





Abstract
Chronic obstructive pulmonary disease (COPD), lung cancer, asthma and pulmonary tuberculosis are common pulmonary diseases that are caused or worsened by tobacco smoking. Growing observational evidence suggests that symptoms and prognosis of these conditions improve upon smoking cessation. Despite increasing numbers of (small) randomised controlled trials suggesting intensive smoking cessation treatments work in people with pulmonary diseases many patients are not given specific advice on the benefits or referred for intensive cessation treatments and, therefore, continue smoking.
This is a qualitative review regarding smoking cessation in patients with COPD and other pulmonary disorders, written by a group of European Respiratory Society experts. We describe the epidemiological links between smoking and pulmonary disorders, the evidence for benefits of stopping smoking, how best to assess tobacco dependence and what interventions currently work best to help pulmonary patients quit. Finally, we describe characteristics and management of any “hardcore” smoker who finds it difficult to quit with standard approaches.
Abstract
Smoking cessation is crucial for respiratory patients: every patient must be given advice and help to quit http://ow.ly/ITgsW
Methodology
This document was written as part of an initiative from a European Respiratory Society (ERS) Task Force with methodological support from ERS. We followed the following procedures.
1) C. Jiménez-Ruiz, P. Tonnesen and K. Lewis searched MEDLINE between January 1, 2002 and December 31, 2013. The keywords describing the patient population were “chronic obstructive pulmonary disease”, “chronic obstructive lung disease”, “emphysema”, “COPD”, “chronic bronchitis”, “lung cancer”, “bronchial cancer”, “thoracic cancer”, “asthma”, “tuberculosis” and “pulmonary tuberculosis”. The keywords describing smoking cessation interventions were “smoking”, “smoking cessation”, “tobacco”, “tobacco use cessation”, “smoking cessation programme”, and “quit”. Studies were included according to the following criteria: 1) dealing with patients with chronic obstructive lung disease (COPD) or lung cancer or asthma or tuberculosis (TB); 2) randomised controlled trials (RCTs) and longitudinal studies; 3) evaluation of a smoking cessation intervention; and 4) published in English.
2) Based on the included studies, C. Jiménez-Ruiz, S. Andreas, K. Lewis and P. Tonnesen produced a first manuscript providing a narrative review of the selected studies. The manuscript was circulated among all members of the Task Force. Each member added comments and suggestions to this manuscript. K. Lewis and C. Jiménez-Ruiz led the redrafting following the reviewer's comments.
3) The first manuscript was revised according to the comments and suggestions from all Task Force members and recirculated.
4) Finally, the manuscript obtained approval from all members of the Task Force. This document is a statement on smoking cessation in COPD and other pulmonary diseases, and the management of smokers with comorbidities that find it difficult to quit.
Introduction
Two previous ERS documents concerning smoking exist: the CEASE (Collaborative European Anti-Smoking Evaluation) trial conducted on behalf of ERS by the Occupational and Epidemiology Assembly [1]; and the report from another ERS Task Force on smoking cessation in patients with respiratory diseases by Tønnesen et al. [2], from 2007. The main conclusions from CEASE trial were as follows: a higher than standard dose of nicotine patch was associated with an increase in the long-term success of smoking cessation, but continuation of treatment beyond 8±12 weeks did not increase the success rates [1]. The main conclusions from the 2007 ERS Task Force were as follows. 1) Patients with respiratory disease have a greater and more urgent need to stop smoking than the average smoker, so respiratory physicians must take a proactive and continuing role with all smokers in motivating them to stop and in providing treatment to aid smoking cessation. 2) Smoking cessation treatment should be integrated into the management of the patient's respiratory condition. 3) Therapies should include pharmacological treatment (i.e. nicotine replacement therapy (NRT), bupropion or varenicline) combined with behavioural support. 4) Respiratory physicians should receive training to ensure that they have the knowledge, attitudes and skills necessary to deliver these interventions or to refer to an appropriate specialist. 5) Although the cost of implementing these recommendations will partly be offset by a reduction in attendance for exacerbations, etc., a budget should be established to enable implementation [2].
More recently, the SmokeHaz website has been created [3]. SmokeHaz is a collaboration between ERS and the UK Centre for Tobacco and Alcohol Studies. The two organisations agreed to join forces, and work with the European Lung Foundation, to provide a website aimed at policymakers primarily focused on the respiratory health hazards associated with smoking. The aim of the SmokeHaz website is to provide a one-stop web platform assessing the relationship between active and passive smoking and a range of specific health outcomes, particularly focusing on lung health. Robust methods were used to gather together all of the available scientific studies that provided an unbiased account of the true relationship between smoking and health. These methods included systematic reviews and meta-analyses [3].
This statement follows in this tradition, with the aim to provide an up-to-date review of current developments in this field.
Smoking cessation in patients with COPD
Smoking as a cause of COPD
COPD is a progressive, multisystem inflammatory disease characterised by airflow limitation. It is one of the most common respiratory disorders with a prevalence of 8–13% among adults in Europe and North America with many remaining undiagnosed [4, 5]. The prevalence is increasing and rises with age [4, 5].
There is a strong relationship between smoking and the development of COPD. ∼40% of COPD patients in the developed world are smokers or ex-smokers. Epidemiological studies show that smoking is linked to a deterioration of pulmonary function [6, 7]. Smoking during adolescence inhibits the normal expansion of pulmonary function during growth and the forced expiratory volume in 1 s (FEV1) later in life [8]. Smoking lowers the age at which FEV1 begins to decline [9], and also accelerates the annual decrease of FEV1 in late adulthood [7, 10, 11].
