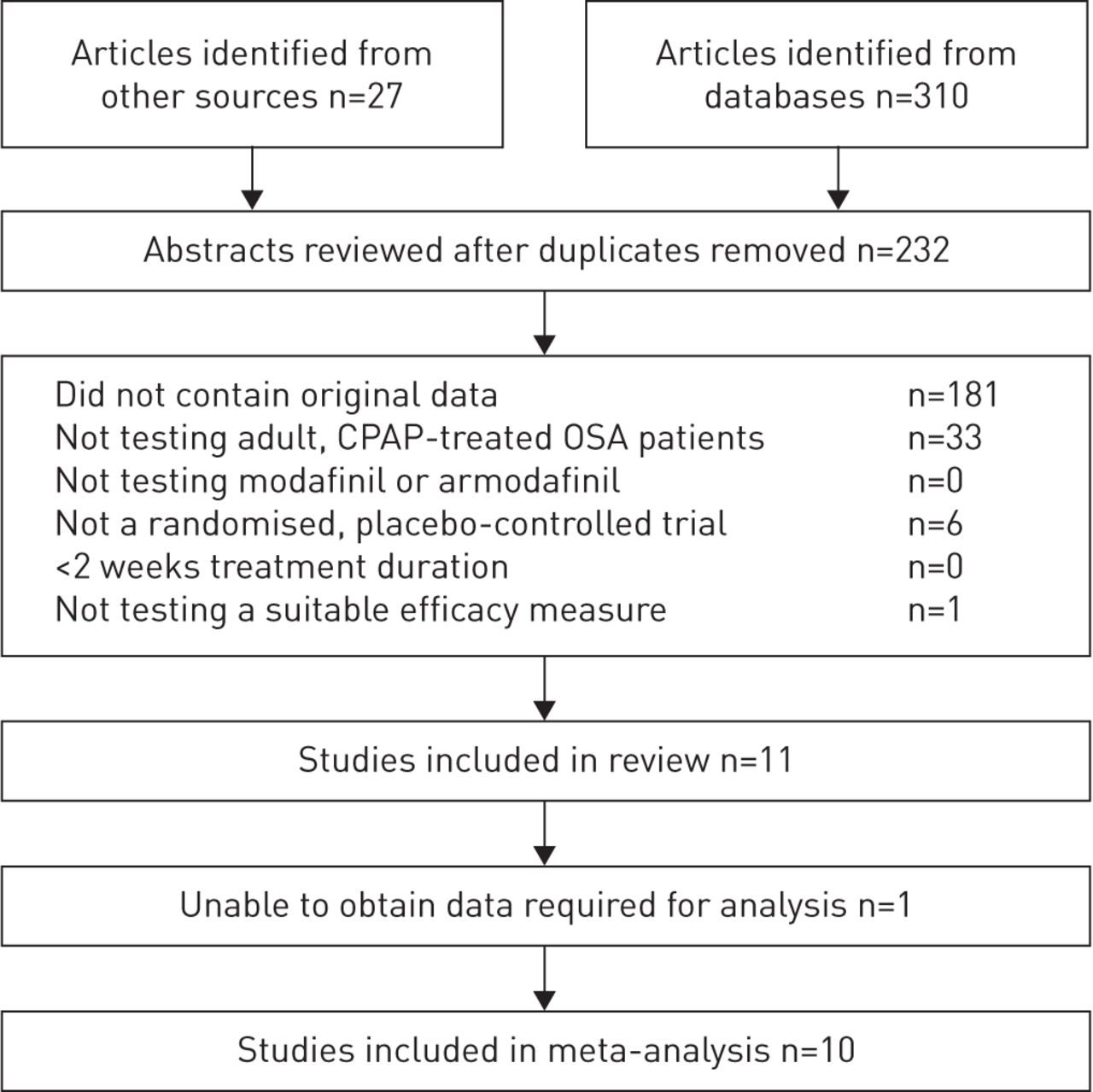
Flow chart of the systematic review. CPAP: continuous positive airway pressure; OSA: obstructive sleep apnoea.
