





Abstract
TKI should be used sequentially with chemotherapy and local procedures to prolong life in EGFR-mutated lung cancer http://ow.ly/KRWP4
To the Editor:
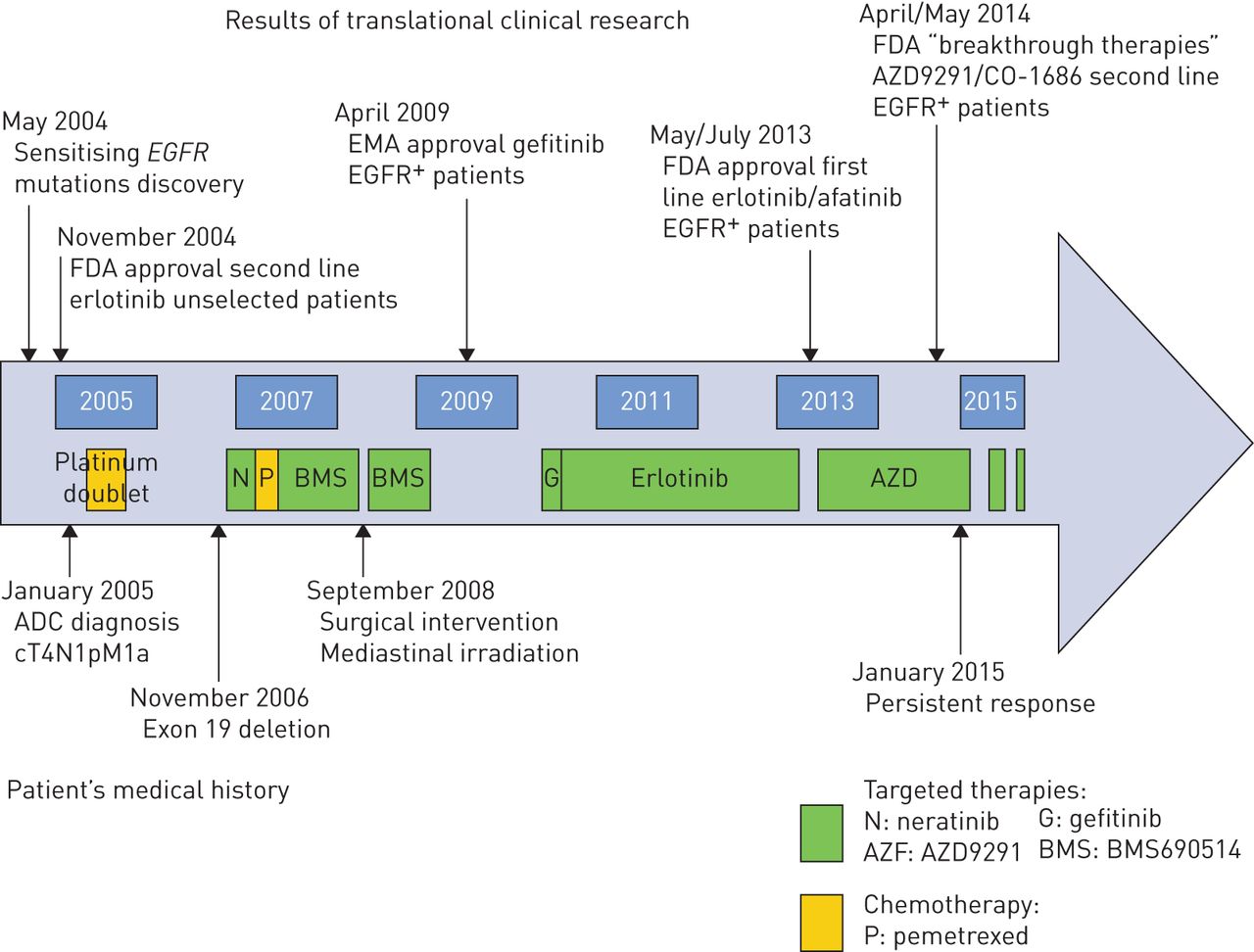
10 years ago, the US Food and Drug Administration approved erlotinib in the second and third line settings for unselected advanced nonsmall cell lung cancer (NSCLC) patients. Activating EGFR mutations were discovered by analysing patient subgroups who responded to oral, first-generation, single-target reversible EGFR tyrosine kinase inhibitor (TKI). Nine randomised phase III chemotherapy-controlled trials in EGFR-mutant NSCLC naive patients showed the superiority of gefitinib, erlotinib and afatinib, respectively, in terms of response rate and progression-free survival. Response rate is in the range of 70% and progression-free survival about 1 year. Exon 19 in-frame deletions represent about 45% of overall EGFR mutations and half of the sensitising ones [1]. New generation targeted therapies are currently under clinical development. However, treatment sequence is still debated after a first line of EGFR TKI regimen in these molecularly selected patients. We herein report a case of a metastatic EGFR-mutated lung adenocarcinoma patient who achieved a prolonged survival of 10 years through multiple surgical and medical treatments (fig. 1).