Smoking cessation remains the most effective intervention that reduces lung function decline in COPD [12], slowing the annual decrease of FEV1 to a rate comparable with that of nonsmokers [6, 13]. FEV1 initially increases after smoking cessation [9, 14] and quitters show a better response to bronchodilators [11] and inhaled corticosteroids (ICS) [15].
Nevertheless, ∼40% of COPD patients remain smokers. In a recent multicentre, interventional study of bronchodilator therapy 40% of participants with established moderate-to-severe COPD were current smokers [16]. Similar data have been reported from epidemiological studies [17, 18].
Characteristics of smokers with COPD
Smokers with COPD have specific features that may make it harder for them to quit [17–19]. Two studies reported that smokers with COPD scored higher on the Fagerström Test for Nicotine Dependence (FTND) and that the number of cigarettes smoked daily was significantly higher compared with smokers without COPD [17, 18]. Another study found that each additional FTND point was associated with an increase of 11% in the probability of developing COPD [19]. These results suggest that smokers with COPD are more nicotine dependent, but it is also possible that persons with a higher degree of dependence run a higher chance of developing COPD.
Some studies report smokers with COPD inhale a greater volume of smoke and inhale more deeply than smokers without COPD, so more toxic substances reach the lungs [12]. This is perhaps confirmed by the observation that smokers with COPD had higher expired carbon monoxide (eCO) levels than healthy smokers (although this was not statistically significant in the multivariate model) [17].
Some studies report no difference in motivation to quit between smokers with COPD and other smokers, but smokers with COPD report less self-efficacy and self-esteem impairing their ability to stop [20]. Co-existent depression was reported in 44% of (hospitalised) patients with COPD and depression is more common among smokers with COPD than in other smokers [21]. A vicious circle may result with smoking leading to COPD, and COPD to depression which itself has a negative impact on cessation in these smokers [21].
Weight gain is frequently associated with smoking cessation, but we could find no studies regarding weight gain in quitters with COPD. The adverse effect of any weight gain (on average 5–6 kg over 6 months in healthy smokers) on lung function is likely to be minimal, especially when the benefits of cessation are considered. Moreover, in underweight patients with COPD some weight gain is desirable.
In summary, many smokers with COPD have specific characteristics that reduce their chance of quitting successfully (table 1).
Benefits of smoking cessation in chronic obstructive pulmonary disease (COPD)
Assessment and recording of smoking status in patients with COPD
Several variables are associated with a successful quit in COPD. These include fewer cigarettes smoked daily, fewer years of smoking, more motivation to quit, more self-efficacy, less dependence, less depression and earlier smoking cessation experiences (fig. 1).
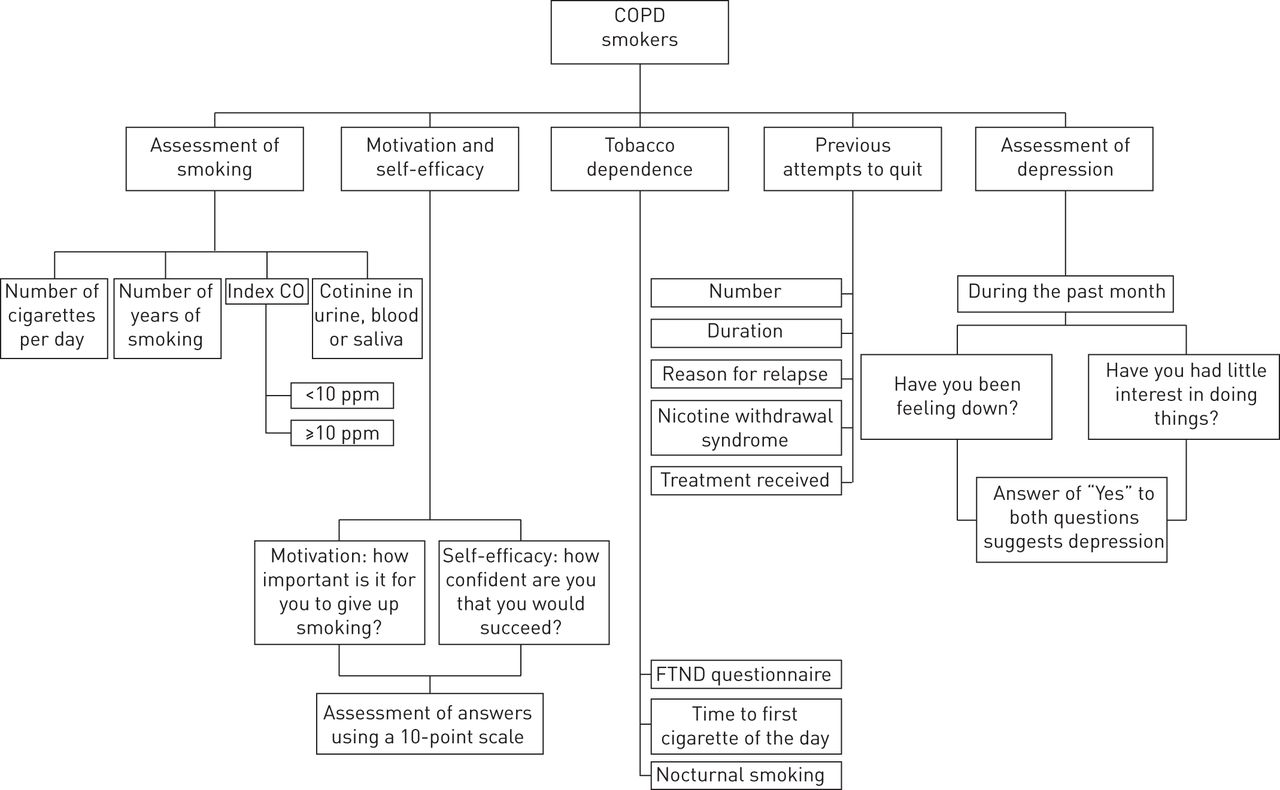
Assessment and recording of smoking status in patients with chronic obstructive pulmonary disease (COPD). FTND: Fagerström Test for Nicotine Dependence.
