





Abstract
AIRWAYS-ICPs is a European Union initiative on multi-sectoral care pathways for chronic respiratory diseases http://ow.ly/Yndtw
Chronic respiratory diseases (CRDs) are major non-communicable diseases (NCDs) [1, 2] that induce a significant burden. Asthma often occurs along the life cycle from early childhood, affecting 30 million children and adults under 45 years of age in Europe [3]. Chronic obstructive pulmonary disease (COPD) has an estimated annual death rate of over 3 million people globally [1, 2]. The annual direct and indirect costs in the 28 European Union (EU) countries due to COPD or asthma are estimated at 48 billion euros and 34 billion euros respectively [3]. Rhinitis occurs in over 100 million people in Europe, and indirect costs are enormous [4]. Asthma is a common risk factor for COPD [5, 6]. CRDs impact ageing and should be prevented, recognised and managed across the life cycle to promote active and healthy ageing (AHA). There is an urgent need to act globally.
European Innovation Partnerships (EIPs) aim to enhance EU competitiveness and tackle societal challenges through research and innovation. To tackle the potential of ageing in the EU, the European Commission, within its Innovation Union policy, launched the EIP on AHA (between the Directorate General for Health and Food Safety (DG Santé) and Directorate General for Communications Networks, Content and Technology (DG CONNECT)) [7]. The B3 Action Plan promotes integrated care models for chronic diseases, including the use of remote monitoring.
The initiative AIRWAYS-ICPs (integrated care pathways for airway diseases) [8] has been approved by the EIP on AHA as the model of chronic diseases of the B3 Action Plan. It is a Research Demonstration Project of the World Health Organization's Global Alliance against Chronic Respiratory Diseases (GARD) [1]. AIRWAYS-ICPs was initiated in 2013 by the WHO Collaborating Centre of Montpellier and the EIP on AHA Reference Site MACVIA-LR (Contre les MAladies Chroniques Pour un VIeillissement Actif en Languedoc-Roussillon, France) led by the Région Languedoc-Roussillon (France) [9].
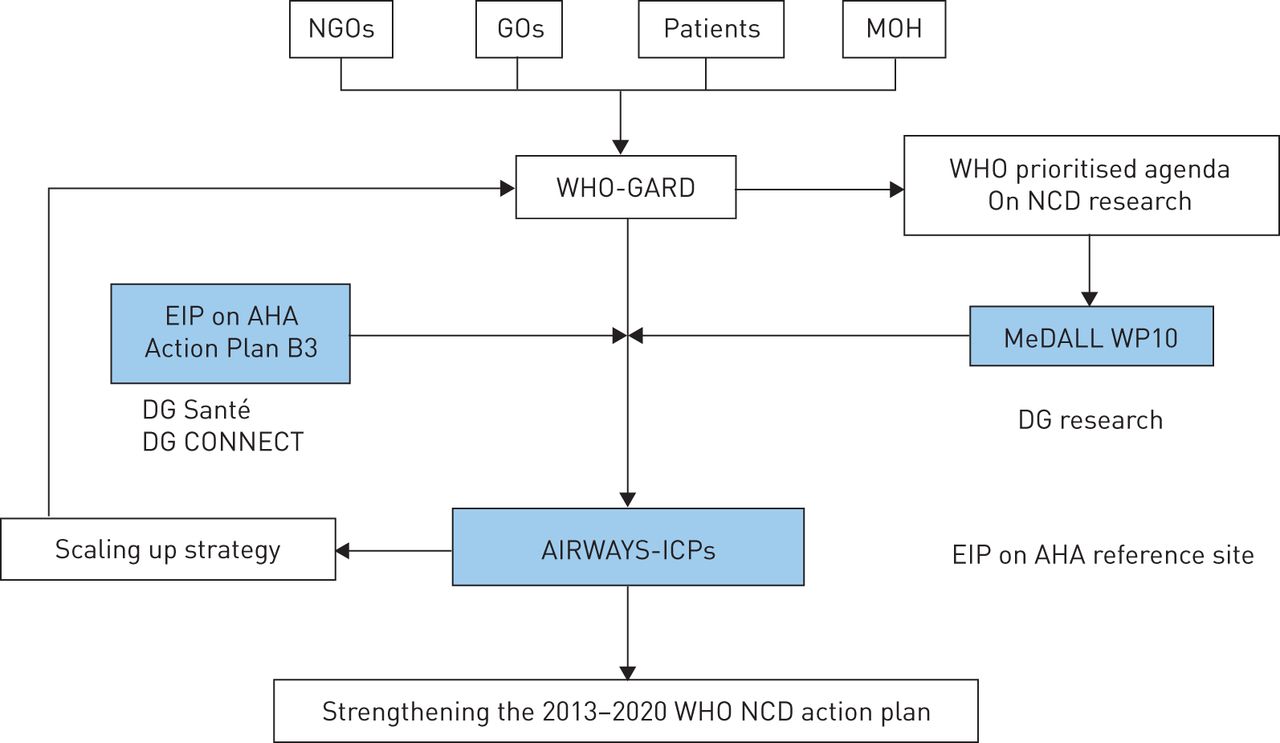
The GARD action plan was the model of AIRWAYS-ICPs (figure 1).

AIRWAYS-ICPs (integrated care pathways for airway diseases) interactions between the European Union and World Health Organization. NGO: nongovernmental organisation; GO: governmental organisation, MOH: Ministry of Health; GARD: Global Alliance against Chronic Respiratory Diseases; NCD: non-communicable disease; EIP: European Innovation Partnership; AHA: active and healthy ageing; DG Santé: Directorate General for Health and Food Safety; DG CONNECT: Directorate General for Communications Networks, Content and Technology; MeDALL WP10: Mechanisms of the Development of Allergy workpackage 10; DG Research: Directorate-General for Research and Innovation.
