





Abstract
Xpert MTB/RIF (Cepheid, Sunnyvale, CA, USA) is endorsed for the detection of pulmonary tuberculosis (TB). We performed a systematic review and meta-analysis to assess the accuracy of Xpert for the detection of extrapulmonary TB.
We searched multiple databases to October 15, 2013. We determined the accuracy of Xpert compared with culture and a composite reference standard (CRS). We grouped data by sample type and performed meta-analyses using a bivariate random-effects model. We assessed sources of heterogeneity using meta-regression for predefined covariates.
We identified 18 studies involving 4461 samples. Sample processing varied greatly among the studies. Xpert sensitivity differed substantially between sample types. In lymph node tissues or aspirates, Xpert pooled sensitivity was 83.1% (95% CI 71.4–90.7%) versus culture and 81.2% (95% CI 72.4–87.7%) versus CRS. In cerebrospinal fluid, Xpert pooled sensitivity was 80.5% (95% CI 59.0–92.2%) against culture and 62.8% (95% CI 47.7–75.8%) against CRS. In pleural fluid, pooled sensitivity was 46.4% (95% CI 26.3–67.8%) against culture and 21.4% (95% CI 8.8–33.9%) against CRS. Xpert pooled specificity was consistently >98.7% against CRS across different sample types.
Based on this systematic review, the World Health Organization now recommends Xpert over conventional tests for diagnosis of TB in lymph nodes and other tissues, and as the preferred initial test for diagnosis of TB meningitis.
Abstract
Xpert MTB/RIF can improve the diagnosis of lymph node TB and TB meningitis http://ow.ly/uFvjZ
Introduction
Worldwide, extrapulmonary tuberculosis (EPTB) accounts for ∼25% of all TB cases, and even higher percentages in HIV-infected individuals and children [1–3]. Existing tests for the diagnosis of EPTB are limited in accuracy and time to diagnosis, and often require invasive procedures and special expertise. For pleural TB, culture of pleural fluid has low sensitivity (on average, 30–50%). For lymph node TB, culture of an aspirate has a sensitivity of 60–70% [4]. Culture specificity is 100% if the presence of Mycobacterium tuberculosis complex is confirmed with antigen tests or nucleic acid amplification tests (NAATs). Often, biopsy with culture and histopathological examination is necessary to achieve a diagnosis. For TB meningitis, the yield of culture is even lower (on average, 30%), although repeat examination of the cerebrospinal fluid (CSF) or the use of NAATs may increase sensitivity and is associated with high specificity (>98%) [5, 6].
The Xpert MTB/RIF assay (hereafter referred to as Xpert; Cepheid, Sunnyvale, CA, USA) is a rapid, automated molecular test with high accuracy for pulmonary TB detection (sensitivity 89%, specificity 99%) [7]. While Xpert has been approved for TB detection in sputum by regulatory agencies, Xpert for TB detection in nonrespiratory specimens is considered “off-label” use [8–10]. However, given the limitations of available tests for EPTB detection, Xpert has been evaluated in several studies.
This systematic review, commissioned by the World Health Organization (WHO) to inform the recent update of the WHO policy on Xpert, aimed to assess the diagnostic accuracy of Xpert for TB detection in nonrespiratory samples in adults and children [11].
Methods
We developed a protocol before commencing the review, following standard guidelines [12, 13].
Search strategy
We searched MEDLINE, EMBASE, the Cochrane Infectious Diseases Group Specialized Register and Web of Knowledge for articles between the January 1, 2007 and October 15, 2013. We reviewed reference lists of all included articles. In addition, we assessed the metaRegister of Controlled Trials and the WHO Clinical Trials Registry Platform. We also attempted to contact all authors who had published abstracts on the topic at the American Thoracic Society Conference, the European Congress of Clinical Microbiology and Infectious Diseases and the Union World Conference on Lung Health (up to 2012), and other experts in the field of TB diagnostics to identify additional studies. No language restriction was applied. The key search terms used were: “Xpert”, “GeneXpert”, “Cepheid”, “tuberculosis” and “Mycobacterium tuberculosis” (further details are provided in the online supplementary material).