Assessment of the number of cigarettes smoked daily in smokers with COPD
Healthcare professionals ask all patients, including those with COPD, about smoking to assess risk and tailor treatment. For the first assessment, healthcare professionals elicit the number of cigarettes smoked daily and the number of years of smoking. Usually, cigarette consumption correlates very strongly with the risk of developing COPD, a worse stage of COPD [12] and faster progression [12, 18, 19, 22].
Alongside smoking index (in pack-years), eCO can be good indicator of the amount of smoking. Nonsmokers typically have readings between 3 and 6 ppm, while readings for smokers are generally 10 ppm or more, depending on the timing, number of cigarettes smoked and pattern of smoking. Passive smoking does not usually put the reading over 10 ppm, but shisha smoke exposure, cannabis use, faulty car exhausts, working with paint stripper, faulty gas boilers and lactose intolerance can increase eCO levels and complicate interpretation. CO monitors may be useful both to verify smoking status and to illustrate early potential health benefits [23].
A CO monitor may be used to tailor disease specific advice to COPD patients:“CO is one of the gases that you inhale when you smoke cigarettes. It displaces oxygen from your red blood cells worsening breathlessness. Cigarettes also damage your lungs over time. If you quit smoking, your CO levels will drop to normal within 24 h.”
Subsequent clinic visits have a different emphasis. Continuing smokers may be worried because they more clearly understand that smoking is impairing their health, they may use denial as a defence mechanism or be reluctant to admit to continuing to smoke. In these situations, healthcare professionals should remain empathetic and demonstrate respect by using questions such as: “What are your thoughts about smoking at this time?” Answers are frequently validated, usually with eCO levels.
Assessment of motivation and self-efficacy in smokers with COPD
Smokers with COPD usually have low self-efficacy [20] and are less motivated to quit than other smokers, both factors associated with low quit rates [20, 24]. Increasing motivation and building self-efficacy are particularly important for this group of patients. Unfortunately, validated measures for assessing the degree of motivation to quit have not yet been developed. A simple way of assessing willingness to quit is to ask:“How important is it for you to give up smoking?”
The smoker answers according to a 10-point scale, with zero being of no importance and 10 being extremely important. Further information can be obtained through motivational interviewing techniques:“You responded that your motivation was at a two. What would need to happen for you to get from your current two to an eight?”
Likewise, self-efficacy can be assessed by asking:“If you were to stop smoking how confident are you that you would succeed?” [25].
If readiness to quit and confidence are good, a quit date is usually set immediately. If motivation is high but self-efficacy is low, treatment and support are very critical for success. If self-efficacy is high but willingness to try is low, effective health education and motivational interviewing [24] are more critical. If both are low, then more intensive support is needed.
Assessment of tobacco dependence in smokers with COPD
Knowing the degree of tobacco dependence and reinforcers that maintain smoking in COPD are crucial. Three questionnaires are commonly used to measure dependence: the FTND questionnaire, the World Health Organization International Classification of Diseases and Injuries, and the Cigarette Dependence Scale [26–28]. The FTND is the most widely used of these scales and predicts difficulty of quitting, severity of withdrawal symptoms and need for pharmacological treatment [29].
Another helpful approach is an understanding of what motivates a smoker to continue: negative reinforcement (i.e. to avoid unpleasant withdrawal symptoms) appears to be more frequent than positive reinforcement (pleasure) among smokers with COPD [30–32].
Some smokers with COPD smoke a low number of cigarettes per day despite a high degree of nicotine dependence. A frequently used method to measure dependence is asking about the time to their first cigarette after waking up. Smokers who start within 30 min after waking have a high degree of dependence, while those who begin to smoke later appear to be less dependent [33]. Another indicator of high dependence is nocturnal smoking.
Assessment of depression in smokers with COPD
In smokers with COPD, healthcare professionals proactively ask about depression and assess the level of depression. For example, using two simple questions: 1) during the past month, have you been bothered by feeling down, depressed, or hopeless? 2) during the past month, have you often been bothered by having little interest or pleasure in doing things? An answer of “yes” to either of the questions is a strong sign of depression [34].
Assessment of previous attempt(s) to quit
Knowledge of previous attempts to quit is very important in helping tailor a new quit attempt. Most smokers take 4–7 attempts to successfully quit and many have tried to quit before [35, 36]. The number of attempts, duration of each abstinence, severity and timing of nicotine withdrawal symptoms, type of psychological support received and the patient's perception of its efficacy, type of pharmacological treatment received and efficacy, and reasons for relapse are often discussed and documented as such information can be useful in guiding treatment.
Smoking cessation treatment in smokers with COPD
Several meta-analyses confirm that a combination of counselling plus pharmacotherapy is the most effective cessation treatment for smokers with COPD [35–39].