Objectives
The aim of AIRWAYS-ICPs is to launch a collaboration to develop practical multisectoral care pathways (ICPs) to reduce the burden of chronic respiratory diseases, their mortality and multimorbidity. AIRWAYS-ICPs proposes a feasible, achievable and manageable project from science to guidelines and policies using existing networks and stakeholders committed to the Action Plan B3 of the EIP on AHA and GARD [1, 2]. It is implemented in European countries and regions, as part of the EIP on AHA, and is scaled up globally with GARD.
Stakeholders
AIRWAYS-ICPs activities are being implemented by a group of 450 members in 70 countries. Members also include those of previous initiatives such as ARIA (Allergic Rhinitis and its Impact on Asthma; initiated in collaboration with WHO) [10] and GARD [1, 2]. The majority of members have been working together since 1999. The GA2LEN (Global Allergy and Asthma European Network, Sixth Framework Programme) network of excellence centres of allergy and asthma [11] and members of EIP on AHA commitments for action are also involved. All stakeholders needed for the implementation of an action plan at the national and local levels actively participate. Scientific societies also participate in the project.
Implementation of the AIRWAYS-ICPs action plan
The action plan was devised by a group of 450 members and implemented in 2013 [8]. Activities are proposed in a logical framework from existing tools to novel information communication technology (ICT) tools and innovative health systems in order to provide an integrated solution for CRDs across the life cycle. The model of CRD can then be used for the health promotion of AHA and management of CRDs in older adults.
Proposing a common framework of care pathways (ICPs) for CRDs to facilitate comparability and trans-national initiatives targeted to all populations according to culture, health systems and income [12]: AIRWAYS-ICPs is participating in the development of a repository that is currently being developed by the EU and that will be available in December 2015. This repository will include good practices in CRDs such as National Institute for Health and Care Excellence (NICE; UK) guidance, national programmes for CRDs [13], asthma, COPD or allergy [14–16], guidelines for asthma, COPD or allergic rhinitis [10, 17–20], and ICPs.
