





Abstract
Climate change policies have stimulated a shift towards renewable energy sources such as biomass. The economic crisis of 2008 has also increased the practice of household biomass burning as it is often cheaper than using oil, gas or electricity for heating. As a result, household biomass combustion is becoming an important source of air pollutants in the European Union.
This position paper discusses the contribution of biomass combustion to pollution levels in Europe, and the emerging evidence on the adverse health effects of biomass combustion products.
Epidemiological studies in the developed world have documented associations between indoor and outdoor exposure to biomass combustion products and a range of adverse health effects. A conservative estimate of the current contribution of biomass smoke to premature mortality in Europe amounts to at least 40 000 deaths per year.
We conclude that emissions from current biomass combustion products negatively affect respiratory and, possibly, cardiovascular health in Europe. Biomass combustion emissions, in contrast to emissions from most other sources of air pollution, are increasing. More needs to be done to further document the health effects of biomass combustion in Europe, and to reduce emissions of harmful biomass combustion products to protect public health.
Abstract
Biomass combustion is an important source of air pollution and ill health in the EU: emissions need to reduce http://ow.ly/RYkPk
Introduction
During the first half of the twentieth century, air pollution in many European cities was dominated by local emissions from fossil fuel combustion for space heating, energy production and manufacturing. As a consequence pollution episodes were common and often severe, like the smog episodes in London [1] and the Meuse valley [2] in Belgium, both associated with large and sudden increases in mortality. These and other episodes led the governments of different countries to introduce air pollution regulations, e.g. the Clean Air Act introduced in 1956 in the UK. Due to this change in practice and the increased availability of cleaner fuels such as oil and gas during the 1960s, air quality in many European cities improved markedly. Nevertheless, more recent studies have demonstrated continued adverse health effects of air pollution at much lower levels of exposure [3–5]. Recently it has also been shown that further decreases in air pollution had a beneficial effect on the life expectancy of the American population during the past few decades [6]. The World Health Organization (WHO), in its 2005 global update of the Air Quality Guidelines, set a guideline for fine particulate matter (PM) in air of just 10 µg·m−3 as an annual average. This concentration is still exceeded in large parts of Europe, and continued efforts are needed to reduce fine particles from all sources.
Against this background, it is potentially worrying that, as a response to climate change policies and fuel pricing, biomass burning (primarily of wood) for residential space heating as well as energy production is now an increasing source of fine PM emissions in the European Union (EU), thus posing new challenges to human health. As a response to fuel poverty, in some communities, wood/biomass burning is seen as a cheap form of fuel when gathered locally. For example, a recent study in Greece documented a 30% increase in winter PM, a 2.5-fold increase in biomass combustion markers and a 20–30% decrease in fuel oil tracers coinciding with the recent economic crisis [7].
A relatively small number of studies have evaluated the health effects of outdoor and indoor exposure to combustion products from fireplaces or wood stoves in developed countries [8–10]. However, extensive epidemiological literature exists that describes the adverse health effects of high-level exposure to pollution from household biomass combustion for cooking and heating purposes in developing countries [11–13]. This literature indicates causal links between PM and acute lower respiratory infections in young children, chronic obstructive pulmonary disease (COPD) in adults [14], and development of cataracts in women [15]. Lung cancer has also been linked to inhalation of biomass combustion products. Indoor emissions from biomass combustion and cooking in developing countries have been classified as probably carcinogenic (International Agency for Research on Cancer IARC Group 2A) [16].
Although combustion of biomass is known to produce numerous air pollutants, the focus of this report is PM emissions, which have received most of the attention in the scientific literature. Therefore, only epidemiological studies in which the primary measure for evaluation of biomass exposure is PM, or components thereof, are considered. This is consistent with the approach taken in prior reviews of biomass combustion health impacts [17, 18] and the Global Burden of Disease (GBD) 2010 report [19, 20]. This approach also follows the perspective of the WHO Air Quality guidelines [21], the review by Naeher et al. [17] and the recent WHO REVIHAAP project report [22], which concluded that there was a lack of evidence supporting differential toxicity of PM from biomass combustion when compared with urban PM from fossil fuel combustion and secondary atmospheric particles.