Inclusion criteria
We included full-text, peer-reviewed, cross-sectional studies, cohort studies, randomised controlled trials and case–control studies that used Xpert for detecting TB in nonrespiratory samples and compared it to a defined reference standard. We included studies on adults and children (aged <15 years) from all settings and countries with ≥10 nonrespiratory samples of predefined sample types (i.e. pleural fluid, lymph node aspirate or tissue, or CSF).
Reference standard
The reference standards were mycobacterial culture or a composite reference standard (CRS) defined by the study authors of the individual studies. The CRS might have included a NAAT (other than Xpert), histology, smear, biochemical testing results, presenting signs and symptoms or a response to treatment with anti-TB therapy in addition to culture (table 1).
Study selection and data extraction
Two review authors (C.M. Denkinger and S.G. Schumacher) independently assessed all articles for inclusion in the systematic review, and extracted data on study methodology, characteristics and test accuracy using a standardised extraction form (Tables 1 and 2; extraction form available in the online supplementary material). We extracted data on sample processing at the study level, although some steps (e.g. homogenisation) might apply to only certain sample types (e.g. tissue). We contacted authors when information was not reported in the paper. Any differences in the study selection and data extraction process between the two review authors were resolved by discussion with a third review author (K.R. Steingart).
Assessment of methodological quality
We grouped studies according to the type of reference standard (culture versus CRS) and assessed study quality separately for the two groups using QUADAS-2, a validated tool for diagnostic studies [32]. The QUADAS-2 protocol is available in the online supplementary material.
Statistical analysis and data synthesis
We performed descriptive analyses using STATA 12 (STATA Corporation, College Station, TX, USA). For each study, we calculated Xpert sensitivity and specificity along with 95% confidence intervals, compared with culture or CRS, and generated forest plots to display sensitivity and specificity estimates using Review Manager 5.2 (Nordic Cochrane Centre, Copenhagen, Denmark).
Imperfect reference standard
In diagnostic accuracy studies, an imperfect reference standard may lead to a misclassification of samples [33, 34]. Culture is an imperfect reference standard for EPTB due to the paucibacillary nature of the disease. Assuming that Xpert correctly identifies TB in a sample with a negative culture, the result would appear to be a false positive, leading to an underestimation of Xpert’s true specificity. A CRS that classifies TB based on a positive result of one out of several tests or clinical components may sometimes reclassify false positives of Xpert (identified as non-TB using culture) as true positives (TB cases) and thus lead to an increased (i.e. more accurate) estimate of Xpert specificity. However, a CRS itself may have reduced specificity that could result in apparent false-negative Xpert results, leading to an underestimation of Xpert’s true sensitivity [35, 36]. Therefore, a comparison of the accuracy estimates based on these two reference standards, culture and CRS, should provide a plausible range for sensitivity and specificity.
We excluded noninterpretable test results (i.e. invalid or erroneous results) from the analyses for determination of sensitivity and specificity [37].
Meta-analysis
We assessed heterogeneity in the forest plots (by visually examining the confidence intervals of individual studies) and in summary plots (by examining the width of the prediction region, with a wider prediction region suggesting more heterogeneity). We expected heterogeneity in terms of the sample types. Therefore, we pre-specified subgroups by sample type: pleural fluid, lymph node samples (tissue and aspirate combined; reporting in studies did not allow separating tissue samples from aspirates) and CSF. We used a bivariate random-effects model and carried out meta-analyses using the metandi command in STATA [38]. A meta-analysis for a predefined sample type was only carried out if at least four studies were available [39].
Several studies did not contribute to both sensitivity (no true positives or false negatives) and specificity, but only to specificity. In such cases, we performed a univariate random-effects meta-analysis of the specificity estimates separately, so as to make complete use of the available data. We compared the specificity estimate from the univariate analysis with that from a bivariate analysis of the subset of studies that provided both sensitivity and specificity.
Meta-regression
We anticipated additional heterogeneity with respect to sample processing methods, the condition of samples, laboratory level and HIV prevalence within the predefined subgroups. Therefore, we chose to use a bivariate meta-regression model (command: mvmeta) in STATA [40] under the assumption that the pooled sensitivity and specificity were different in each subgroup, but not the between-study variance–covariance matrix. We performed the meta-regression assessing only studies with a culture reference standard because the number of studies using CRS was limited. We also presumed that the effect of the covariate would not differ between the different reference standards. We focused on three categorical covariates (further subgroup analysis was not feasible because of the limited number of studies): concentration step (yes or no), condition of sample (fresh versus frozen) and HIV prevalence (>10 or ≤10%).