Developing a strategy for low-resource settings based on existing WHO initiatives such as the WHO Package of Essential Noncommunicable disease [21] and the essential list of drugs, as well as validated primary management strategies in low- and middle-income countries [22].
Aiding risk stratification in chronic disease patients with a common strategy. AIRWAYS-ICPs has developed a simple stratification algorithm for asthma control and severity (following a 2009 WHO meeting) which can be extended to all chronic diseases unifying the classification of the diseases for clinical, research and public health use [23–25].
Defining important questions on CRDs in older adults. There are no specific recommendations for CRDs in older adults and a research activity is ongoing to better understand asthma, COPD and their multimorbidities in old age.
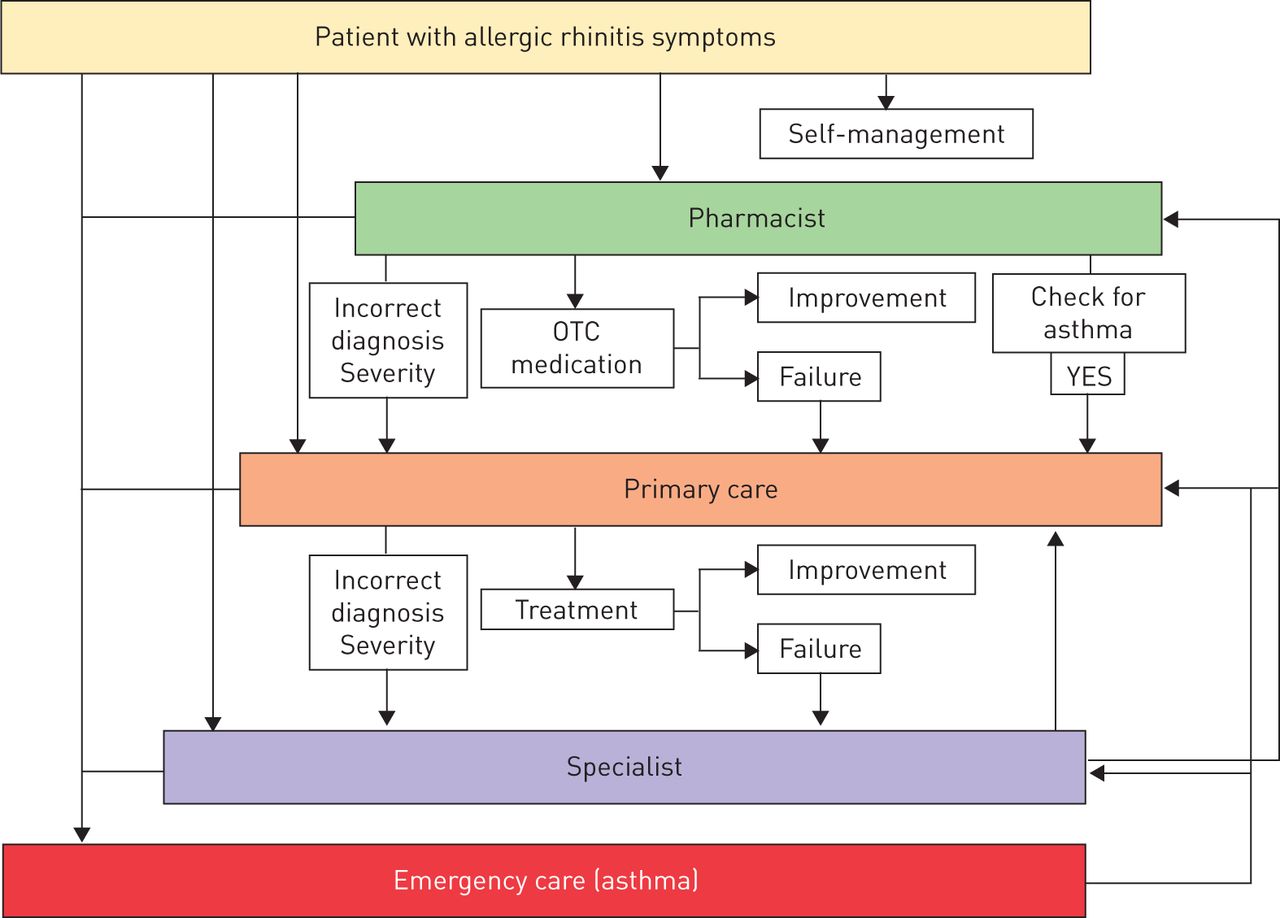
Developing multisectoral care pathways for CRDs and their multimorbidities across the life cycle, implementing emerging technologies for individualised and predictive medicine. Within the past four decades, an epidemic of allergic diseases and asthma has been observed globally in children and adults. The expected epidemic wave of asthma and rhinitis in older adults is an insufficiently recognised problem. In Europe, over 20% of adults suffer from allergic rhinitis and over 5% from asthma. These patients are now reaching the age of 65 years and a new health problem in old age people will be to understand, detect and manage these patients who also suffer from NCD multimorbididy and polymedication. There is an urgent need for a simple tool which would allow individualised and predictive medicine. AIRWAYS-ICPs is tackling this expected health problem, based on systems medical principles, in accordance with guidelines proposed by the European Commission (www.casym.eu) using the MACVIA-ARIA Sentinel NetworK (MASK). A common language is being used at the patient, pharmacist and physician levels using tablets and cell phones (figure 2).
A first project directly linked with the activities of the WHO Collaborating Centre on rhinitis and asthma was initiated in 2013 and has been completed [10, 26–30]. MASK proposes the study of symptoms of patients suffering from allergic symptoms during the pollen season (rhinitis and asthma) in order to make them sentinels for the onset and severity of the pollen season. Patients are geolocalised and evaluate their symptoms by visual analogue scale using a cell phone with a touch screen or internet. A clinical decision support system will be finalised in December 2015. A care pathway from the patient to health care professionals has been built (figure 2) and a clinical decision support system will be available in December 2015.