This position paper deals with the effects of biomass smoke on respiratory and cardiovascular health in the developed world, where wood burning is primarily, but increasingly, used as an auxiliary source of domestic heating and energy production. When searching the literature, the following terms were used in a PubMed search: “wood smoke” OR “domestic heating” AND “USA OR Canada OR Europe OR Australia” AND “wood stove” AND “health”. In addition to the search we consulted international experts and research centres active in the field.
Biomass combustion emissions in developed countries
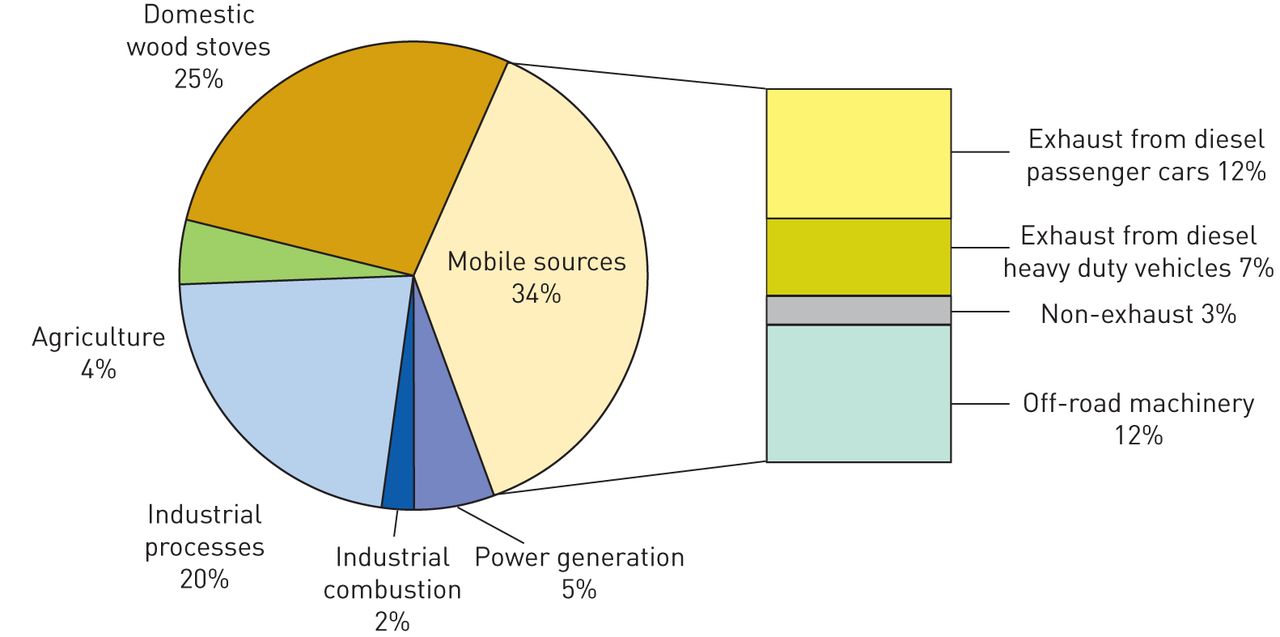
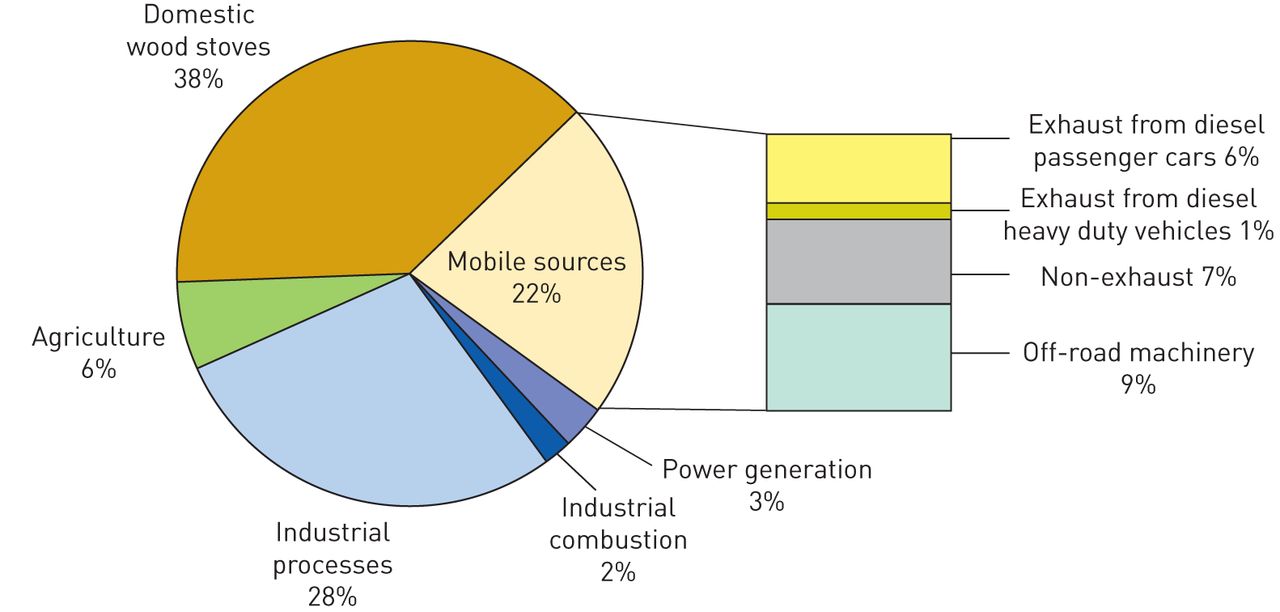
Estimates from several countries have shown that biomass (primarily wood) burning is contributing substantially to the total concentrations of PM in the local environment. Studies from Denmark and Sweden have found air pollution concentrations from wood burning in rural areas with limited traffic to be in the same range as those from traffic in major cities [23, 24]. Estimates of the current situation for some European countries (i.e. Sweden, Finland, Germany and Austria) indicate 15–25% of particles with a 50% cut-off aerodynamic diameter of <2.5 µm (PM2.5) originate from residential biomass combustion [25] and data from Alpine valleys indicate contributions of 50% or more. From a European perspective, it has been estimated that small scale domestic wood/biomass combustion will become the dominant source of fine primary particle air pollution by 2020 [26], with a contribution of 38% of total emissions (figs 1 and 2). More recently the International Institute for Applied Systems Analysis estimated that, between 2005 and 2030, the use of biomass for energy production in the EU will double, whereas use of coal, gas and oil are all expected to decrease [27]. Another study estimated that of all external health costs occurring in Denmark as a result of Danish air pollution emissions, woodsmoke generated by domestic heating was responsible for 16% of these costs in 2000, and subsequently reached 30% in 2008 due to an 80% increase in the use of wood for domestic heating in Denmark over that period [28].

Sector contributions to primary particles with a 50% cut-off aerodynamic diameter of <2.5 µm emissions in the EU15, 2000. Reproduced from [26].

{kind=link}
{kind=link}
Sector contributions to primary particles with a 50% cut-off aerodynamic diameter of <2.5 µm emissions in the EU15, 2020. Reproduced from [26].