Sensitivity analysis
In addition, we performed two sensitivity analyses by limiting inclusion in the meta-analysis to: 1) studies in which patients were selected consecutively; or 2) studies that did not use a case–control design.
We chose not to carry out formal assessment of publication bias using methods such as funnel plots or regression tests because such techniques are not considered to be valid for diagnostic accuracy reviews [13]. The sponsors of the study had no role in study design, data collection, data analysis, data interpretation or writing of the report.
Results
We identified 18 studies (fig. 1) [14–31] that included 4461 samples. TB prevalence (based on culture) ranged from 0% to 81%. All studies were written in English. Eight (44%) studies were conducted in low/middle-income countries (table 1). Six studies did not include any HIV-positive patients and for two studies, HIV status was unknown [20, 32]. One study only included HIV-positive patients [30]. The percentages of HIV-positive patients included in remaining studies ranged from 1% to 87% of the study population (table 1). 10 studies included children, with percentages ranging from 2% to 34%.

Flow diagram of studies in the review. EPTB: extrapulmonary tuberculosis.
The median number of samples per study was 137 (interquartile range 67–342). Seven studies included only one sample type (e.g. pleural fluid only) [17, 18, 21, 25, 26, 30, 39] (table 1). The remainder of the studies included different sample types in varying percentages. Six studies used archived frozen samples, 11 used fresh samples, and one used both fresh and frozen samples (table 2).
With respect to specimen processing, the studies varied widely (table 2). Only four (25%) studies used the protocol (i.e. volume of sample included and sample reagent to sample ratio) recommended by the manufacturer [36] for unprocessed sputum samples [17, 19, 29, 25] (table 2). Most of the studies that included a mechanical homogenisation step (40%) also performed a decontamination procedure with N-acetyl-l-cysteine and sodium hydroxide solution. 11 (55%) studies reported a concentration step (table 2). The sample reagent/sample volume ratio also varied. Five (25%) studies used a ratio of 3/1, while the remainder of studies used 2/1. Of the eight studies that used a digestion/decontamination step, four studies used a ratio of 2/1 (table 2).
Methodological quality of studies
The overall methodological quality of the included studies using a culture reference standard is summarised in figure 2 (additional information on the quality assessment for each study individually and using a culture reference standard is given in the online supplementary material). The majority of studies collected data prospectively (n=14; 78%) (table 1) and only three studies used a case–control design [15, 23, 26]. All studies were performed either in tertiary care centres or reference laboratories.

a) Risk of bias and b) applicability concerns as percentages across the included studies using a culture-based reference standard for tuberculosis detection.
We considered that differences in sample processing might affect estimates of the diagnostic accuracy of Xpert to varying degrees (table 2). In particular, we were concerned that the mechanical homogenisation step could be a source of variation in test accuracy (n=8, 40%) for two reasons: procedural differences might affect the quantity of sample particles in the sample volume and the particles could clog the cartridge valves leading to noninterpretable results. We also considered the possibility that the reference standard could introduce bias due to misclassification of participants (fig. 2) [34, 35].
Detection of EPTB
Studies were very heterogeneous, particularly among smear-negative samples; therefore, combining studies to obtain accuracy estimates of Xpert for EPTB (all forms combined) was not considered to be meaningful. For smear-positive samples (506 samples), a univariate analysis yielded a sensitivity of 97.4% (95% CI 95.5–99.3%) across sample types. Data were too limited to estimate specificity.
We focused the remainder of the analysis on predefined subgroups of sample types (i.e. pleural fluid, lymph node aspirate or tissue, and CSF) to account for the heterogeneity. Data for smear status of samples were not available for the individual sample types. Therefore, samples included in the subgroups may be smear-positive, negative or unknown.