Authors were contacted for seven studies where the required data was not able from published reports or clinical trial registries [3–5, 13, 14, 17, 18, 25]. Efficacy data were supplied by one study team [14]. The Teva Cephalon statistical team provided extra required data for four studies [3–5, 17, 18] but not one study [13] so data were extracted using the plot digitiser method. Schiza et al. [25] kindly responded to our request for clarification but the required data could not be obtained as the dataset had been lost.
Reviewers agreed that 10 studies reported in 11 articles met all criteria of the review and were able to be included in the meta-analysis [3–5, 13–20]. The characteristics of these studies can be seen in table 1. The characteristics of patients from included studies can be seen in table 2. The total number of patients analysed was 1466, and they were primarily middle aged, male and overweight–obese. While our study selection criteria did not explicitly state a required level of CPAP use, all patients had CPAP use of >4 h per night, except a subset of patients in one study [3].
No study reported was found to be at high risk of bias but some were methodologically unclear. No study was deemed to have inadequate patient and outcome assessor blinding, random sequence generation, allocation concealment, or completeness of reporting (table S1).
Meta-analyses
Meta-analysis indicated that modafinil/armodafinil reduced the ESS score by 2.2 points over placebo (95% CI 1.5–2.9; 10 trials) (figure 2). Random effects models were used as the results showed moderate heterogeneity (I2=58%). The effect size was moderate 0.55 (95% CI 0.38–0.73). A funnel plot of the mean effect versus effect size of each of these studies did not show strong evidence of publication bias (figure S2). The two studies included in the EMA review [3–5], when put together in a meta-analysis, show an improvement on ESS of 2.7 points over placebo (95% CI 1.9–3.5) (figure S1).

Forest plot indicating that Epworth Sleepiness Scale (ESS) scores improved significantly on modafinil/armodafinil by 2.2 points over placebo. Horizontal lines represent 95% confidence intervals from each indicated study for the effects of modafinil or armodafinil after adjustment for placebo. Elongated diamonds indicate the mean (apex of diamond) and 95% confidence intervals for the pooled estimate of the effect. The unit of measurement on the horizontal axis is improvement in points on a 24-point scale; patients like these typically start with a score above 10. df: degrees of freedom. #: armodafinil trial (all others modafinil).
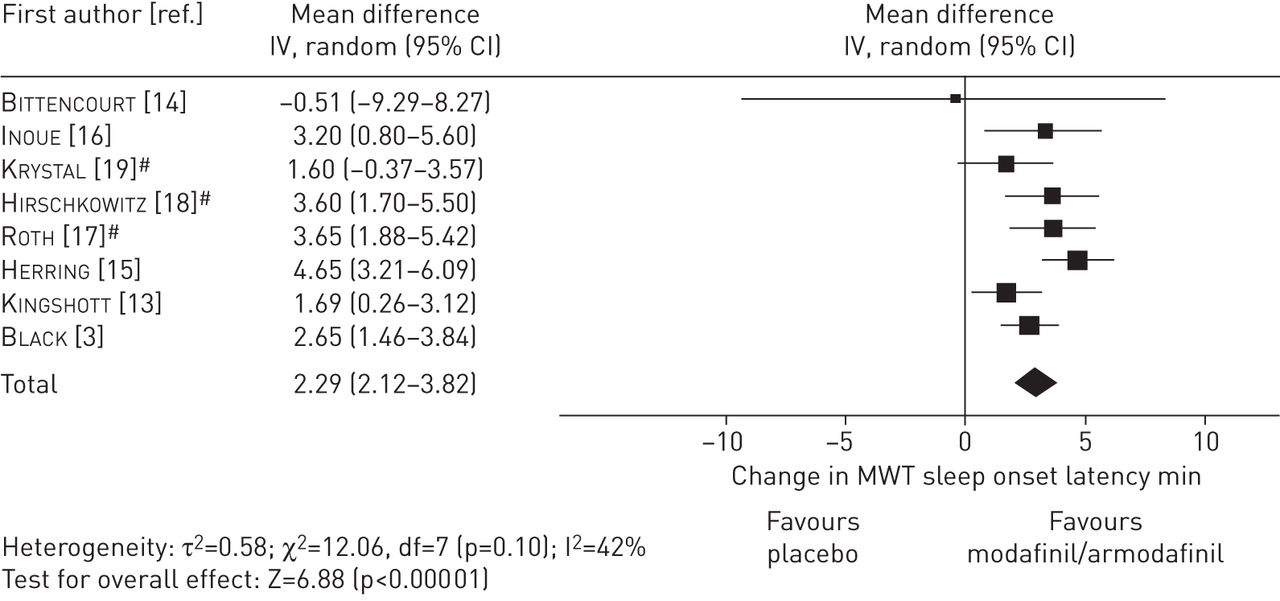