Within the EU, biomass is used in small scale residential (<50 kilowatt thermal (kWth)) heating appliances and in medium scale (<20 MWth) district heating/industrial systems as well as in large centralised heat and power plants. In the small and medium scale sector, a large number of units are in use and the technology covers a vast range, from the simplest fireplaces to fully automated systems. The current number of residential biomass combustion systems within the EU is estimated to be ∼65 million direct heating appliances (fireplaces, stoves and cookers) and ∼8 million indirect heating appliances (boilers), firing mainly using wood logs but also wood chips and fuel pellets [24]. The technological level has traditionally been low, as has the combustion efficiency and emission performance. It is generally understood, although poorly documented, that behavioural factors can have a large impact on residential stove emissions, including wood sizing, fuel moisture content, ignition procedure, burn temperatures and stove maintenance [29, 30]. Recent developments have resulted in modern appliances with decreased emissions, but still, these systems are often sensitive to firing procedures and are not optimised in real life-operation. Moreover, emissions during the starting phase remain magnitudes higher than in the stationary phase even in modern appliances [31, 32]. Thus, significant potential for further emission reduction remains [25].
The typical PM2.5 emission factors given range from 40–300 and 50–2000 mg·MJ−1 for modern and conventional domestic wood stoves, respectively [33]. When using humid fuels and poorly insulated stoves, the PM2.5 emissions may be significantly elevated (grammes per MJ). Emissions from such low-temperature combustion are often completely dominated by liquid droplets consisting of a complex array of organic components [34]. Combustion may also be too intense when using very dry fuel in well insulated stoves, thus resulting in so-called “air-starved” conditions. Such combustion may contain the highest emissions of carcinogenic polycyclic aromatic hydrocarbons (PAHs) and is dominated by solid agglomerated soot (black carbon) particles, which shows similarities to diesel soot [32, 35].
Modern biomass combustion technologies such as automatic small-scale wood pellet appliances and larger domestic heating plants are commonly more efficient and have much lower particle emissions in the range of 10–50 mg·MJ−1 (typically <30 mg·MJ−1) [33]. Using these technologies, organic and soot emissions may be almost completely eliminated, and the particle emissions are instead dominated by inorganic salts like potassium sulfates and chlorides, with minor amounts of zinc.
Further information on biomass combustion technology is provided in the online supplementary material.
Exposure
The contribution of woodsmoke to ambient PM mass is highly dependent on season, density of sources and the specific technologies employed as well as meteorology and topography. Studies have estimated that wood/biomass combustion contributes 10–30% or ∼1–4 µg·m−³ to the annual average fine particle concentrations measured in different parts of Europe. Details of the studies and methods applied can be found in the online supplemental material. Tables S1–S3 show the contributions of biomass combustion to outdoor and indoor PM concentrations in the developed world. In some cases wood combustion is the major source of ambient PM, especially during the heating season. Woodsmoke also contributes substantially to some of the particle components that are considered particularly harmful such as particle-bound PAH, volatile organic compounds and metals [23, 36–40].
While air pollution from woodsmoke is often highest in close vicinity to houses where and when wood burning takes place [40], there is also a more global contribution of biomass combustion from indoor heating and cooking, energy production, and from agricultural and wild fires even at distant background stations [41] and over the oceans [42]. Outdoor woodsmoke concentrations may be less predictive for individual exposure compared with other air pollutants because of the potential for wood stoves to emit pollution indoors, and wood combustion for heating occurs in locations and during periods when indoor infiltration may be relatively low due to building construction (insulation) and operation (closed windows) [43, 44]. Therefore, unsurprisingly, studies evaluating fine particle levels in homes with wood-burning appliances have given mixed results, ranging from indoor particles with a 50% cut-off aerodynamic diameter of <10 µm (PM10) levels as high as 100 µg·m−³ [45, 46] to only minor differences between indoor concentrations measured in homes with and without wood burning appliances. In a few studies looking at woodsmoke tracers, significant differences (66–80%) were observed for potassium, calcium and zinc as well as 1,3-butadiene and benzene [47, 48]. In one study, the levels of benzo(a)pyrene and several other PAHs were found to be three- to five-fold higher in homes with wood combustion appliances compared with homes without [49].
Epidemiology
Health effects of anthropogenic biomass combustion products in the developed world
Whereas there is a vast literature on health effects of indoor air pollution from biomass burning in the developing world [11], comparatively few studies have addressed health effects of biomass burning in the developed world. We will first discuss epidemiological observations from areas where biomass combustion (mostly wood burning) is a relatively important source of ambient air pollution. We will then discuss smaller-scale studies of populations living in homes using wood for heating and/or cooking.