Detection of lymph node TB
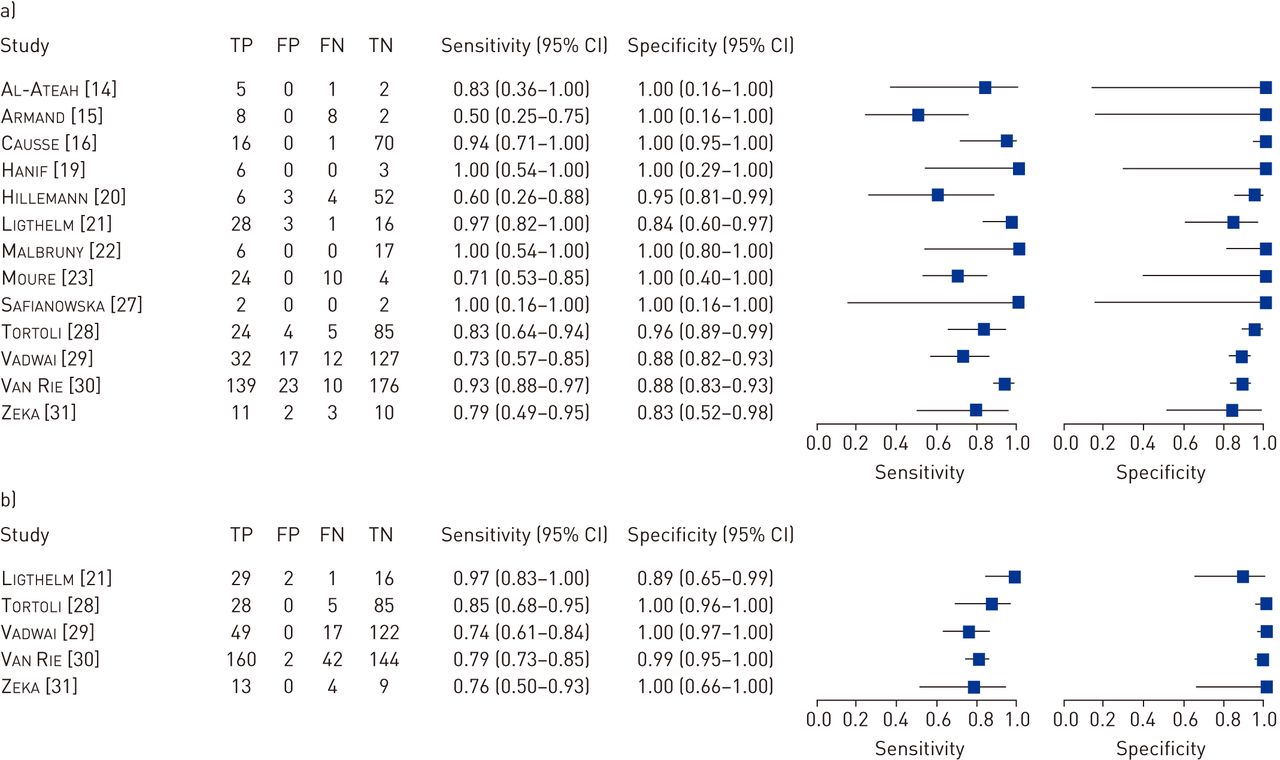
For studies [14–16, 19–23, 27–31] that evaluated lymph node biopsy or fine-needle aspirate using a culture reference standard (13 total, 10 with >10 samples; 955 samples, 362 culture-positive), Xpert sensitivity ranged from 50% to 100% (fig. 3a). Pooled sensitivity across studies was 83.1% (95% CI 71.4–90.7%) and pooled specificity was 93.6% (95% CI 87.9–96.8%). Only two studies reported any noninterpretable results for Xpert: 1.4% (five out of 353) and 10% (two out of 20) [15, 30].
