





Figures
- FIGURE 1
Flow diagram of study cohort. PH: pulmonary hypertension; mPAP: mean pulmonary artery pressure; PCWP: pulmonary capillary wedge pressure; WHO: World Health Organization; IPAH: idiopathic pulmonary arterial hypertension; CTD-PAH: connective tissue disease-associated pulmonary arterial hypertension; BB: β-blocker.
- FIGURE 2
a) β-blockers used in pulmonary hypertension patients. “Others” include bisoprolol, propranolol, nebivelol and sotalol. n=193. Some patients received more than one β-blocker. b) Reasons for β-blocker initiation. “Others” include palpitations, autonomic dysfunction, peri-operative and thyroid disorders. n=193. c) Reasons for β-blocker discontinuation. “Others” include bronchospasm and unknown. n=60. CCF: congestive cardiac failure; CAD: coronary artery disease; SoB: shortness of breath.
- FIGURE 3
Propensity score-adjusted Kaplan–Meier analysis. a) Estimated survival of entire study cohort stratified by β-blocker therapy (relative risk 0.92, 95% CI 0.66–1.28; p=0.63); b) probability of clinical worsening over time in study patients stratified by β-blocker therapy (relative risk 0.93, 95% CI 0.66–1.32; p=0.70); c) probability of survival stratified by β-blocker therapy in the idiopathic pulmonary arterial hypertension (IPAH) subgroup (relative risk 0.57, 95% CI 0.31–1.05; p=0.7); d) estimated clinical worsening events stratified by β-blocker therapy in IPAH patients (relative risk 0.69, 95% CI 0.46–1.02; p=0.07); e) estimated survival with β-blocker therapy in the connective tissue disease pulmonary arterial hypertension (CTD-PAH) subgroup (relative risk 1.14, 95% CI 0.76–1.70; p=0.53); f) probability of clinical worsening events with β-blocker therapy in the CTD-PAH cohort (relative risk 1.01, 95% CI 0.72–1.41; p=0.97). Numbers beneath each chart denote the populations at risk. The aOR for mortality with β-blocker use is 0.98 (95% CI 0.57–1.69) at 5 years and 0.44 (95% CI 0.25–0.77) at 10 years for the overall study population. Similarly, aOR for clinical worsening events with β-blocker use is 0.73 (95% CI 0.42–1.27) at 5 years and 0.54 (95% CI 0.30–0.99) at 10 years. BB: patients who used β-blockers and continued to do so until they reached the end-points of the study; no BB: patients who had never used β-blockers.