Smoking cessation counselling for smokers with COPD
During the first consultation, smokers with COPD receive firm advice that tobacco smoking is the main or only cause of their illness and current symptoms (table 2). It is important they are informed that: 1) smoking cessation is the only measure that slows the progression of illness and improves prognosis; 2) inhaled treatments will not work as well with continued smoking; and 3) smoking cessation improves airflow obstruction and all of the four core symptoms of COPD (breathlessness, cough, wheeze and chest pain) [40].
Characteristics of counselling for smoking cessation in smokers with chronic obstructive pulmonary disease (COPD)
Nevertheless, most smokers with COPD have already been advised to stop smoking so may feel patronised and/or be tempted to withhold information. An empathic and non-judgmental relationship where smoking is discussed in a nonthreatening and respectful way is useful. The advice is usually short, and direct: “The best thing you can do to help your COPD is to stop smoking. I can help you with that”. This advice is repeated at every follow-up visit. There are no definite advantages to using specific words like “smokers' lung” or providing contingent reinforcement with lottery tickets, when compared with usual advice [20, 41]. A common procedure for CO monitoring is that the healthcare professional first exhales into the device, showing a normal CO concentration of 1–4 ppm. Then the smoker blows into the machine, after which she/he immediately sees a much higher reading (average of 10–20 ppm). Then the healthcare professional emphasises that the high amount of CO attaches to haemoglobin/blood molecules thereby reducing oxygen delivery all over the body. Respiratory nurses have successfully provided repeat and intensive cessation treatments for smokers with COPD [42].
At least one study supports the idea that spirometry increases motivation and even quit rates in smokers with COPD [43], but a meta-analysis found little evidence of benefit of various biomedical risk assessments (including eCO and genetic susceptibility, and eCO with spirometry) when provided in addition to cessation counselling alone [44]. A UK study randomised some smokers to being given their spirometry results described as a “lung age” (the age of the average healthy individual who would perform similar spirometry to them). A control group received a raw figure for FEV1. Both groups were advised to quit and offered referral to local smoking cessation services. 13.6% of the “lung age” group versus 6.4% of the FEV1 group quit smoking after 12 months (number needed to treat=14). The cost per successful quitter was estimated at 366 euros [45].
Healthcare professionals encourage their patients to quit immediately if in hospital or to choose a quit date, and identify high-risk situations and development of coping skills. Symptoms of nicotine withdrawal are explained using written information and self-help materials. Follow-up visits are arranged with the main or sole purpose of smoking cessation. A commonly used frequency is the first, second, eighth, 12th, 16th and 24th week after the target quit date. We could find no studies, to date, reporting the use of new technologies (apps, texts, e-mails, etc.) in COPD smokers. Group interventions are equally effective as individual support in COPD [37].
Long-term oxygen therapy assessment and prescribing in COPD provide another opportunity for intensive smoking cessation intervention [46].
Pharmacological treatment for smokers with COPD
The standard pharmacological treatments are all licensed for smokers with COPD with no additional prescribing limitations (table 3).
Pharmacological treatments for smokers with chronic obstructive pulmonary disease (COPD)
Short-acting NRT
Nicotine gum. The efficacy of nicotine gum in smokers with COPD has been shown in large-scale clinical trials. The Lung Health Study was a multicentre, randomised, controlled trial designed to determine whether a programme incorporating a smoking cessation intervention and regular use of an inhaled bronchodilator in smokers at high risk of COPD slowed the annual decline in FEV1. After 12 months, nicotine gum in combination with an intensive behavioural programme led to significantly more quitters than usual care [52]. Another open-label, randomised study of 446 consecutive smokers with pulmonary disorders (including COPD) compared four different forms of NRT and placebo. The continuous abstinence rates at 12 months follow-up were: placebo 2%, nicotine inhalator 5%, nicotine patches 9%, and nicotine inhalator plus nicotine patches 6%. All active arms were more successful than placebo (p<0.01) [53].
Dosing and duration is the same for COPD as all smokers. For those who smoke <20 cigarettes per day, or smoke their first cigarette >30 min after waking up, one 2-mg piece of nicotine gum every 1–2 h. For those who smoke ≥20 cigarettes per day, or who smoke their first cigarette within 30 min of awakening, 4-mg pieces are often used at a similar frequency. Treatment duration ranges from 8 to 12 weeks. For those with high nicotine dependence, medication may be prolonged for up to 6–12 months [54]. Nicotine gum is often used as a rescue medication to control cravings on top of other medication.
Nicotine sublingual tablets. A trial of 370 smokers with COPD compared treatment with sublingual tablets at adequate doses or placebo for 12 weeks, and also examined low and high levels of support. Smoking cessation rates were statistically significantly superior in the active treatment group at 6 and 12 months follow-up (23 versus 10% and 17 versus 10%, respectively). There was no significant difference in the effect of NRT between low and high levels of support [47].
Other study designs
In a randomised clinical trial, 247 smokers with COPD received a continuous 1-year smoking cessation programme (including a 2-week period of hospitalisation then trained staff providing feedback and encouraging comments by phone throughout the year), while 231 smokers received usual care. 52% of smokers in the continuous 1-year smoking cessation programme were abstinent after 1 year and 38% after 3 years, compared with 7 and 10%, respectively, in the control group. In spite of the high cost of this programme, beneficial economic effects were likely to be obtained in the long run [55].
Smokers with COPD who are unable or unwilling to set a quit date are advised to use NRT in a reduction-to-quit approach. This method builds self-efficacy and motivation [56]. However, a systematic review of 25 studies in all smokers (including COPD) found that smoking reduction (as opposed to quitting) has fewer quitters and does not appear to slow the accelerated decline of lung function [57]. The lack of beneficial effect of smoking reduction could be explained by compensatory deeper and longer inhalation of smoke [14, 58, 59], but may still increase cessation rates in the long-term.