Several studies have looked at the health effects of air pollution in Seattle, USA and Vancouver, Canada where, in winter, residential wood burning is an important contributor to outdoor PM pollution. A time series study conducted in Seattle documented that in the cold season, ambient PM2.5 was associated with total and cardiovascular (but not respiratory) mortality [50]. Interestingly, potassium, a marker of woodsmoke, also showed positive associations with total and cardiovascular mortality in the cold season. A study from Vancouver also showed positive associations between PM10 in winter and total mortality [51].
Other studies from Seattle found associations between PM and respiratory symptoms (chest congestion and wheeze) in young children [52], increased medication use [53], decreased lung function [54], emergency room visits for asthma [55] and hospitalisations [56]. Smaller studies on cardiovascular morbidity end-points generally found little evidence for effects on sudden cardiac arrest [57], myocardial infarction [58], heart rate variability [59], and measures of systemic inflammation or thrombosis [60].
There are few epidemiological studies of chronic or sub-chronic exposure to biomass PM resulting from residential wood burning as a heat source. In metropolitan Vancouver, extensive mobile monitoring and geospatial modelling were used to develop a spatio-temporal model of ambient winter woodsmoke [61], which was applied to a variety of health outcomes. Positive associations were reported with low birth weight [62], infant bronchiolitis [63], otitis media [64] and COPD hospitalisation. However, no association was found for COPD mortality [65] or for incident childhood asthma [66].
A study conducted in southern California reported significant positive associations between the biomass combustion source fraction and preterm birth [67], although not with term low birth weight [68], which was also not associated with PM mass.
In Europe, some studies have estimated the acute exposure impacts of particle source apportionment in locations where biomass combustion is a more minor contributor to ambient PM. For example, in a study conducted in Copenhagen, associations were reported between the biomass source fraction and respiratory and cardiovascular hospital admissions in the elderly (age >65 years), but not for asthma-related admissions among children [69]. Of these, only the associations with respiratory admissions remained significant after adjustment for the contributions from other sources.
In Christchurch, New Zealand, source apportionment studies indicated that 90% of wintertime PM originated from wood combustion, and ambient PM10 was associated with increased respiratory and cardiovascular (excluding ischaemic heart disease) hospital admissions [70]. In a study conducted in Temuco, Chile, where an estimated 87% of winter PM10 was attributable to wood combustion, PM10 was associated with cardiovascular and respiratory mortality, hospitalisations, and emergency room visits for acute respiratory infections [71]. This study was conducted in an area where the average PM10 concentration was 46 μg·m−3 with daily means often well above 150 μg·m−3, i.e. much higher than concentrations measured in Seattle, USA and Vancouver, Canada.
Health impacts of community and household stove interventions
Studies of community- or household-level health impacts following wood stove intervention strategies have been limited. Table 1 highlights results on effects of interventions such as wood stove change out programmes on ambient PM levels in the developed world; table S2 shows the effects on indoor PM concentrations. A 4-year, survey-based study tracked parent-reported respiratory symptoms and conditions among school children during the community wood stove exchange in Libby, Montana, USA. Significant reductions in reported frequency per 5 µg·m−3 decline in ambient PM2.5 were observed for wheeze (27%), irritant symptoms such as watery eyes (33%), cold (25%), bronchitis (55%), flu (52%) and throat infection (45%) [75]. No significant reductions were observed for reported ear infection, but the population studied was not in the age group most commonly impacted by this condition. In the same community, no consistent effects were observed for school absences.
Effects of wood stove interventions on outdoor particulate matter (PM) levels in developed countries
In Launceston, Tasmania, Australia, substantial mortality changes were observed between the period before (1994–2000) and after (2001–2007) a government-coordinated fuel switching effort. The investigators demonstrated significant reductions in male mortality only: 18% from cardiovascular causes and 28% from respiratory causes [72]. Similar findings of borderline significance were observed for winter mortality for both sexes combined.