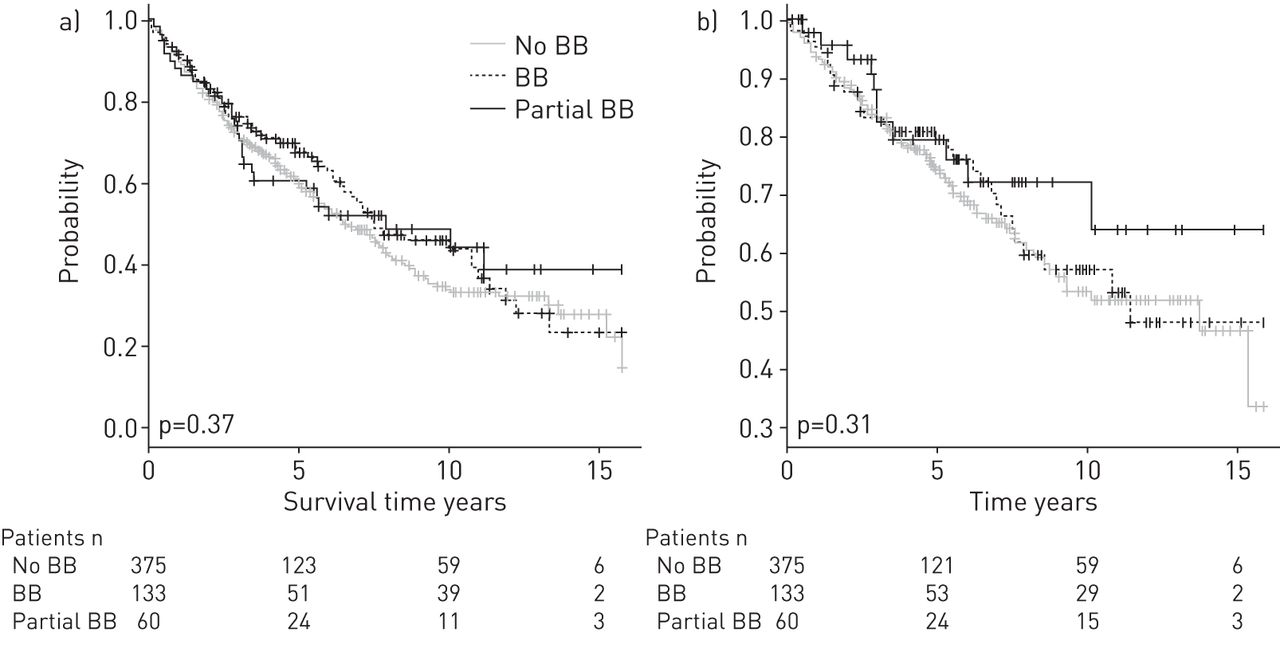
- FIGURE 4
Outcome analyses of the three groups of the study population: patients in the BB group continued to use a β-blocker; the no BB group had never used β-blockers and the partial BB group had started β-blocker therapy but it was discontinued because of side-effects. Numbers beneath each chart denote the populations at risk. a) Kaplan–Meier plot of probability of survival stratified by β-blocker therapy (relative risk 0.92, 95% CI 0.78–1.10; p=0.37); b) Kaplan–Meier plot of estimated time to clinical worsening events stratified by β-blocker therapy (relative risk 0.92, 95% CI 0.81–1.07; p=0.31).
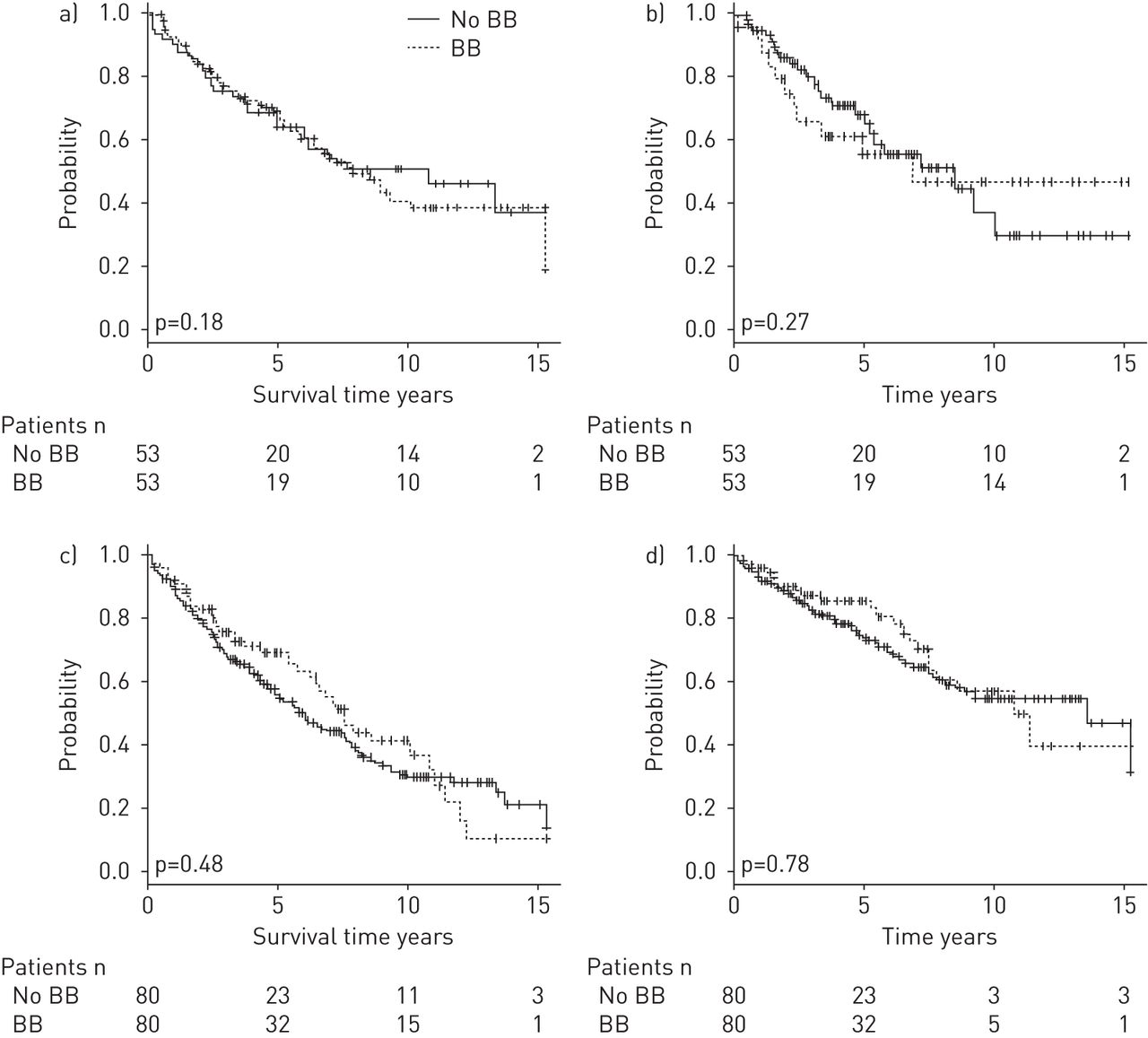
- FIGURE 5
Propensity-matched outcome analyses based on New York Heart Association (NYHA) class at presentation. The study population was divided into two groups: NYHA classes I and II and NYHA classes III and IV at diagnosis. Numbers beneath each chart denote the populations at risk. a) Kaplan–Meier plot of estimated survival with β-blocker therapy for those patients in NYHA classes I and II at presentation (relative risk 0.71, 95% CI 0.43–1.17; p=0.18); b) Kaplan–Meier plot of likelihood of clinical worsening events over time with β-blocker therapy for those patients in NYHA classes I and II at presentation (relative risk 0.78, 95% CI 0.51–1.21; p=0.27); c) Kaplan–Meier plot of estimated survival with β-blocker therapy for those patients in NYHA classes III and IV at presentation (relative risk 1.19, 95% CI 0.74–1.91; p=0.48); d) Kaplan–Meier plot of likelihood of clinical worsening events over time with β-blocker therapy for those patients in NYHA classes III and IV at presentation (relative risk 1.05, 95% CI 0.72–1.54; p=0.78). BB: patients who used β-blockers and continued to do so until they reached the end-points of the study; no BB: patients who had never used β-blockers.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Baseline characteristics of the study population