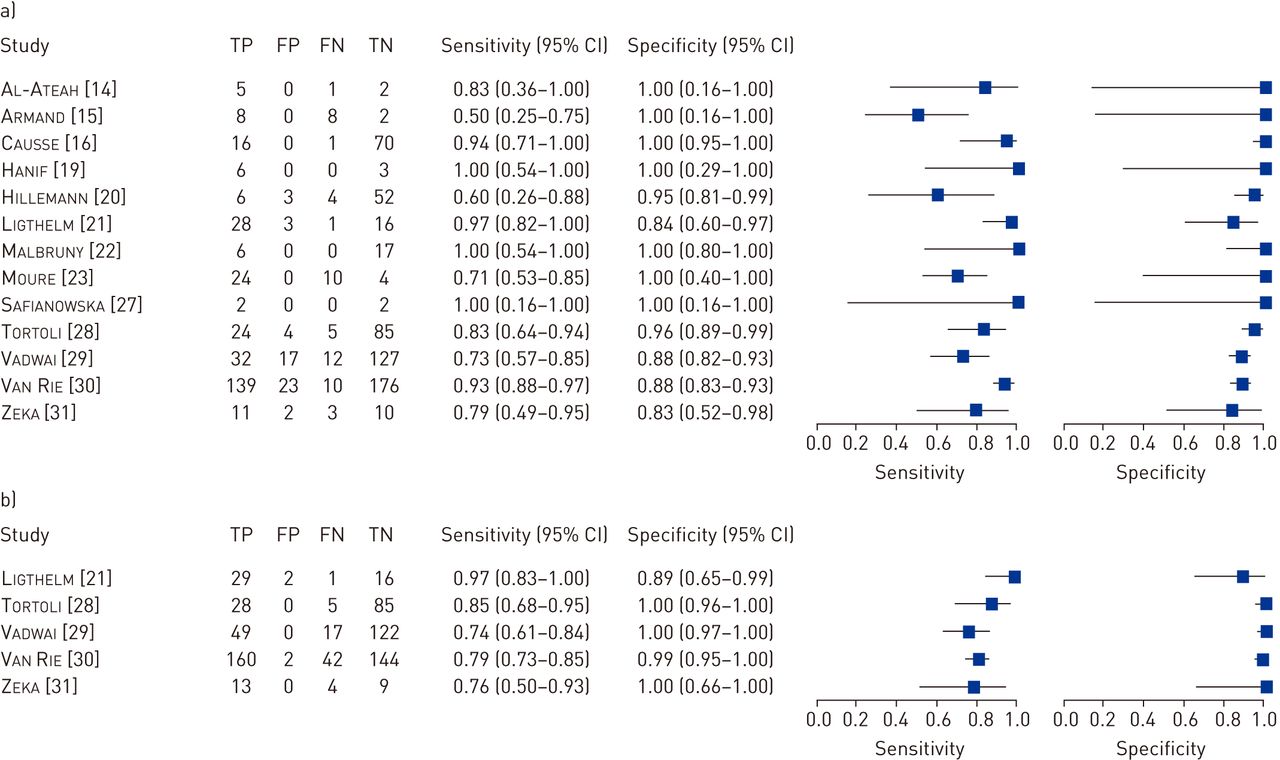
Forest plot of Xpert sensitivity and specificity for tuberculosis detection in lymph node samples (tissue or aspirate) with a) culture reference standard and b) composite reference standard. The squares represent the sensitivity and specificity of one study, the black line its confidence interval. TP: true positive; FP: false positive; FN: false negative; TN: true negative.
Five studies [21, 28, 29–31] assessed Xpert in lymph node samples against a CRS (fig. 3b). Pooled sensitivity was 81.2% (95% CI 72.4–87.7%). As expected, the specificity was improved, at 99.1% (95% CI 94.5–99.9%), in comparison to the culture reference standard.
Studies that used fresh samples showed a higher sensitivity (86.4%, 95% CI 75.7–97.1%) than those that used frozen samples (74.0%, 95% CI 56.5–91.5%); however, the precision of these estimates was low as data were limited. Only three studies included >10% HIV-positive patients. Accuracy estimates did not differ substantially between these studies and others that included <10% HIV patients.
Detection of pleural TB
14 studies [14–20, 22, 23, 26–29, 31] (841 samples in total, 92 culture positive) evaluated Xpert in pleural fluid versus culture. Xpert sensitivity varied widely (0–100%) (fig. 4a). The outliers at the lower and upper ends of the range were studies with few culture-confirmed TB cases. The pooled sensitivity was 46.4% (95% CI 26.3–67.8%) and the pooled specificity was 99.1% (95% CI 95.2–99.8%).