The MWT improved by 3 min on modafinil/armodafinil over placebo (95% CI 2.1–3.8 min, eight trials) (figure 3). Random effects models were used due to low–moderate heterogeneity (I2=42%). The effect size was small–moderate (0.41, 95% CI 0.36–0.51). MSLT was measured in two studies and showed an improvement in sleep onset latency on modafinil/armodafinil of 1.3 min over placebo (95% CI 0.3–2.3 min, I2 not calculable). The effect size was small (0.33, 95% CI 0.08–0.58) (figure S3).

Forest plot indicating that Maintenance of Wakefulness Test (MWT) sleep onset latencies were significantly improved by modafinil/armodafinil treatment by 3 min. Horizontal lines represent 95% confidence intervals from each indicated study for the effects of modafinil or armodafinil after adjustment for placebo. Elongated diamonds indicate the mean (apex of diamond) and 95% confidence intervals for the pooled estimate of the effect. df: degrees of freedom. #: armodafinil trial (all others modafinil).
FOSQ total score improved by 1 point over placebo (three studies; 95% CI 0.6–1.4; I2 not calculable). The effect size was small (0.33, 95% CI 0.2–0.46) (figure S4). Overall, 71% of patients on modafinil/armodafinil and 44% of patients on placebo were at least minimally improved on the CGI-C. This equates to a risk ratio (RR) for at least a minimally improved CGI-C score of 1.6 on modafinil/armodafinil compared with placebo (95% CI 1.3–2; seven trials) (figure S5). Random effects models were used again due to moderate heterogeneity (I2=45%).
Safety
There was a total of 1268 patient-years on modafinil/armodafinil and 1005 patient-years on placebo. There were no deaths reported on drug or placebo in any trial. Table S2 lists all SAEs, AEs leading to withdrawal and all reported AEs.
There was a total of 10 SAEs on modafinil/armodafinil (1036 patients) and nine SAEs reported on placebo (805 patients) (RR 0.8, 95% CI 0.2–3.1) (figure 4). In total, 75 (7.2%) of those on modafinil/armodafinil and 24 (3%) of those on placebo withdrew due to an AE (RR 2.1, 95% CI 1.3–3.4) (figure 5). Overall, there was a greater likelihood of a patient suffering any AE on modafinil/armodafinil than on placebo with (RR 1.7, 95% CI 1.3–2.2) (figure S6). There were 687 adverse events (0.54 per patient-year) reported on modafinil/armodafinil and 317 (0.32 per patient-year) on placebo. The common AEs (per patient-year) on modafinil/armodafinil were: headaches (0.14), nausea (0.05), anxiety (0.04), insomnia (0.04), dizziness (0.03), nervousness (0.02), diarrhoea (0.03), dry mouth (0.02), infection (0.02), runny nose (0.02) and upper respiratory tract infection (0.01). On placebo, the numbers of events per patient-year for these AEs were: headaches (0.07), nausea (0.02), anxiety (0.01), insomnia (0.01), dizziness (0.01), nervousness (<0.01), diarrhoea (0.02), dry mouth (no events), infection (0.02), runny nose (0.02) and upper respiratory tract infection (0.02).