{kind=link}
Graphical view of medical history of the patient, according to translational clinical research advances. EMA: European Medicines Agency; FDA: US Food and Drug Administration; ADC: adenocarcinoma.
Our female patient was 60 years old when a chronic cough led to the diagnosis of a right lower lobe adenocarcinoma in January 2005. She had smoked five to six cigarillos per day from the age of 53 to 58 years, was treated for hypertension and had undergone a hysterectomy in 1999 for personal convenience. She presented an initial pericardial effusion with a positive cytology. The tumour was then classified as stage IV (cT4N1pM1a), according to the current seventh TNM classification. Thus, she was treated with a six-cycle platinum-based chemotherapy doublet. The tumour progressed in November 2006 and new biopsies revealed an E746 A750 deletion in exon 19 of the EGFR gene. Neratinib was then unsuccessfully administered for 3 months with grade 2 diarrhoea and grade 1 skin ulceration of the index finger. The tumour progressed through three cycles of pemetrexed. It was proposed that our patient join a phase 1 trial testing an oral signal-transduction inhibitor with both anti-angiogenic (VEGFR1−3 inhibition) and anti-HER functions (HER1, HER2, HER4): BMS690514 [2]. She presented grade 1 facial folliculitis, grade 2 diarrhoea and grade 3 hypertension, despite an association of angiotensin-converting enzyme inhibitor and thiazide diuretic. Therefore, the drug dose was decreased by 25%. BMS690514 was interrupted after 1 month because of a Tako-Tsubo cardiomyopathy and restarted with half a dose. After 15 months of treatment, the patient underwent an extended surgical procedure in a context of remarkable partial response. Tumour residues were found in mediastinal adenopathies which led to local irradiation. BMS690514 was discontinued after a 5-month adjuvant therapy. Interestingly, post-operative molecular analyses did not reveal any EGFR mutation but a chromosome 7 polysomy. 1 year later the tumour relapsed in all lung parenchyma. Gefitinib was unsuccessfully administered for 1 month and switched for a sixth line prescription of 85% full-dose erlotinib (because of grade 2 skin toxicity). The disease remained stable for 3 years in a context of manageable grade 2 skin toxicities and one resected skin basal cell carcinoma. In October 2013, the patient was enrolled on the AZD 9291 phase 1 trial testing this oral daily irreversible EGFR inhibitor. After 1 year, she still presents an excellent partial response with excellent physical condition and normal daily activities.