Finally, a high-efficiency particulate air filter intervention crossover study examined changes in microvascular endothelial function as measured by reactive hyperaemia index (RHI) as well as changes in serum and urine markers of oxidative stress and inflammation [77]. In this study, filtration units were placed in homes with and without wood stoves to reduce indoor PM concentrations. The use of the filter was associated with significantly higher mean measures of RHI (9%) and significantly lower mean measures of the inflammatory marker C-reactive protein (CRP) (33%). These findings remained robust when the analyses were restricted to participants in wood stove homes, but not among participants in non-wood stove homes. Smaller magnitude and nonsignificant changes in RHI and CRP were found when modelled per µg·m−3 reduction in indoor PM2.5 rather than per filter on/off status, possibly reflecting between-home variability in smoke infiltration. A recent study conducted in an urban area at very low levels of ambient and indoor PM2.5 was, however, not able to reproduce these findings [78].
Wild fires
The respiratory health effects associated with wildfire smoke exposure have recently been reviewed in detail [79, 80], and are summarised here to provide supporting evidence of the health impacts resulting from exposure to biomass combustion products. Similar to the literature described above for domestic biomass combustion, wildfire smoke exposure was associated with respiratory symptoms, increased asthma medication use, outpatient physician visits, emergency room visits, hospital admissions and mortality. Stronger associations were observed for asthma-specific physician visits, hospitalisations and emergency room visits, as well as for respiratory symptoms among individuals with asthma compared with non-asthmatic individuals. Relatively few studies have reported on the relationship between cardiovascular outcomes and wildfire smoke, with varying specificity in exposure estimates. A number have reported null associations for mortality [81], hospital admissions [82] and outpatient physician visits [83], despite evidence of positive associations for measures of respiratory health. However, several recent studies have reported associations between forest fire smoke exposure and cardiac outcomes including emergency visits for heart failure [83], out of hospital cardiac arrest [84–86] and cardiac mortality [87, 88].
Toxicity of woodsmoke particles
The physicochemical properties of biomass combustion PM varies between different combustion conditions. As discussed in the online supplementary material, the heterogeneity of biomass PM characteristics is high. Accordingly, evaluation of the respiratory and cardiovascular toxicity of biomass emission PM is complex. The limited knowledge of physicochemical properties of ambient (real-life) biomass PM exposure further complicates the evaluation of the possible health risks associated with biomass PM exposure.
Impact of combustion conditions and particle properties
Woodsmoke particles constitute a complex and variable mixture of organic-dominated particles, soot agglomerates and inorganic ash alkali particles; three particle types that differ considerably in shape, size, solubility and chemical composition [89]. Health relevant properties of these particle types are described in more detail in the online supplementary material. These differences in physicochemical properties may affect various aspects of PM-induced toxicity, including pulmonary deposition, clearance and cellular effects. For instance, soluble inorganic ash particles are cleared rapidly from the lungs compared with insoluble soot agglomerates. The pulmonary deposition is determined by size, shape and hygroscopicity. For biomass PM, hygroscopic particle growth in the respiratory tract has a large impact on particle deposition probability [90–92]. Biomass PM from complete and incomplete combustion exhibited relatively low deposited fractions in the respiratory tract, while ambient woodsmoke PM (likely originating from mixed combustion conditions) resulted in larger deposited fractions. Although the ambient woodsmoke deposition was lower than for vehicular traffic particles (38% versus 69% for particle number concentrations), the alveolar deposited fractions were estimated to be ∼20% for both types of particles [92]. Differences in pulmonary deposition for different types of biomass PM possibly affect the severity of the respiratory and cardiovascular effects, but this has not been specifically addressed in human inhalation studies. In cell culture studies, the chemical composition and combustion conditions have a large impact on the cellular effects induced by biomass PM. Various organic compounds influence the biological effects of PM resulting from poor combustion, whereas metals are of major importance for the effects induced by inorganic ash particles from complete combustion [89, 93–95]. These findings have also been confirmed in vivo in two short-term instillation studies of different types of biomass PM [94, 95]. It is important to keep in mind that these in vitro and in vivo studies do not account for differences in pulmonary particle deposition and clearance, which are also influenced by the combustion conditions and the resulting PM properties. Physicochemical ageing in the atmosphere, by reaction of the emissions with hydroxyl radicals and ozone, chemically transforms the primary biomass PM. For example PAHs may be transformed to quinones and nitro-PAHs [96]. This also leads to formation of low volatility vapours that add new secondary organic particle mass (on the timescale of minutes to days). Currently, it is not known if atmospheric ageing leads to increased or decreased toxicity. An initial study showed effects of ageing by ozone on biomass PM characteristics and toxicity [97].
