





To the Editor:
Rhinovirus wheezing illnesses during early childhood are strongly linked with development of asthma later in life [1]. Indeed, rhinovirus infection in the first 3 years of life is associated with an almost 10-fold increase in risk for asthma at age 6 years [1]. The exact mechanism by which rhinovirus elicits a pro-asthmatic propensity in young children is largely unknown, but is purportedly related to a viral-induced T-helper cell (Th)2 airway inflammatory response [2]. Interestingly, the discovery of interactions between epithelial innate immunity and adaptive allergic responses has unveiled new potential links between rhinovirus and asthma. Of particular interest is the epithelial-derived cytokine thymic stromal lymphopoietin (TSLP), which is considered a “master Th2 cytokine” because it primes the differentiation of naïve T0 cells into Th2 lymphocytes via activation of antigen presenting cells [3]. TSLP is induced by rhinovirus infection or by exposure to double stranded (ds)RNA (viral surrogate) in the lungs of allergic mice [4], and in human bronchial epithelial cells (HBEC) [5]. Together, these data suggest that TSLP may be the missing link between innate antiviral epithelial immunity and the Th2 immune response characteristic of asthma.
This cross-sectional preliminary study aimed to investigate whether rhinovirus infections that occur naturally during the first 3 years of life are associated with elevated airway TSLP levels and enhanced Th2 responses, which may potentially facilitate the establishment of rhinovirus-induced pro-asthmatic changes during early childhood. We measured nasal airway TSLP, Th2 cytokines and antiviral responses in nasal washes obtained from newborns, infants and toddlers (≤3 years) with PCR-confirmed acute rhinovirus infection (n=71) relative to age-matched subjects without detectable virus using the PCR panel (n=54). Nasal airway secretions were collected from children aged ≤3 years seen in our medical centre (from February to December 2013) at the onset of acute respiratory illnesses by nasal saline lavage. The median (interquartile range) age of subjects was 0.58 (0.15–0.83) years in the control group and 0.99 (0.48–1.65) years in the rhinovirus group. There were no significant differences in the baseline demographic characteristics of the study groups, including ethnicity and sex. Nasal samples were analysed by a viral multiplex PCR kit (Luminex, TX, USA) for 14 targets used for clinical purposes in our institution according to the manufacturer’s recommended protocol. Nasal airway protein levels of TSLP, interleukin (IL)-4, IL-13, IL-12 (p70), and interferon (IFN)-γ were measured using a commercially available multiplex magnetic bead immunoassay (Millipore, MA, USA). Demographics and clinical information were obtained by electronic medical record review. This study was approved by the Institutional Review Board of the Children’s National Medical Center, Washington, DC, USA.
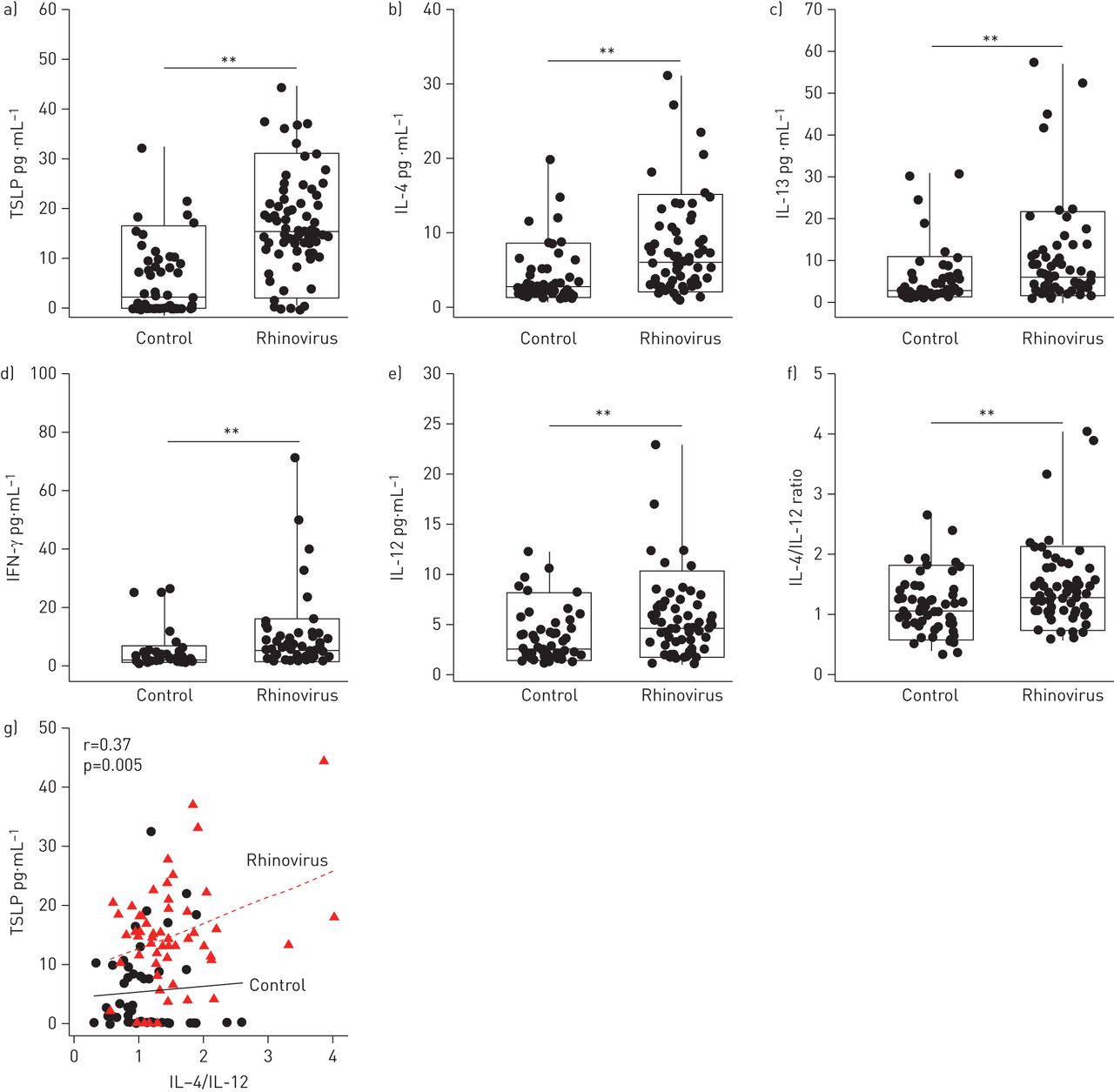
Our results identified that young children with rhinovirus infection had higher mean±se nasal TSLP levels compared with age-matched subjects without any identifiable virus (16.7±1.2 pg·mL−1 versus 5.5±0.9 pg·mL−1; p<0.01) (fig. 1a). Multivariate linear regression models identified that the association between rhinovirus infection and TSLP protein level (OR 8.25 (95% CI 5.02–11.48); p<0.001) was independent of sex, gestational age at birth and race/ethnicity. To explore if acute rhinovirus infection is also linked to enhanced nasal secretion of Th2 cytokines we measured protein levels of IL-4 and IL-13 in the same study subjects. Figures 1b and c show that young children with naturally occurring rhinovirus infection had elevated mean±se levels of classical Th2 cytokines compared with individuals without detectable virus (IL-4: 8.1±0.8 pg·mL−1 versus 4.1±0.5 pg·mL−1; and IL-13: 10.2±1.5 pg·mL−1 versus 5.3±SE 0.9 pg·mL−1). Although rhinovirus also elicited Th1 antiviral responses, as demonstrated by higher IL-12 and IFN-γ protein levels in rhinovirus-infected subjects relative to those with a negative viral PCR panel (mean±se IL-12: 5.6±0.5 pg·mL−1 versus 3.6±0.3 pg·mL−1; and IFN-γ: 8.3±1.5 pg·mL−1 versus 3.8±0.7 pg·mL−1; all p<0.05) (figs 1d and e), there was an overall predominance of Th2 cytokine production in the rhinovirus group according to Th2/Th1 cytokine ratio (IL-4/IL-12 ratio; 95% CI 1.28–1.63 in rhinovirus versus 95% CI 0.99–1.26 in control; p=0.004) (fig. 1f). Moreover, TSLP levels showed a moderate positive correlation with the Th2/Th1 cytokine ratio in rhinovirus-infected children (r=0.37; p<0.05; fig. 1g). Collectively, our results indicate that acute rhinovirus infection during early childhood is associated with an enhanced airway secretion of TSLP/Th2 cytokines that predominates over Th1 antiviral nasal cytokine responses.