Bupropion and nortriptyline. A RCT of 12 weeks of bupropion in 404 smokers with mild or moderate COPD led to a continuous abstinence rate of 16 versus 9% for placebo at 6 months [48]. Another RCT of 255 smokers with mild or moderate COPD or at risk of COPD found a continuous abstinence rate at 6 months of 28% for bupropion, 25% for nortriptyline and 15% for placebo. The only statistically significant difference was between bupoprion and placebo [49].
A similar study showed prolonged abstinence rates at 1 year of 20.9% with bupropion, 20.0% with nortriptyline and 13.5% with placebo but these were not statistically significant. Costs per quitter were 1368 euros with bupropion, 1906 euros with nortriptyline and 1212 euros with placebo [50].
A meta-analysis of 7372 smokers with COPD showed that counselling combined with NRT had the greatest effect on prolonging abstinence rates versus usual care alone (odds ratio (OR) 5.08, 95% CI 4.32–5.97; p<0.0001), and versus counselling alone (OR 2.80, 95% CI 1.49–5.26; p=0.001).The second most effective intervention overall was counselling combined with an antidepressant (OR 3.32, 95% CI 1.53–7.21; p=0.002) (and this seems more effective than in other smokers with presumably lower rates of depression). Counselling alone was of borderline superiority above usual care (OR 1.81, 95% CI 0.96–3.44; p=0.07) [35].
Varenicline. Varenicline is the most recently approved medication to aid cessation [60]. In a RCT of 504 smokers with mild and moderate COPD, treatment with varenicline for 12 weeks plus cognitive behavioural therapy resulted in a week 9–52 continuous abstinence rate of 17 versus 6% in the placebo group (OR 4.04, 95% CI 2.13–7.67) [51].
Systematic reviews of pharmacotherapy
In a systematic review, the average 12-month continuous abstinence rates for smokers with moderate-to-severe COPD were 1.4% for usual care, 2.6% for minimal counselling, 6.0% for intensive counselling and 12.3% for intensive counselling plus pharmacotherapy. Compared with usual care, the costs per quality-adjusted life year gained were 16 900 euros for minimal counselling, 8200 euros for intensive counselling and 2400 euros for intensive counselling plus pharmacotherapy [36].
In a cohort of 472 smokers with severe or very severe COPD attending a specialist smoking cessation service in Spain who were treated with a combination of pharmacotherapy and behavioural support, 49% quit at 24 weeks (quit rates on different medications were 44% with nicotine patch, 55% with bupropion and 61% with varenicline). 12 month quit rates were not reported [61].
Smoking cessation in patients with lung cancer
Smoking as a cause of lung cancer
Tobacco smoke contains over 60 known carcinogens, 85% of lung cancer cases are caused by inhaling tobacco smoke and the lifetime risk of dying of lung cancer by the age of 75 years in continuous smokers is 16% [62]. There is no threshold level of smoking under which exposure is without risk [62]. All histological subtypes of lung cancer are caused by tobacco smoke [63].
Benefits of smoking cessation in patients with lung cancer
Many studies report that smoking cessation after a diagnosis of lung cancer is associated with health improvements (table 4) [64–83].
Benefits of smoking cessation in lung cancer
Worse surgical complications in smokers
A retrospective cohort study showed that survival at 120 weeks following surgery for nonsmall cell lung cancer (NSCLC) in non- and ex-smokers was 60–70% compared with only 25% in continuing smokers [64]. There are many biological explanations for this difference including increased complications from treatment, recurrences and new incidental tumours. Data from the American Society of Thoracic Surgeons on 7990 patients undergoing primary resection of NSCLC between 1999 and 2007 showed that hospital mortality and the risk of pulmonary complications were lower not only in never or long-term ex-smokers but also in those who had stopped smoking as recently as 1–12 months before surgery [65]. These retrospective data are prone to reporting bias (especially as smoking was usually self-reported) and quitting may be a marker for other prognostic factors such as higher socioeconomic group, more compliance with medications, etc. However, a meta-analysis of RCTs in non-lung cancer surgery showed statistically significant benefits of preoperative smoking intervention on total complication rates, surgical wound complications, cardiovascular complications, re-operations and a shorter hospital stay, but individual studies (often elective procedures) were not powered for survival [66]. Earlier smoking cessation is better, with each week of cessation lowering the risk of post-operative complications by 19%. Trials of at least 4 weeks of cessation showed significantly larger effects than shorter trials [67]. Another systematic review included less well designed studies and was, therefore, reluctant to draw firm conclusions [68].
Worse response to chemotherapy in smokers
A retrospective study of 285 patients (63% current smokers) receiving platinum-based chemotherapy for lung cancer found nonresponders (n=191) to have smoked significantly more than responders (67.8±35.1 versus 38.7±27.1 pack-years; p<0.001). Multivariate analysis confirmed that heavy tobacco consumption (≥40 pack-years) was the most important independent negative predictor of response (adjusted OR 10.4, 95% CI 5.1–21.3) [69]. A small study in Asian patients yielded similar results [70].
Smoking affects drug metabolism. The epidermal growth factor receptor (EGFR) inhibitor, erlotinib is metabolised to a greater extent in smokers due to induction of the cytochrome P450 enzyme, CYP1A1/1A2 [71]. In a phase I/II study, the maximum tolerated daily dose was double (300 mg) in smokers, despite similar incidence of skin toxicity and diarrhoea, suggesting faster metabolism [72]. The dose-normalised area under the plasma concentration–time curve of irinotecan was significantly lower in smokers than nonsmokers, indicating an increased risk for treatment failure [69, 73, 74]. Smokers with NSCLC have fewer activating EGFR mutations [75, 76] and anaplastic lymphoma kinase positive driver gene alterations reducing the chances of responding to these inhibitors [74, 76].