The system has been extended to persistent rhinitis and asthma, and a pulmonary function test using cell phones is currently being tested (available mid 2016). This may be of interest in all countries to screen for bronchial obstruction (asthma and COPD) by patients or at primary healthcare centres.
The application is available in 15 languages from the App store (iOS) and Google play (Android). It is free for patients and, due to the simplicity of the tool, it can be used in developed and many developing countries (if a smart phone is available).
Embedding the concept of frailty into CRDs and proposing an operational AHA questionnaire developed by the Reference Site Network of the EIP on AHA using WHO Disability Assessment Schedule 2.0 and quality-of-life questionnaires [31, 32]. Unrecognised CRDs can be detected in frail elderly patients [33]. Optimising treatment and integrated care services of frail COPD patients with multimorbidities and polypharmacy improves certain health outcomes [34].
Scaling up strategies in Europe and beyond. The scaling up strategy has been clearly defined and approved by AIRWAYS-ICPs members. It follows the EIP-AHA recommendations on a five-step framework: 1) what to scale up: 1-1) databases of good practices; 1-2) assessment of viability of the scaling up of good practices; 1-3) classification of good practices for local replication; and 2) how to scale up: 2-1) facilitating partnerships for scaling up; 2-2) implementation of key success factors and lessons learnt, including emerging technologies for individualised and predictive medicine. Scaling up will take place within and beyond Europe with GARD [35–40].
Strengthening the WHO NCD Action Plan. AIRWAYS-ICPs is in line with the WHO NCD Action Plan since it aims to reduce the preventable and avoidable burden of morbidity, mortality and disability by means of multisectoral collaboration and cooperation at national, regional and global levels.
{kind=link}
{kind=link}
Care pathways for rhinitis and asthma multimorbidity across the life cycle. OTC: over-the-counter. Reproduced from [26] with permission from the publisher.