{kind=link}
Nasal airway protein levels of a) thymic stromal lymphopoietin (TSLP), the T-helper cell (Th)2 cytokines b) interleukin (IL)-4 and c) IL-13, and the Th1 cytokines d) interferon (IFN)-γ and e) IL-12. f) Th2/Th1 cytokine ratio (IL-4/IL-12) in subjects with rhinovirus relative to control. Data are presented as boxplots (boxes represent the median and interquartile range, and whiskers represent the 10th–90th percentile) and p-values were obtained by two-sample t-tests. **: p<0.01. g) Moderate positive linear relationship between TSLP and Th2/Th1 cytokine ratio (IL-4/IL-12) in subjects with rhinovirus (r=Pearson correlation).
The nasal airway immune profile observed in young children infected with rhinovirus resembles what is seen in the lower airways of asthmatic individuals. Epithelial and sub-mucosal bronchial samples from adult asthmatic patients have enhanced TSLP mRNA expression, and bronchoalveolar lavage samples from these patients have higher concentrations of TSLP protein compared with those seen in healthy control subjects [6]. HBEC obtained from adult asthmatics exhibit a disproportionately high expression of TSLP relative to antiviral IFN-β responses after exposure to dsRNA (rhinovirus mimic) [7]. Human nasal epithelial cells also produce TSLP after dsRNA exposure [8], suggesting that they are the potential origin of nasal TSLP in our study. However, TSLP is secreted by nasal fibroblasts as well [9], thus the specific cellular source and corresponding signalling mechanism mediating nasal TSLP secretion during rhinovirus infection in early life is still unclear. Nonetheless, the presented findings suggest that rhinovirus might promote pro-asthmatic changes in early life via enhanced airway TSLP levels, which are known to orchestrate Th2 atopic responses in the asthmatic lung [3, 10, 11].
Our data also provides new evidence that viral respiratory illnesses in young children are associated with Th2 airway inflammation, which may explain why viruses such as rhinovirus elicit wheezing in early life, a clinical picture that resembles the asthmatic phenotype of older individuals [12, 13]. This has been suggested by a recent longitudinal study that reported that episodes of viral-induced wheeze in preschool children are characterised by enhanced airway inflammation (assessed by exhaled nitric oxide), reversible airflow limitation in spirometry, and asthma-related symptoms [14]. Our current preliminary work has not yet examined if the presence of elevated nasal TSLP and associated Th2 cytokines correlates with disease severity and/or predicts recurrence of the wheezing episodes. Nonetheless, recent reports suggest that the combination of a positive asthma predictive index with ongoing airway inflammation correlates with recurrent wheezing in young children [15]. This information highlights the importance of conducting future studies to investigate the potential role of airway pro-asthmatic biomarkers (i.e. TSLP and Th2 nasal cytokines) to better stratify viral-induced wheezing during preschool years and, thus, rationalise the use of asthma therapies in this age group.
In summary, our cross-sectional preliminary data indicate that acute rhinovirus infection in young children is associated with elevated nasal airway levels of TSLP/Th2 cytokines. This new information suggests that rhinovirus might shift immune responses towards Th2 in early life, which may facilitate the development of asthma during the first 3 years of life. However, given the cross-sectional design of our current study, we cannot prove a cause–effect relationship between rhinovirus infection, TSLP/Th2 responses and potential downstream effects resulting in pro-asthmatic effects later in life, thus, caution needs to be taken when interpreting the potential implications of these preliminary findings. Longitudinal studies are required to enhance our knowledge about the developmental aspects of TSLP biology and rhinovirus-induced Th2 airway inflammation, which might ultimately lead to novel strategies for the management of viral-induced wheezing and childhood asthma.
Footnotes
Support statement: This study was supported by NIH grants HL090020, HD001399 and the Board of Visitors (BOV) grant of Children’s National Medical Center.
Conflict of interest: None declared.
- Received March 13, 2014.
- Accepted May 12, 2014.
- ©ERS 2014
References