Worse response to radiotherapy in smokers
In 83 patients receiving curative radiotherapy for NSCLC, smoking was an independent risk factor for developing radiation pneumonitis [77] and pulmonary infections [76]. Median and two-year survival rates were also longer in nonsmokers [79].
Worse survival time and increased risk of recurrence or second primary lung malignancy in smokers
In 215 patients with limited-disease small cell lung cancer (SCLC) treated with radio-chemotherapy, patients who quit smoking during therapy had a median survival time of 18.0 months versus 13.6 months for those who continued to smoke. The five-year survival rate for the two groups (8.9 versus 4.0%, respectively; p=0.0017) suggested smoking cessation before radio-chemotherapy was associated with improved long-term outcome, but whether this was a direct cause or merely a marker of other prognosticators is not known [80].
A meta-analysis of 10 RCTs and observational studies showed continued smoking was associated with a significantly increased risk of all-cause mortality (hazard ratio (HR) 2.94, 95% CI 1.15–7.54) and recurrence (HR 1.86, 95% CI 1.01–3.41) in early stage NSCLC and of all-cause mortality (HR 1.86, 95% CI 1.33–2.59), development of a second primary tumour (HR 4.31, 95% CI 1.09–16.98), and recurrence (HR 0.26, 95% CI 1.06–1.50) in limited stage SCLC. Life table modelling estimated the 5 year survival in 65 year-old patients with early NSCLC who continued smoking to be 33%, compared with 70% for those who quit smoking. In limited stage SCLC, an estimated 29% of continuing smokers would survive for 5 years compared with 63% of quitters [81].
Improvement in quality of life after quitting in smokers with lung cancer
Quality of life and performance status improve in lung cancer after quitting smoking [82]. In 70 consecutive patients undergoing lobectomy or pneumonectomy for NSCLC, smoking at the time of surgery was associated with a poorer post-operative quality of life score. Cessation was associated with improved quality of life scores at any time point relative to lung cancer surgery [83].
A cohort study of over 1500 patients found that never- and former-smokers with lung cancer had a better tumour-specific quality of life score than smokers [84]. Smoking cessation in 200 people with NSCLC was associated with better performance status and quality of life [82].
Characteristics of smokers with lung cancer
Willingness to quit is particularly high immediately after a diagnosis of lung cancer is discussed with smokers. The importance of this “teachable moment” is reported in two large lung cancer screening trials [85, 86]. Despite high levels of nicotine dependence [85], smoking cessation rates in general cancer patients [87] and lung cancer patients [88] are comparable with “healthy” controls. For example, 40–53% of lung, and head and neck cancer patients were abstinent 6 months following treatment [89, 90].
Characteristics of lung cancer patients who continue to smoke
∼10–13% of people still smoke 6 months following a diagnosis of lung cancer [88–90]. Younger age, depression, and having a household member who smokes are factors that are associated with not quitting [91]. Smoking cessation treatments for patients with lung cancer are similar to those for patients with COPD and follow-up is often tied to other treatment visits and specific counselling designed to increase self-efficacy, and to reduce fatalistic thinking and emotional distress.
Therapeutic interventions in smokers with lung cancer
From the above evidence, healthcare professionals are aware that cessation is associated with longer survival and improved quality of life for smokers with lung cancer and they are usually alert to specific barriers to quitting.
Counselling
Whilst research into modified approaches for smokers with lung cancer continues, most Task Force members offer basic, short, directed advice:“One of the best things you can do to fight your lung cancer is to stop smoking. I can help you to stop smoking.”
Follow-up visits often coincide with other oncology visits, if possible, to reduce the onus on patients and specific information regarding treatment complications and survival benefits is supplied. Reducing fatalistic beliefs and addressing depression might also improve self-efficacy and self-esteem, especially if patients feel they have some control to contribute to one aspect of their forthcoming (often rigorous) treatments (table 5) [92].
Characteristics of counselling for smoking cessation in smokers with lung cancer
Pharmacological interventions
NRT, bupropion, and varenicline have all been used in smokers with lung cancer. There are no RCTs of bupropion in smokers with lung cancer compared with other groups [93]. A small pilot combining varenicline with smoking cessation counselling in patients with a diagnosed or suspected thoracic malignancy showed only half of 32 eligible participants completed the 12-week course, but biochemically validated 7-day, point prevalence abstinence rates were 34.4 versus 14.3% in the control group (OR 3.14, 95% CI 0.6–16.6; p=0.18). The authors concluded the programme was feasible, acceptable and probably effective as the lack of statistical significance was probably due to the very small sample size [94].
Table 6 shows the most relevant information from this section.
Summary of the relevant issues for smoking cessation in patients with lung cancer
Smoking cessation in smokers with asthma
The prevalence of smoking among people with asthma is similar to the general population, i.e. ∼20–25% [95, 96].
Benefits of smoking cessation in asthma
Continued smoking has detrimental effects on asthma. One population based, longitudinal study over 15 years reported that smokers with asthma had a greater decline in FEV1 than nonsmokers with asthma [97]. A meta-analysis of 10 controlled trials in people with asthma using ICS showed that smokers had a reduced benefit and an increased need for concomitant medications compared with nonsmokers [98]. A Canadian study of 893 persons with asthma found that smokers had poorer asthma control, made greater use of acute care and had higher absenteeism from work or school compared with their nonsmoking counterparts [99]. Stopping smoking is followed by better asthma control. One study found that after several weeks of quitting persons with asthma showed improved pulmonary function and a reduction in neutrophils in their sputum [100].