Characteristics BB No BB Partial BB p-value Subjects n 133 375 60 Age years 59±14 57±16 55±16 0.22 BMI kg·m-2 29±8 28±8 26±6 0.12 Race 0.84 Caucasian 97 (73) 280 (75) 40 (67) African-American 27 (20) 70 (18) 12 (20) Hispanic 4 (3) 15 (4) 7 (1) Asian 5 (4) 10 (3) 3 (0.5) Sex 0.24 Male 46 (35) 109 (29) 23 (38) Female 87 (65) 265 (71) 37 (62) Smoking history 0.27 Never smoked 74 (56) 229 (61) 37 (62) Ex-/current smoker 59 (44) 149 (39) 23 (38) Aetiology of PAH 0.005 Idiopathic 47 (35) 186 (50) 27 (45) Connective tissue disease 86 (65) 189 (50) 33 (55) Co-existing cardiac illness Coronary artery disease 13 (9) 47 (12) 7 (12) 0.38 Valvular heart disease 13 (10) 36 (10) 9 (15) 0.95 Cardiac arrhythmias 27 (20) 80 (21) 13 (22) 0.79 Dyslipidaemia 54 (41) 158 (42) 20 (33) 0.76 Pericardial effusion 21 (27) 54 (21) 10 (17) 0.24 Comorbidities Diabetes mellitus 27 (22) 73 (20) 14 (23) 0.63 Renal failure 31 (23) 88 (23) 16 (26) 0.64 Hypertension 27 (20) 72 (19) 13 (22) 0.78 Sleep apnoea 12 (9) 45 (12) 7 (13) 0.94 LVEF % 56±7 56±8 58±8 0.56 Heart rate beats·min-1 71±17 84±15 74±19 0.01 Pro-BNP pg·mL−1 780±218 349±852 511±403 <0.016 Baseline NYHA functional class# 0.52 I 2 (0.5) 0 II 48 (38) 125 (34) 10 (19) III 58 (46) 180 (48) 26 (43) IV 20 (16) 62 (17) 16 (25) Baseline 6MWD m 286±111 303±102 221±59 0.15 Follow-up months median (range) 81 (1.5–247) 75 (1–388) 31 (1.5–145) 0.41 Transplant 9 (7) 25 (7) 4 (7) 0.97 Mortality 69 (52) 184 (49) 32 (53) 0.57 Data are presented as mean±sd or n (%), unless otherwise stated. BB: patients who had continued to use β-blockers until they reached the end-points of the study; no BB: patients who had never used β-blockers; partial BB: patients who were started on β-blocker therapy but discontinued after a period; BMI: body mass index; PAH: pulmonary arterial hypertension; LVEF: left ventricular ejection fraction; BNP: brain natriuretic peptide; NYHA: New York Heart Association; 6MWD: 6-min walking distance. #: n=126 (BB), n=369 (no BB) and n=52 (partial BB).