Toxicological effects related to human health
Human controlled exposure studies report that short-term inhalation of woodsmoke induces mild inflammatory effects including distal airway inflammation, increased oxidative stress and immune cell recruitment, but no effects on measures of lung function [98–103]. Studies also report systemic effects such as increased levels of coagulation markers, and decreased heart rate variability and systemic inflammation [100, 104–107]. In mice and rats, long-term inhalation of woodsmoke in concentrations relevant for ambient exposure induces mild inflammatory effects in the airways, systemic inflammation and decreased lung function [17, 108–112]. Woodsmoke PM has also been reported to exacerbate allergic inflammation and allergic sensitisation, and to decrease pulmonary macrophage function in terms of impaired infection resistance [17, 109, 112–114], this was recently demonstrated to apply equally to particles from Malawian and Norwegian woodsmoke [115]. Overall, in vivo and in vitro experiments demonstrate that woodsmoke PM can induce inflammatory responses, cytotoxicity, genotoxicity, oxidative stress and immunosuppressive effects [17, 93–95, 104, 111, 116–122]. Atopy alone did not appear to increase susceptibility to the toxic effects of woodsmoke PM [123], whereas conditions affecting deposition, such as pre-existing lung disease, have yet to be studied in biomass combustion product experiments.
While some human inhalation studies report significant respiratory and systemic effects, other studies have not found these. This ambiguity could partly be due to the great heterogeneity in experimental set-ups, fuel type, biomass exposure generation and physicochemical properties of PM. Interestingly, the two studies reporting significant effects for either respiratory or cardiovascular end-points applied biomass PM originating from flaming combustion of wood logs in conventional stoves, rendering emissions of soot and organics [98, 99, 104, 105]. Other studies applied PM from more complete or more incomplete (smouldering) combustion conditions. This may point towards an influence of combustion conditions and physicochemical properties on the effects reported in the human exposure studies.
The high variability in respiratory and cardiovascular effects reported in the human inhalation studies could be due, in part, to differences in the physicochemical properties of the applied biomass PM. This reflects the inherent complexities in the evaluation of health risks from a very heterogeneous class of PM. The mild inflammatory effects following short-term, controlled inhalation of woodsmoke in healthy individuals are in accordance with the mild inflammatory effects reported in animal models. However, these data cannot be extrapolated to long-term exposure scenarios or effects in susceptible individuals. Also, based on the current, limited experimental findings, we cannot conclude that exposure to residential biomass emissions in developed countries is less harmful than exposure to combustion particles from fossil fuel combustion.
Policy implications
Air pollution arising from wood burning has been recognised as a problem for some time in Scandinavian and Alpine countries, especially during the winter period. Across Europe, the Renewable Energy Directive has set a goal to produce 20% of energy from renewable sources by 2020, increasing wood/biomass combustion for power generation. As mentioned in the Introduction, biomass combustion is expected to become the major source of primary PM emissions over the next 5–15 years. This will compromise efforts to reduce ambient PM concentrations to below the current WHO Air Quality Guidelines. This, in turn, will probably result in large numbers of avoidable, premature deaths across Europe over that time period.
