





Figures
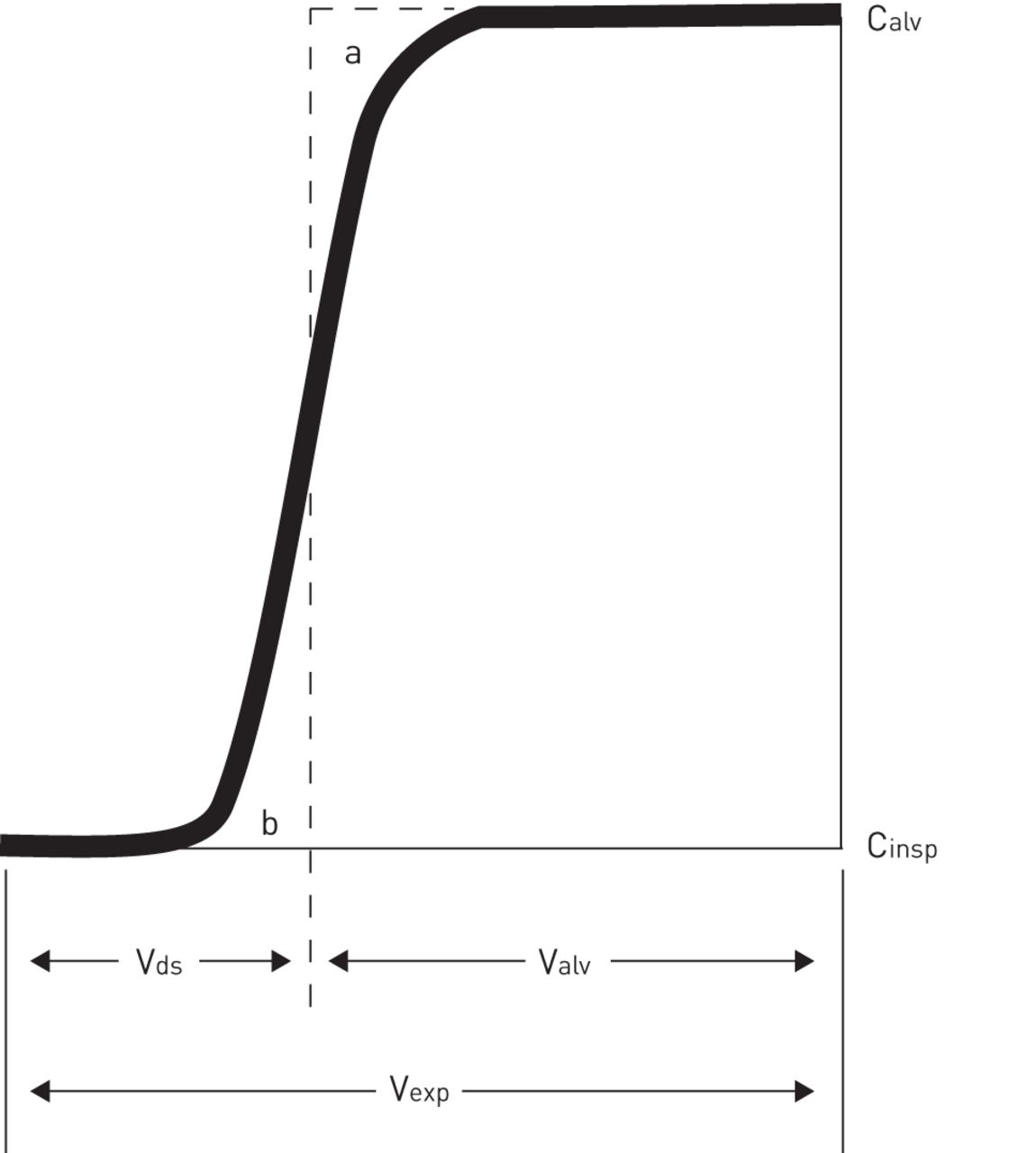
- FIGURE 1
Fowler’s illustration of the measurement of anatomical dead space, plotting exhaled concentration of nitrogen (C) following an inspired breath of 100% oxygen against exhaled volume (Vexp), where Cinsp represents the inspired nitrogen concentration (0%) and Calv represents the alveolar concentration of nitrogen. The vertical dashed line is positioned so that a and b subsume equal areas, and the intersection of the dashed line with the exhaled volume axis defines Vds, the anatomical dead space volume. Valv: alveolar volume. The original notation used by Fowler has been retained. Reproduced from [5] with permission from the publisher.
- FIGURE 2
Allocation of ventilation and blood flow in an abnormal lung that includes shunt, increased alveolar ventilation/perfusion ratio (V′A/Q′) heterogeneity and increased anatomical dead space. The lung has an overall V′A/Q′ of 1.0 and has the component lung units sorted according to their individual V′A/Q′ ratios. The broad base of the bell-shaped curve reflects substantial overall V′A/Q′ heterogeneity. The bar on the left represents the frequency of lung units compromising shunt, and the bar on the right represents lung units receiving ventilation but no pulmonary artery blood flow. Figure reproduced courtesy of R.W. Glenny (Division of Pulmonary and Critical Care Medicine, University of Washington, Seattle, WA, USA).
