





Abstract
Cladribine treatment has marked efficacy for clinical, functional and imaging outcomes in a child with PCLH http://ow.ly/CK3XJ
To the Editor:
Langerhans’ cell histiocytosis (LCH) is a rare disease of unknown aetiology involving accumulation of Langerhans’ cells organised in granuloma, in various organs [1]. Pulmonary LCH (PLCH) is characterised by focal Langerhans’ cell granulomas infiltrating and destroying distal bronchioles, which results in cysts, major destruction of the pulmonary tissue and pneumothorax [2, 3]. PLCH is rare in children <18 years old.
When cysts are present, in children or adults, the disease is usually considered no longer active, and no treatment is effective for chronic cysts. The long-term outcome is marked by a slow progression to respiratory insufficiency and may be an indication for lung transplantation [4]. Recently, cladribine (2-chlorodeoxyadenosine), a synthetic chlorinated deoxyadenosine analogue, was found to be effective in adult patients with chronic cystic PCLH, with improvement in both lung function and computed tomography (CT) findings [5, 6].
We report the case of a child with cystic PLCH included in the French LCH registry (UPN 2106223; www.histiocytose.org), who showed marked improvement with cladribine monotherapy.
The initial history of this patient was remarkable, and was reported in 2009 [7], because the first symptom was abnormal movement of the trunk at age 20 months. LCH was diagnosed by liver and skin biopsy, and the initial workup concluded liver (sclerosing cholangitis) and skin involvement, associated with fever and inflammatory syndrome. The LCH was treated with vinblastine, steroids and 6-mercaptopurine for 15 months (in addition to ursodesoxycholic acid), with complete remission.
2 months after the end of therapy, reactivation of the disease was diagnosed by mediastinal node and lung involvement. The lung involvement was limited to a few cysts, and vinblastine and steroids were resumed for 11 months. The outcome was again favourable and the lung cysts disappeared. 2 months after the end of therapy, pituitary involvement, with diabetes insipidus followed by thyroid insufficiency, with pituitary thickening, was observed. Hormone replacement therapy was given but not LCH-specific therapy. 18 months later, the patient presented a new reactivation localised to the lung, with bilateral pneumothorax. In addition to surgical cure of the pneumothorax, vinblastine and 6-mercaptopurine were resumed for 12 months, with no change in CT findings or clinical stability.
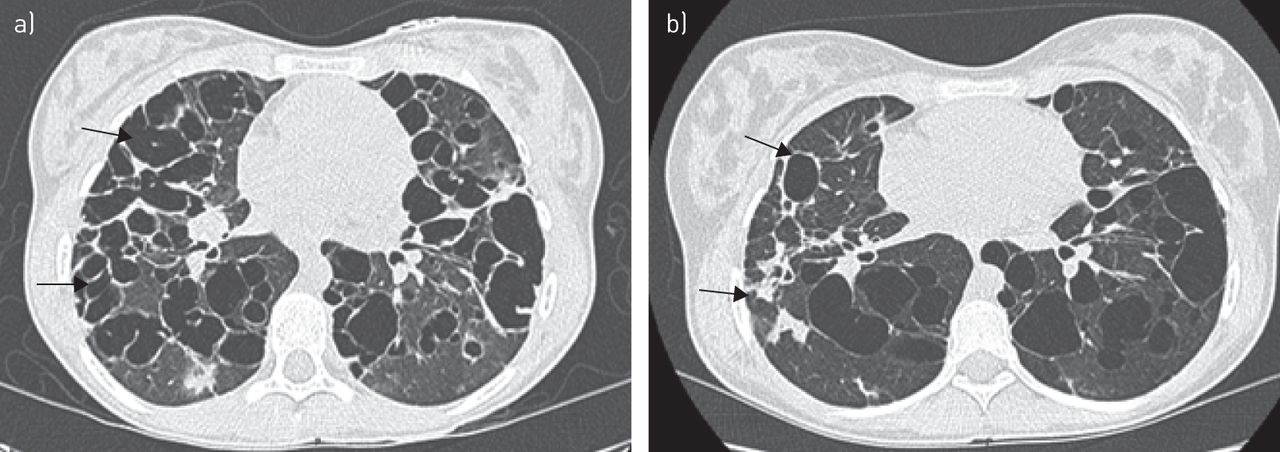
At 4 years and 9 months later, when the patient was 13 years old, reactivation of the disease was considered because she presented asthenia, weight loss (15% loss in 6 months) and inflammatory syndrome. The lung condition had worsened to stage III World Health Organization (WHO) functional class dyspnoea and lung function had deteriorated (forced vital capacity (FVC): 0.65 L, 27% of predicted; forced expiratory volume in 1 s (FEV1): 0.45 L, 22% of predicted; FEV1/FVC: 81%; and diffusing capacity of the lung for carbon monoxide: 1.05 mmol·min−1·kPa−1, 45% of predicted). On 6-min walk testing, the peripheral oxygen saturation decreased from 95% at rest to 89% after 330 m (40% of predicted). High-resolution CT of the lung showed extensive thick-walled cysts, together with mediastinal nodes (fig. 1a). An increased erythrocyte sedimentation rate, of 70 mm·h−1(normal value <20 mm·h−1), was associated with decreased albuminaemia, 30 g·L−1 (normal value >45 g·L−1).