To our knowledge, this article presents the longest reported survival of a metastatic lung cancer patient with EGFR mutation. One Chinese female patient harbouring an EGFR-mutated metastatic lung cancer achieved an 8-year survival. She was treated with two alternated sequences of conventional chemotherapy and gefitinib [3]. Several published cases reported 3-year survival for metastatic lung cancer patients. All were treated with at least one EGFR TKI line [4]. Oncogenic addiction of EGFR-mutated NSCLC lung cancer is well-known: the timing of the first TKI administration does not impact the response rate, nor patients' overall survival [5]. In contrast to in vitro data, there is no clinical cross-resistance between platinum salts and EGFR TKI. However, the sequence of targeted therapies and conventional chemotherapy administration is still under debate after the first line. Mok et al. [6] recently reported that upon progression on gefitinib first line therapy, standard chemotherapy alone without continuation of gefitinib should be the preferred second line therapy.
Around 60% of patients progressing through first line EGFR TKI develop a resistance mutation such as T790M. Second generation EGFR TKIs, such as afatinib and dacomitinib, failed to overcome significant acquired resistance to erlotinib and gefitinib [7]. CO1686 and AZD9291 are third generation EGFR TKI which can irreversibly bind to EGFR sensitising mutations, as well as the acquired T790M mutation, with high selectivity as compared to wild-type EGFR [8]. Other resistance mechanisms can imply c-Met or HER2 amplification, phenotypic transformation into small cell cancer or epithelial–mesenchymal transition. 20% of resistance molecular mechanisms to EGFR TKI are still unknown. The present case is of value regarding EGFR inhibition. Our patient showed a primary resistance to neratinib, her initial EGFR TKI (a pan-HER inhibitor with indisputable activity in breast cancer). This failure is in line with the lack of activity of neratinib in classical EGFR sensitising mutations (i.e. exon 19 and exon 21 mutations). A phase II trial failed to confirm any clinical relevance of this second generation irreversible pan-HER inhibitor in lung cancer patients [9]. The patient was then exposed to BMS690514 compound. This is a pleiotropic signal transduction inhibitor with indisputable activity on EGFR sensitising mutations but on which development was halted after a randomised phase II trial versus erlotinib, which demonstrated similar efficacy read-outs but increased toxicity. Interestingly, the initial EGFR mutation was not found after surgery (Sanger sequencing). We introduced gefitinib in 2010 for three main reasons: 1) the tumour harboured an exon 19 EGFR deletion in 2006; 2) the lack of EGFR mutation on the 2008 surgical sample is probably related to the context of the concomitant excellent partial response (the EGFR clone was probably a minor clone at that time point); and 3) the patient had benefited from BMS690514, which is also an EGFR inhibitor. Upon relapse, the patient was exposed to gefitinib without success, but adequately controlled by erlotinib. The most likely explanations for the lack of efficacy of 250 mg gefitinib versus the clear activity with 100 mg erlotinib are as follows: 1) suboptimal plasma exposure with gefitinib [10, 11]; and 2) cross-resistance between EGFR TKIs. Indeed, three published cases report significant efficacy of erlotinib in gefitinib-resistant lung cancer [12–14]. Overall, through sequential EGFR inhibitors, our patient achieved three progression free survivals of more than 1 year in the fourth, sixth and seventh lines, respectively. The current efficacy of the AZD9291 third generation EGFR TKI in this case of is consistent with recently reported clinical results [15]. Finally, the very extended surgical procedure performed 3 years after the initial diagnosis must have been a key point in the long-term survival of our patient. Indeed, by reducing the tumour burden, the surgery may have allowed a decrease in the number of remaining EGFR resistance clones, thus delaying relapse and allowing a tumour-free interval of 2 years.
Despite the limitations of a case report, this long-term survival of an EGFR-mutated metastatic NSCLC patient provides an example of an optimal therapeutic sequence. Prospective clinical trials are accordingly warranted to validate such a sequential therapy and its timing.
Footnotes
Conflict of interest: Disclosures can be found alongside the online version of this article at erj.ersjournals.com
- Received January 30, 2015.
- Accepted March 9, 2015.
- Copyright ©ERS 2015
References