Forest plot of Xpert sensitivity and specificity for tuberculosis detection in pleural fluid with a) culture reference standard and b) composite reference standard. The squares represent the sensitivity and specificity of one study, the black line its confidence interval. TP: true positive; FP: false positive; FN: false negative; TN: true negative.
In comparison with the bivariate analysis, a univariate analysis for specificity achieved a similar estimate (98.9%) with a slightly narrower confidence interval (97.9–99.8%). One study reported noninterpretable results for Xpert: 5.4% (six out of 111) [20].
Six studies (598 samples) [17, 18, 26, 28, 29, 31] evaluated Xpert in pleural fluid versus CRS. Only a univariate analysis was feasible given the limited data. Compared with the pooled estimate with culture as the reference standard, the CRS subgroup yielded a lower sensitivity (21.4%, 95% CI 8.8–33.9%) with a slightly higher specificity of 100% (95% CI 99.4–100%) (fig. 4b).
Sensitivity was increased in studies with a low rate of HIV co-infection (49.5% compared with 40.6% in studies with >10% HIV) and in studies that used a concentration step (49.1% compared with 41.6% without concentration step). A higher sensitivity was also observed for fresh samples (59.0%, 95% CI 41.0–76.9%) compared with frozen samples (31.4%, 95% CI 18.9–43.9%); however, the estimates for all of these subgroup analyses were imprecise and the confidence intervals were wide and overlapping.
Detection of TB meningitis
13 studies (839 samples; 10 with >10 samples, 159 culture positive) evaluated Xpert in CSF against culture [14–16, 19, 20, 22–25, 27–29, 31]. Sensitivity varied widely (51–100%), with the study by Vadwai et al. [29] (sensitivity none out of 196 samples, three false negatives) considered an outlier (fig. 5a). Pooled sensitivity was 80.5% (95% CI 59.0–92.2%) and pooled specificity was 97.8% (95% CI 95.2–99.0%). Noninterpretable results for Xpert were reported in three studies, with only one study [28] having >2% (i.e. 3.6%).

Forest plot of Xpert sensitivity and specificity for tuberculosis detection in cerebrospinal fluid with a) culture reference standard and b) composite reference standard. The squares represent the sensitivity and specificity of one study, the black line its confidence interval. TP: true positive; FP: false positive; FN: false negative; TN: true negative.
Five studies (711 samples) that assessed Xpert in CSF samples versus a CRS found variable sensitivity (20–86%) (fig. 5b) [24, 25, 28–29, 31]. Pooled sensitivity was 62.8% (95% CI 47.7–75.8%) and pooled specificity was 98.8 (95% CI 95.7–100%).
Prevalence of HIV and the condition of the specimen did not have an effect on Xpert sensitivity and specificity in CSF. However, a concentration step in the processing of the sample (table 2) appeared to enhance the sensitivity of Xpert (84.2% (95% CI 78.3–90.1%) versus 51.3% (95% CI 35.5–67.1%) for unconcentrated samples; specificity 98.0% (95% CI 96.7–99.2%) versus 94.6% (95% CI 90.9–98.2%) for unconcentrated samples).
Sensitivity analyses across all samples types did not substantially affect the results (online supplementary material).