{kind=link}
High-resolution computed tomography scans of the lung at the right inferior pulmonary vein in a child with primary Langerhans’ cell histiocytosis a) before treatment with cladribine and b) 18 months after treatment. Lung cysts decreased in size or resolved (arrows). Resolved cysts appear as residual irregular-shaped pseudomasses.
Because of the previous therapy with vinblastine (for ∼4 years in total) and its lack of efficacy for lung cysts, therapy with cladribine was considered. The patient received six courses of subcutaneous injections of cladribine at 5 mg·m−2 each for five consecutive days every 4 weeks (cumulative dose 150 mg·m−2) [1]. The treatment was well tolerated, with the exception of a febrile urticarial rash at the end of the therapy and 15 months later, an episode of genital infection due to herpes simplex virus type 2.
At 2 years and 6 months after the start of cladribine therapy, the dyspnoea had improved to WHO functional class II. High-resolution CT of the lung showed a decreased number of, or resolution of, thick-walled cysts, and the lung tissue initially containing these cysts had retracted. Resolved cysts appeared as residual irregular-shaped pseudomasses (fig. 1b). The cyst score (briefly, each lung was divided into three areas, from the lung apices to the domes of the diaphragm, and semi-quantitative CT scores were assigned to each area to estimate the extent of the cysts), from Tazi et al. [8], decreased from 22 in the pre-therapeutic evaluation to 18 at 2 years after therapy. FVC and FEV1 values increased by 53% (+0.58 L) and 55% (+0.40 L), respectively, as compared with pretreatment values. On 6-min walk testing, the peripheral oxygen saturation decreased from 97% at rest to 94% after 481 m (76% of predicted).
This case shows, for the first time, the marked efficacy of cladribine treatment for clinical, functional and imaging outcomes in a nonsmoking child with PCLH. In children, PCLH usually occurs as part of disseminated LCH (multifocal and systemic forms), with pulmonary involvement often not a prominent feature [9]. The pathogenesis of PLCH in childhood differs from that of adults, in that more than 95% of affected adults are cigarette smokers [3], and the pathology may reflect an uncontrolled immune response to an unknown stimulus or antigen.
Since the first publication reporting its use, in 1993 [10], cladribine has been used for several LCH patients [11, 12]. However, the main indication is refractory disease, mainly bone lesions, and not lung-cyst LCH. To date, the lung has not been considered a target organ for cladribine in children, especially in disease with diffuse cystic lesions. Although further studies are warranted to confirm our results, the present observation gives promise for the use of cladribine in children with PCLH.
Acknowledgements
The authors thank the patient and the family for their participation. The authors thank Abdellatif Tazi (Service de pneumologie, Hôpital Saint-Louis, Paris, France) for council.
Footnotes
This article has been revised according to the erratum published in the February 2016 issue of the European Respiratory Journal.
Support statement: The French Histiocytosis registry is supported by grants from the Institut de Veille Sanitaire and INSERM. This project received constant and unlimited support from the Association Histiocytose France, a grant from the association “la petite maison dans la prairie” and a grant from the RMHE. This report was based on research from the Centre de Reference des Histiocytoses and was supported by the Société d'Hémato Immunologie Pédiatrique and the Société Française des Cancers de l'Enfant.
Conflict of interest: None declared.
- Received August 9, 2014.
- Accepted September 22, 2014.
- Copyright ©ERS 2015
References