Conclusions
AIRWAYS-ICPs is expected in the short term to reduce morbidity, and improve education and work and in the long term to promote AHA [41]. AIRWAYS-ICPs has strategic relevance to the EU Health Strategy and the WHO NCD Action Plan (2013–2020), adding value to existing public health knowledge.
Acknowledgements
AIRWAYS-ICPs working group: Adcock I, Addis A, Agache I, Agusti A, Alonso A, Annesi Maesano I, Anto JM, Bachert C, Baena-Cagnani C, Bai C, Baigenzhin A, Barnes PJ, Beck L, Bedbrook A, Benezet O, Bennoor KS, Benson M, Bernabeu-Wittel M, Bindslev Jensen C, Blain H, Blasi F, Bonini M, Bonini S, Boulet LP, Bourdin A, Bourret R, Bousquet PJ, Brightling CE, Briggs A, Brozek J, Buhl R, Bush A, Caimmi D, Calderon M, Calverley P, Camargos P, Camuzat T, Canonica GW, Carlsen KH, Casale TB, Cazzola M, Cepeda Sarabia AM, Cesario A, Chen YZ, Chkhartishvili E, Chiron R, Chuchalin A, Chung KF, Cox L, Crooks G, Crooks MG, Custovic A, Dahl R, Dahlen SE, De Blay F, Dedeu T, Deleanu D, Demoly P, Devillier P, Didier A, Dinh Xuan AT, Djukanovic R, Dokic D, Douagui H, Dubakiene R, Eglin S, Elliot F, Emuzyte R, Fabbri L, Fink-Wagner A, Fletcher M, Fokkens WJ, Fonseca J, Franco A, Frith P, Furber A, Gaga M, Gamkrelidze A, Garcia Aymerich J, González-Díaz S, Gouzi F, Garcés J, Guzmán MA, Harrison D, Hayot M, Heaney L, Heinrich J, Hooper J, Humbert M, Hyland M, Iaccarino G, Jakovenko D, Jardim J, Jeandel C, Jenkins C, Johnston SL, Jonquet O, Joos G, Jung KS, Kalayci O, Karunanithi S, Keil T, Kolek V, Kowalski M, Kull I, Kuna P, Kvedariene V, Le LT, Louis R, MacNee W, Mair A, Manning P, Manuel Keenoy ME, Majer I, Masjedi MR, Melén E, Melo Gomes E, Menzies-Gow A, Mercier G, Mercier J, Michel JP, Miculinic N, Mihaltan F, Milenkovic B, Molimard M, Momas I, Montilla-Santana A, Morais Almeida M, Morgan M, N'Diaye M, Nafti S, Nekam, Neou A, Nicod L, O'Hehir R, Ohta K, Paggiaro P, Palkonen S, Palmer S, Papadopoulos NG, Papi A, Passalacqua G, Pavord I, Pedersen S, Pigearias B, Plavec D, Postma DS, Price D, Rabe KF, Radier Pontal F, Redon J, Rennard S, Roberts J, Robine JM, Roca J, Roche N, Rodenas F, Roggeri A, Rolland C, Ryan D, Sanchez-Borges M, Schünemann HJ, Sheikh A, Shields M, Siafakas N, Sibille Y, Similowski T, Small I, Sola-Morales O, Sooronbaev T, Stelmach R, Sterk PJ, Stiris T, Sud P, Tellier V, To T, Todo Bom A, Triggiani M, Valenta R,Valero AL, Valovirta E, Vandenplas O, Van Ganse E, Vasankari T, Vestbo J, Vezzani G, Viegi G, Visier L, Vogelmeier C, Vontetsianos T, Wagstaff R, Wallaert B, Wahn U, Whalley B, Wickman M, Williams D, Wilson N, Yawn BP, Yiallouros P, Yusuf O, Zar HJ, Zhong N, Zidarn M.
Footnotes
Conflict of interest: Disclosures can be found alongside the online version of this article at erj.ersjournals.com
- Received November 9, 2015.
- Accepted November 9, 2015.
- Copyright ©ERS 2016
References