Between 2010 and 2020, biomass burning is forecast to increase by 57–110% across the EU [124]. The UK alone is stimulating through financial incentives 700 000 homes to convert to biomass heating systems, and biomass boilers are increasingly installed to meet renewable energy requirements.
So far, the emission limits that exist within the EU and the rest of the developed world for new small-scale biomass combustion devices are rather tolerant and easily fulfilled by today's systems. The measuring methods applied and emission limits still vary, thus the need for harmonisation is obvious. To date, insufficient efforts have been made towards the development of particulate emission control devices for these units. The situation is, however, currently under revision, and considerably tougher and harmonised emission standards are under discussion within the EU (e.g. related to the EcoDesign directive). In parallel with new technological solutions, it is also important to educate wood stove owners in the best wood burning practices based on recent research. Still, a considerable pollution contribution from existing residential installations will most probably continue.
Furthermore, it is expected that smaller, decentralised biomass installations will become more important in future energy supply scenarios. To enable an increased bioenergy sector, unexploited raw materials other than those based on stem wood (e.g. from forestry, agricultural sector and industrial residues) will have to be utilised. Compared with traditional wood fuels, these fuels have a higher content of fine particle forming ash matter and trace metals [125].
As outlined earlier in this review, there is increasing evidence of adverse health effects of wood/biomass combustion emissions as currently dominated by those from small inefficient stoves, which places this renewable energy source in direct conflict with its perception as a healthy source of energy and domestic heating. The potential for adverse health effects associated with biomass emissions also conflicts with their role in reducing other exposures forcing climate change. A conservative estimate of the current contribution of biomass smoke to premature mortality in Europe would amount to at least 40 000 deaths per year. This is based on a contribution of biomass smoke to population exposure of 10%, and recent estimates of the total mortality burden due to PM exposure in Europe (EU28) of over 400 000 premature deaths each year [126]. A recent WHO report estimated that ambient PM from residential heating with wood and coal is responsible for 61 000 premature deaths per year in the EU28 [127]. This latter estimate is dominated by woodsmoke.
Modern and more efficient biomass technologies are available, and further development and implementation of such systems are clearly motivated from an air pollution mitigation perspective. In addition, an important regulatory step would be the unconditional adoption of the PM10 and PM2.5 WHO annual mean Air Quality Guideline values to protect public health [128]. Compliance with these science-based guideline values (annual mean PM10 and PM2.5 concentrations of 20 and 10 μg·m−3, respectively) would inevitably require the development and implementation of clean air strategies and “best available technology” for biomass combustion, comparable to the EU control policies for vehicle emissions.
Conclusions
Biomass combustion is widespread, is increasing, and makes an important contribution to ambient PM2.5, especially in winter, in the developed world.
Epidemiological studies strongly suggest that there are adverse health effects related to short-term as well as long-term exposure to biomass smoke in the developed world. Intervention studies performed, to date, suggest beneficial health effects of reducing exposure to biomass smoke. We recommend that emissions from biomass combustion should be kept to a minimum to protect public health.
As the evidence from studies in the developed world is still limited, further studies are necessary to more precisely quantify the adverse health effects of biomass combustion. This should include comparative studies to document similarities and differences between effects of combustion products from biomass and fossil fuels.
Acknowledgements
This position paper is the result of a workshop convened and supported by the European Respiratory Society in Brussels, Belgium, March 6–7, 2014. We sincerely thank the constructive assessment and many suggestions received from the European Respiratory Journal peer reviewers, which significantly increased the quality and scope of our original submission.
Footnotes
The authors alone are responsible for the views expressed in this publication and they do not necessarily represent the decision or stated policy of the World Health Organization.
This article has supplementary material available from erj.ersjournals.com
Conflict of interest: Disclosures can be found alongside the online version of this article at erj.ersjournals.com
- Received October 8, 2014.
- Accepted September 1, 2015.
- The content of this work is copyright of the authors or their employers. Design and branding are copyright ©ERS 2015
References