Forest plot indicating that there is not an increased risk of suffering a serious adverse event on modafinil/armodafinil compared to placebo (risk ratio 0.8, 95% CI 0.2–3.1). Horizontal lines represent 95% confidence intervals from each indicated study for the effects of modafinil or armodafinil after adjustment for placebo. Elongated diamonds indicate the mean (apex of diamond) and 95% confidence intervals for the pooled estimate of the effect. df: degrees of freedom. #: armodafinil trial (all others modafinil).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot indicating that patients are more likely to report an adverse effect severe enough for them to withdraw from the trial on modafinil/armodafinil compared to placebo (risk ratio 2.1, 95% CI 1.3–3.4), indicating that there is an increased likelihood of suffering an adverse event leading to withdrawal on modafinil/armodafinil over placebo. Horizontal lines represent 95% confidence intervals from each indicated study for the effects of modafinil or armodafinil after adjustment for placebo. Elongated diamonds indicate the mean (apex of diamond) and 95% confidence intervals for the pooled estimate of the effect. df: degrees of freedom. #: armodafinil trial (all others modafinil).
The change in systolic and diastolic blood pressure on modafinil/armodafinil over placebo was numerically quantified in only three trials (figure S7). Systolic blood pressure increased by 3.0 mmHg (95% CI 0.8–5.2 mmHg) and diastolic blood pressure increased by 1.9 mmHg (95% CI 0.5–3.3 mmHg). The remaining seven trials all measured blood pressure and all reported no change.
Discussion
Our systematic review found 10 placebo-controlled trials of modafinil or armodafinil for the treatment of res-OSA. When analysed together, modafinil/armodafinil improved ESS score by 2.2 points over placebo (95% CI 1.5–2.9, effect size 0.55). Active treatment also improved MWT by 3 min (95% CI 2.1–3.8 min, effect size 0·41) and MSLT by 1.3 min (95% CI 0.3–2.3, effect size 0.33). Our other pre-specified measure of sleepiness was the patient-reported FOSQ, in which modafinil/armodafinil showed only a 1-point improvement over placebo (95% CI 0.6–1.4, effect size 0.33). Our post hoc outcome measure, CGI-C, was reported by seven trials and the likelihood of at least a minimally clinically significant improvement on modafinil/armodafinil was RR 1.6 greater than placebo (95% CI 1.3–2.0).
In 2010, the EMA removed the indication for modafinil to be used in res-OSA [2]. In the later 2011 publication detailing this decision [2], only two trials of modafinil [3–5] and none of armodafinil for the indication were assessed in determining efficacy, whereas much more extensive accumulated safety data were tabulated. The data were described but no meta-analysis was performed in this report. Our meta-analysis of just those two trials available to the EMA (reduction of 2.7 ESS points over placebo (95% CI 1.9–3.5) gave a very similar effect size to that we found analysing all 10 trials. They also had very similar effects on the MWT and MSLT.
A meta-analysis conducted in parallel with ours has recently reported a very similar efficacy estimate based on six of the 10 trials that we located [26]. So while our study is a more comprehensive review, the effect of modafinil/armodafinil is about the same as the effect identified by the EMA [2] and Sukhal et al. [26]
Safety
Patients on modafinil/armodafinil were not more likely to suffer SAEs than patients on placebo (figure 4). These trials were relatively short, and were powered to show effectiveness and not safety for rare events. Our estimate of risk for SAEs has wide confidence limits, meaning we cannot rule out the possibility of elevated risk. Risk of withdrawal due to adverse events and risk of all AEs was elevated on modafinil/armodafinil (figures 5 and S6). The adverse events that were notably elevated (table S2) were all already known and have been listed in the medication guides [27, 28].
Modafinil/armodafinil did not cause a clinically significant increase in blood pressure in these trials for res-OSA. The three trials that numerically quantified blood pressure changes, when analysed together, showed an increased systolic and diastolic blood pressure of 3.0 mmHg (95% CI 0.8–5.2 mmHg) and 1.9 mmHg (95% CI 0.5–3.3 mmHg), respectively (figure S7). Part of this apparent increase in the three trials reporting data may be due to a small decrease in blood pressure on placebo in the two larger trials [3–5]. The remaining seven trials measured and reported no changes in blood pressure, but unfortunately did not quantify this, so we were unable to perform a meta-analysis of these data (figure S7).