Smoking characteristics in patients with asthma
Analysis of 195 057 calls to quit-lines in 15 states in the USA from 2005 to 2008 showed that callers with asthma were less likely to quit compared with those without disease after a 7 month follow-up period [101]. Smokers with asthma are less likely to use appropriate methods to manage their asthma and are less likely to attend asthma education programmes compared with nonsmokers [102]. Some studies report that smokers with asthma develop nicotine dependence more quickly than smokers without asthma, which could explain fewer successful quit attempts [103].
Therapeutic interventions in patients with asthma
There are few studies of smoking cessation in patients with asthma. In an observational study of ever-smokers with asthma, the median time until quitting was 17 years [104]. A small interventional study of 32 smokers with asthma found 66% quit at 6 weeks but the longer term success was not reported [100]. A study of 57 smokers with asthma treated with NRT, bupropion and counselling found a 12-month quit rate of 28% [105].
The only RCT of smoking cessation in people with asthma randomised 220 smokers to: 1) smoking reduction (reducers); 2) complete smoking cessation (abstainers); or 3) continuation of usual smoking (continuing smokers). Subjects used nicotine chewing gum or an oral nicotine inhaler to promote reduction and cessation [106]. Cessation rates were 15% in both the cessation and reduction groups versus 3% in the control group. Asthma control and bronchial reactivity improved in quitters, but to a lesser extent in reducers [106].
Standard doses and duration of licensed pharmacotherapies with counselling are recommended [105, 106], but in clinical guidelines for treatment of asthma the importance of cessation is only briefly mentioned alongside the lack of smoking cessation trials specifically for asthma patients [107, 108].
The percentage of smokers with asthma that quit smoking can be used as a quality indicator for asthma clinics. As smokers with asthma may be several decades younger than smokers with COPD, cessation benefits will be larger in terms of quality-adjusted life years gained and so probably more cost-effective.
Table 7 shows a brief summary of the relevant issues from this section.
Summary of the relevant issues for smoking cessation in patients with asthma
Smoking cessation in patients with pulmonary TB
TB remains a global emergency killing 1.4 million people every year [109]. As smoking prevalence has risen in developing countries [110] more people with TB smoke now than ever [111].
Smoking prevalence in patients with TB
Smoking is more prevalent in people with TB compared with people without TB [112–123], with the risk of TB increasing in people who smoke more and who have smoked for more years. Meta-analyses suggest that smoking is an important risk factor for both pulmonary and extrapulmonary TB [124–126]. Moreover, TB is one of the “new” illnesses causally linked to smoking in the 2014 update of the US Surgeon General's Report [62].
Passive smoking and TB
A community survey of 1344 people showed that children who lived in a household with a patient with TB, were significantly and independently at increased risk of TB infection if they were exposed to passive smoking than if there was no added smoke in the house [127]. Cohort studies confirm this [128], with TB risk increasing with more tobacco smoke exposure [124, 129].
Effects of smoking on TB course and treatment
Longitudinal studies worldwide associate current smoking with worse TB outcome; it independently predicts positivity for acid-fast bacilli, delayed sputum conversion to negative cultures, longer duration of symptoms before diagnosis, prolonged infectivity, worse radiographic changes at presentation and longer time to recovery [130], chronic dyspnoea and fibrosis [131], and TB treatment failure and more deaths [120, 121, 131–138].
Mechanisms of how continued smoking leads to worse TB outcomes
Smoker's behaviour
Smokers with TB may present later because they interpret worsening cough or breathless as due to their smoking or delay seeking help because they do not want healthcare professionals to judge or address their smoking [121]. Smokers have been shown to be less compliant with TB medications than nonsmokers [139].
Biological mechanisms
Current smokers had a lower body mass index when diagnosed with TB [140] probably reflecting more advanced disease (see earlier), and certainly less physiological reserve. Nicotine reduces production of tumour necrosis factor-α by alveolar macrophages [126] rendering the patient more susceptible to progressive disease from latent infection. Tobacco smoke also reduces mucociliary clearance and the immune activity of a variety of cells [141].
Drug metabolism
Smokers show increased clearance of antimicrobial metabolites through induction of the cytochrome P450 enzymes. Serum rifampicin levels were lower in smokers compared with nonsmokers [142].
Smoking cessation in patients with TB
In a study from rural China, 55% of smokers reported stopping after a TB diagnosis but nearly one-fifth relapsed within 15 months [119]. Similar findings were reported from India [143] and Indonesia [144].
Barriers to smoking cessation in patients with TB
Focus group work suggests that patients diagnosed with TB were more receptive to advice to quit, but that they might start smoking again after recovery and some quit attempts were inhibited by exposure to smoking at TB facilities despite the presence of a “teachable moment” [145]. Healthcare professionals dealing with TB in developing nations sometimes advise patients with TB about smoking less [143, 144] and in one study only 5% believed they were sufficiently trained in smoking cessation techniques [146]. Furthermore, smoking cessation pharmacotherapy is less available and relatively expensive for use on a large scale in developing countries.
Benefits of quitting smoking and quit strategies in patients with TB
Training TB healthcare workers using DOTS (directly observed treatment, short-course) in Rio de Janeiro, Brazil to deliver smoking cessation for 1 day improved their self-rated efficacy but the effects on smoking rates were not reported [147].