- FIGURE 3
Arterial (Pa) (retention) and alveolar (PA) (excretion) partial pressures for intravenously infused inert gases spanning a very large range of solubility in blood. The single solid curved line represents the arterial and alveolar curves of a perfectly homogenous lung (PaHOMO = PAHOMO), and the two dashed lines represent the influence of ventilation/perfusion heterogeneity that creates an arterial–alveolar partial pressure difference for both respiratory and inert gases. Pv: mixed venous partial pressure; λG: represents the solubility appropriate for CO2. #: solubility is expressed as mL of gas per mL of blood at 1 Atm. Reproduced from [19] with permission from the publisher.
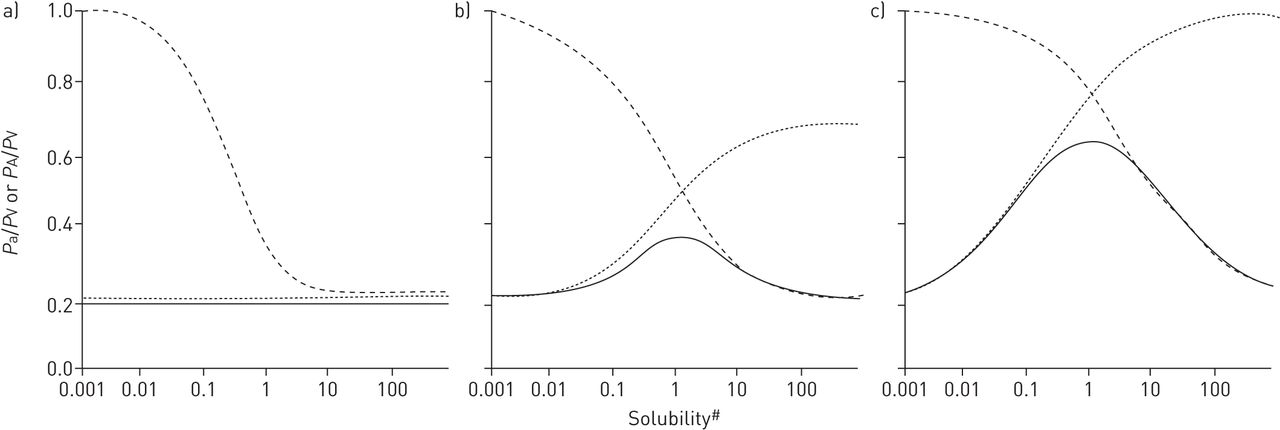
- FIGURE 4
Plots based on inert gas retention and excretion values for three model lungs that have 20% shunt and 20% anatomical dead space, illustrating the influence of a) no alveolar ventilation/perfusion ratio (V′A/Q′) heterogeneity, b) normal V′A/Q′ heterogeneity, and c) a high extent of V′A/Q′ heterogeneity. The dashed lines identify the physiological dead space calculation for the entire range of inert gas solubility. The solid lines represent the inert gas arterial–alveolar differences and the dotted lines represent the venous admixture calculation for the inert gases. #: solubility is expressed as mL of gas per mL of blood at 1 Atm. Reproduced from [19] with permission from the publisher.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
A simple two-compartment alveolar model containing a shunt compartment and a normal alveolar unit
Compartment 1 (shunt) Compartment 2 (ventilated) Combined output V′A 0.0 L·min−1 4.5 L·min−1 4.5 L·min−1 Q′ 1.5 L·min−1 3.0 L·min−1 4.5 L·min−1 V′A/Q′ 0.0 L·L−1 1.5 L·L−1 1.0 L·L−1 PaCO2 46 mmHg 37 mmHg 40 mmHg PACO2 46 mmHg 37 mmHg 37 mmHg Alveolar VD/VT 7.5% V′A: alveolar ventilation; Q′: perfusion; PaCO2: arterial CO2 tension; PACO2: alveolar CO2 tension; VD/VT: alveolar dead space.
- TABLE 2
A simple three-compartment alveolar model of V′A/Q′ heterogeneity
Compartment 1 (low V′A/Q′) Compartment 2 (normal V′A/Q′) Compartment 3 (high V′A/Q′) Combined output V′A 0.2 L·min−1 2.0 L·min−1 2.0 L·min−1 4.2 L·min−1 Q′ 2.0 L·min−1 2.0 L·min−1 0.2 L·min−1 4.2 L·min−1 V′A/Q′ 0.1 L·L−1 1 L·L−1 10 L·L−1 1 L·L−1 PaCO2 42 mmHg 40 mmHg 20 mmHg 40 mmHg PACO2 42 mmHg 40 mmHg 20 mmHg 29.6 mmHg Alveolar VD/VT 26% V′A: alveolar ventilation; Q′: perfusion; PaCO2: arterial CO2 tension; PACO2: alveolar CO2 tension; VD/VT: alveolar dead space.











Jump To
- Article
- Abstract
- Abstract
- Introduction
- Bohr dead space
- Fowler dead space
- Physiological dead space
- Shunt contribution to physiological dead space
- V′A/Q′ heterogeneity contribution to physiological dead space
- Physiological dead space in an abnormal lung
- Physiological dead space during exercise
- Can “true” alveolar dead space also exchange CO2?
- Interaction between anatomical dead space and V′A/Q′ heterogeneity
- Diffusion impairment and physiological dead space
- Dead space measurements in ARDS
- Factors contributing to the elevated VD/VT in ARDS
- Abnormal exercise dead space measurements in heart failure
- Abnormal exercise dead space measurements in pulmonary hypertension
- Summary and conclusion
- Footnotes
- References
- Figures & Data
- Info & Metrics