- TABLE 2
Pulmonary hypertension profiles of the patients at diagnosis
BB No BB Partial BB p-value Subjects n 133 375 60 RA dilatation 75 (97) 250 (97) 60 (100) 0.82 RV dilatation 61 (79) 206 (80) 46 (77) 0.90 TR jet velocity cm·s-1 407±71 405±73 435±61 0.74 Positive bubble study 8 (10) 27 (11) 4 (7) 0.97 RVSP mmHg 73±23 74±24 77±27 0.68 sPAP mmHg 74±19 75±21 81±23 0.41 dPAP mmHg 30±9 32±11 35±12 0.08 mPAP mmHg 45±11 47±14 51±16 0.08 PCWP mmHg 9±3 10±6 10±3 0.16 Pulmonary vascular resistance Wood units 9±5 10±6 11±7 0.16 Cardiac index (Fick) L·min-1·m-2 2.6±0.9 2.4±2 2.5±1.8 0.04 Cardiac output (Fick) L·min-1 4.9±2 4.5±2 4.5±2 0.04 Pulmonary arterial oxygen saturation % 63±12 64±13 62±11 0.41 PAH medications Epoprostenol 33 (25) 127 (34) 21 (35) 0.05 Sildenafil 66 (50) 144 (38) 28 (46) 0.02 Bosentan 32 (24) 112 (30) 20 (33) 0.20 Treprostinil 11 (8) 41 (11) 8 (13) 0.37 Ambrisentan 15 (11) 18 (5) 9 (15) 0.10 Tadalafil 12 (9) 19 (5) 6 (10) 0.10 Iloprost 4 (3) 11 (3) 3 (5) 0.96 Oxygen therapy 29 (22) 84 (23) 17 (28) 0.86 Data are presented as n (%) or mean±sd, unless otherwise stated. n=568. BB: patients who had continued to use β-blockers until they reached the end-points of the study; no BB: patients who had never used β-blockers; partial BB: patients who were started on β-blocker therapy but discontinued after a period; RA: right atrium; RV: right ventricle; TR: tricuspid regurgitation; RVSP: right ventricular systolic pressure; sPAP: systolic pulmonary artery pressure; dPAP: diastolic pulmonary artery pressure; mPAP: mean pulmonary artery pressure; PCWP: pulmonary capillary wedge pressure; PAH: pulmonary arterial hypertension.
- TABLE 3
Effects of β-blocker therapy in pulmonary arterial hypertension patients: propensity-adjusted outcome analysis
Unadjusted Optimal matching Mortality OR (95% CI) 1.11 (0.75–1.66) 1.13 (0.69–1.82) Clinical worsening events OR (95% CI) 1.01 (0.64–1.60) 0.96 (0.55–1.68) Transplant OR (95% CI) 1.02 (0.46–2.23) 1.17 (0.39–3.47) Hospitalisation OR (95% CI) 0.89 (0.60–1.32) 1.06 (0.66–1.32) NYHA class change from baseline Year 1 -0.12 (-0.35–0.10) 0.03 (-0.24–0.30) Year 3 0.11 (-0.53–0.31) 0.07 (-0.53–0.40) Year 5 0.24 (-0.01–0.49) 0.17 (-0.15–0.48) 6MWD m Baseline -15 (-42–12) -3 (-36–30) Follow-up -15 (-50–20) -23 (-69–22) Data are presented as mean difference (95% CI), unless otherwise stated. NYHA: New York Heart Association; 6MWD: 6-min walking distance.
Supplementary material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
- Data supplement - This supplement contains additional figures E1, E2 and E3.