Siddiqi et al. [148] performed a cluster RCT in 1955 adult smokers with suspected TB in Pakistan. Validated continuous smoking abstinence rates at 1 and 6 months were significantly higher with behavioural cessation support alone (41%) or with support combined with bupropion therapy (45%) compared with usual care (8.5%) [148]. Smokers with TB had greater improvements in quality of life over 6 months, when assigned to DOTS plus cessation support compared with DOTs alone [149].
Healthcare professionals provide a brief behavioural cessation intervention at diagnosis followed by monthly behavioural support throughout the TB treatment course and pharmacotherapy is offered wherever possible. The intervention and (self-reported) quit attempts may be recorded, e.g. on a modified TB treatment card [150].
Table 8 summarises the most relevant issues from this section.
Summary of the relevant issues for smoking cessation in patients with tuberculosis (TB)
Smoking cessation in smokers that find it difficult to quit
This section describes the therapeutic approach for smokers who are fully aware of the health risks and benefits of stopping smoking and who would like to become nonsmokers, but cannot overcome the barriers to quitting (loss of reward, withdrawal, discomfort, stress, weight gain, etc.).
These smokers are often offered a combination of counselling and pharmacological treatment. For those who have already received standard support and pharmacotherapy many Task Force members have found it helpful to change the style of the advice as well as its content. Being empathic, being understanding, and showing respect towards the patients' opinions regarding their smoking can make patients interested and attentive again [151]. Advice often focuses on reducing smoking rather than quitting abruptly. There are two possible benefits of smoking reduction. Most importantly, it can be a way to gradually achieve stopping smoking altogether [152]. The other possible benefit is to reduce the harm from smoking where complete cessation is not achieved. Although there is a strong relationship between cigarette consumption and the disease-risk, the reduction of risk associated with reduced smoking is not as clear. This is because unaided reduction may be accompanied by more vigorous puffing on the remaining cigarettes. For such a reduction to generate amelioration of risk or symptoms it probably has to be substantial (at least by 50%) and for an extended period of time [106, 153].
Three specific behavioural procedures have been proposed to aid smoking reduction by Hughes et al. [154]: 1) creating a hierarchy of the importance of each cigarette throughout an average day and start omitting those cigarettes either from the top (most needed) or from the bottom (least needed); 2) increasing the time interval between cigarettes; and 3) counting the number of cigarettes per day and making sure the number is within the quota allowed. The efficacy of these three alternatives appears uncertain and similar [154].
Both harm reduction and complete cessation using pharmacological support are much more promising. Standard doses of NRT [56, 152, 155] and varenicline [156] have helped reduction to quit (more than placebo), but bupropion doesn't seem as effective [155]. Different classes of pharmacotherapy are increasingly prescribed (off licence) in combination, in higher doses and for longer periods than normally recommended for those with particularly high addiction and/or ongoing withdrawal symptoms. Treatment with nicotine patches for 2 weeks prior to a predetermined quit date has also improved success for smokers who failed previous attempts to quit with NRT at standard doses [157–159]. For smokers who have failed in a previous attempt with varenicline, treatment may be prolonged for 24 weeks [155] or it may be started 4 weeks prior to the target quit date [160] to improve quit rates. A recent randomised clinical study has shown that the combination of varenicline with nicotine patches is more effective than varenicline alone [161], although a previous study did not show this [162]. Another study showed that the combination of varenicline with bupropion was more effective than varenicline alone at 6 months but not at 1 year of follow-up [163].
Figure 2 provides the reader with a therapeutic approach for smokers that find it difficult to quit.

{kind=link}
{kind=link}
The therapeutic approach used by most Task Force members for smokers that find it difficult to quit. NRT: nicotine replacement therapy; VRN: varenicline; BP: bupropion.
Conclusions
1) Like anyone else, smokers with COPD, lung cancer, asthma and TB are always advised to stop smoking. Healthcare professionals always make it clear that quitting smoking is the best thing these patients can do to improve their lung health. Smokers are usually offered a combination of counselling and pharmacological treatments.
2) Many patients remain unable to stop despite being aware of the specific link between their condition and smoking, and having a desire to stop. This suggests that they are highly dependent. They may face other barriers to successful smoking cessation compared with other smokers.
3) Using smoking cessation medications has been shown to be useful. NRT, bupropion and varenicline all have strong evidence of efficacy. A combination of two or more NRT products, higher than usual dosing, extended use prior to quitting and extended use post-quitting can improve treatment efficacy. Extended use of varenicline prior to and after the target quit date, and the combination of varenicline with nicotine patches or bupropion can improve treatment outcomes.
4) In smokers who are highly motivated to quit but are unable to do so, a harm reduction approach is often considered using varenicline and NRT at higher doses and for a more prolonged duration prior to quitting. In some patients, at least, such intervention can still facilitate successful cessation.
Footnotes
Conflict of interest: S. Masefield and P. Powell are employees of the European Lung Foundation. Other disclosures can be found alongside the online version of this article at erj.ersjournals.com
- Received May 20, 2014.
- Accepted December 24, 2014.
- Copyright ©ERS 2015
References











Jump To
- Article
- Abstract
- Abstract
- Methodology
- Introduction
- Smoking cessation in patients with COPD
- Smoking cessation in patients with lung cancer
- Smoking cessation in smokers with asthma
- Smoking cessation in patients with pulmonary TB
- Smoking cessation in smokers that find it difficult to quit
- Conclusions
- Footnotes
- References
- Figures & Data
- Info & Metrics