Our qualitative synthesis of these clinical trial data across all 10 trials are that modafinil/armodafinil might slightly increase blood pressure but this appears to be below the level of major clinical concern.
Limitations
The biggest limitation of our meta-analysis is the lack of long-term safety data. However, the safety data that we have analysed comes from placebo-controlled trials in properly selected patients, allowing us to make causative statements specific to this indication, at least over the short term (<3 months). The statistical analysis performed on safety data here is incomplete due to the different reporting styles of AEs (some trials reported all AEs, some only those events occurring in >3% or >5% of patients and one trial only reported adverse drug reactions, i.e. those with physician-assumed causality), not allowing an accurate meta-analysis of all events. Spontaneously reported data may be of some help in determining safety but those data are from open-label use and also suffer from a number of other well-described weaknesses. We have attempted to locate every trial ever undertaken on this question but it is possible we may have missed some. The sponsor of most of the initial trials was Cephalon (now Teva Cephalon), who have assured us they have not undertaken any other trials than we have described here. Our funnel plot analysis did not identify strong evidence of publication bias but it is possible that there are other investigator-initiated trials that are unregistered or have been registered outside of the databases we searched and remain unpublished in the peer-reviewed literature.
There was low–moderate heterogeneity between the studies, which we had not anticipated a priori. The source of heterogeneity appears to be the study by Inoue et al. [16], which reported the greatest net treatment effect and had a number of features that may be significant: fewer females, no dropouts and low body mass index in an ethnically Japanese population. Conversely, Krystal et al. [19] had a larger percentage of females (50%), higher dropouts and higher mean body mass index in their study with a lower effect size. This study was performed in depressed patients, which could also conceivably explain the reduced effect. Because this heterogeneity was unexpected and because of the relatively small number of trials, we have not presented formal statistical tests of heterogeneity as recommended [12].
Conclusion
This meta-analysis has shown that modafinil/armodafinil improves objective and subjective measures of daytime sleepiness in patients with res-OSA. In addition, our safety review has used the same high-quality data so clinicians can assess the risk–benefit profile with a clear idea as to causation within patients who actually fit the listed indication. The risk of long-term or serious risks within the indication remains unclear due to the underpowering of the trials available. Therefore, the removal of modafinil for this indication appears to have been an unfortunate decision by the EMA, particularly when the major pharmaceutical alternatives are amphetamine derivatives, which do not have a better safety profile and are well known potential drugs of abuse [6]. It seems to us that practising clinicians should consider modafinil in this indication on a case-by-case basis using their best clinical judgement but there is not a clear mandate for a blanket recommendation to not prescribe modafinil/armodafinil in these patients.
Acknowledgements
The authors would like to thank the following academic investigators who responded to our queries about ambiguous or missing data: Lia Bittencourt (Universidade Federal de Sao Paolo, Sao Paola, Brazil), Ruth Kingshott (Sheffield Children's NHS Foundation Trust, Sheffiled UK), David Dinges (University of Pennsylvania, Philadelphia, PA, USA), William Herring (Merck Sharpe and Dohme Corp., Rahway, NJ, USA) , Max Hirshkowitz (Baylor College of Medicine, Houston, TX, USA) and Sophia Schiza (University of Crete, Heraklion, Greece). We would also like to thank Teva Cephalon for their cooperation in providing results as required. Finally, we would like to thank Brendan Funnell (Funnell Designs, Sydney, Australia) for graphic design assistance.
Footnotes
This article has supplementary material available from erj.ersjournals.com
Support statement: This research was supported by an Australian National Health and Medical Research Council (NHMRC) grant to N.S. Marshall (1004528) and a University of Sydney Bridging Grant to N.S. Marshall. J.L. Chapman is supported by a NHMRC postgraduate scholarship (1038709). Funding information for this article has been deposited with FundRef.
Conflict of Interest: Disclosures can be found alongside the online version of this article at erj.ersjournals.com
- Received September 10, 2015.
- Accepted November 27, 2015.
- Copyright ©ERS 2016