Discussion
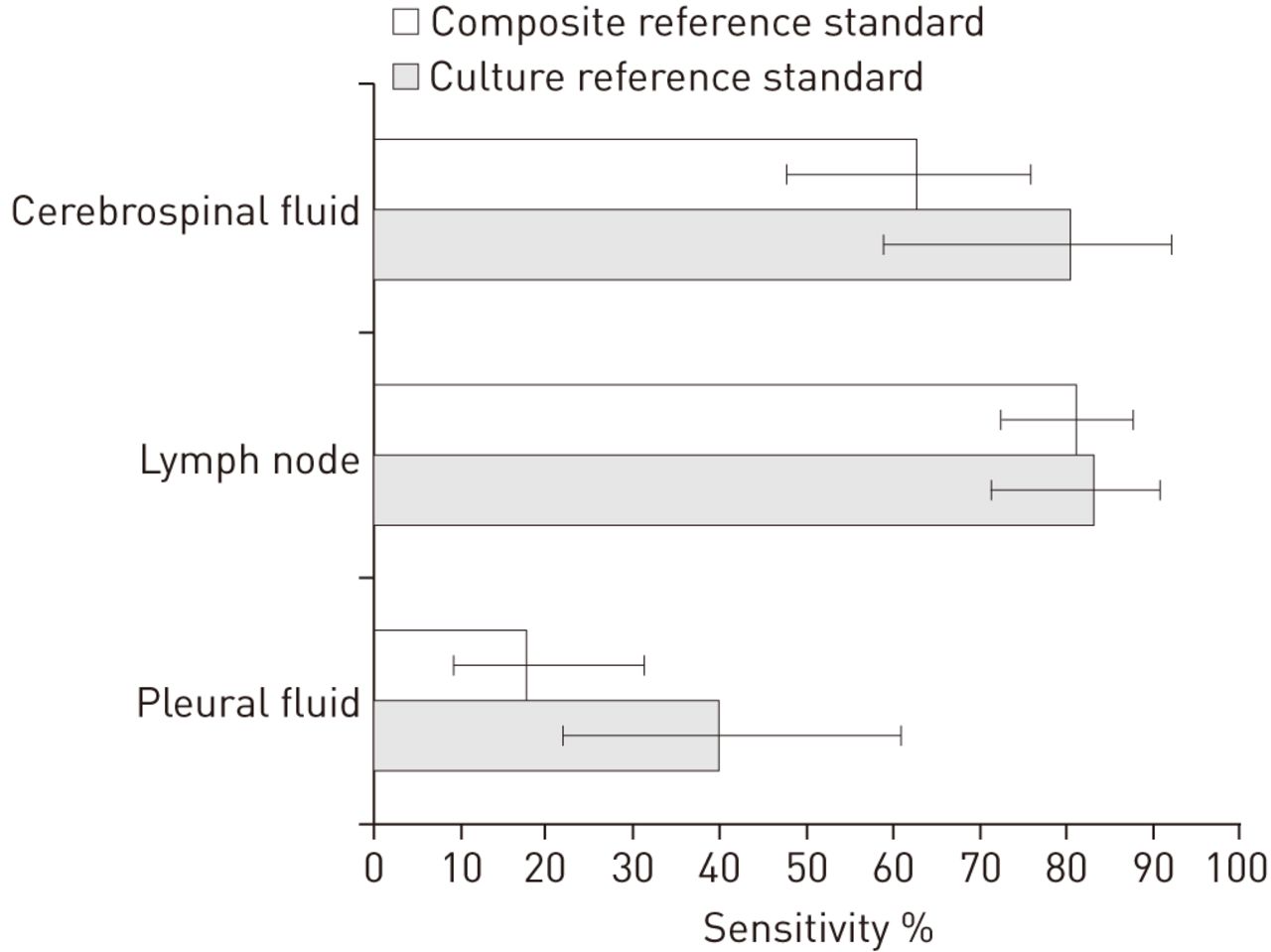
Our systematic review demonstrated that Xpert sensitivity for TB detection in nonrespiratory samples varied widely across different sample types. While Xpert is a highly sensitive diagnostic for TB detection in lymph node samples and moderately sensitive for the detection of TB meningitis, our results show lower sensitivity for testing pleural fluid. Figure 6 shows the pooled sensitivity estimates for different sample types (pooled specificity estimates are online supplementary material).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pooled sensitivity estimates across sample types.
The high sensitivity (97.4%, 95% CI 95.5–99.3%) of Xpert in smear-positive samples across sample types and the low proportion of noninterpretable results (1.2%) support the use of the test in nonrespiratory samples in principle. The poor sensitivity of Xpert in pleural fluid is probably due to the paucibacillary nature of the disease and the fact that not pleural fluid but rather pleural biopsy is the sample of choice for the diagnosis of pleural TB (as has been described for culture) [41]. The presence of PCR inhibitors, either in the pleural fluid itself or from blood contamination of the sample, could be considered as well [42, 43]. Where resources are available, Xpert on pleural fluid could still be considered in the work-up of pleural TB as it has higher sensitivity than smear and provides a more rapid diagnosis than culture and histology.
Prior data have suggested a potential role for NAATs in the diagnosis of TB from CSF and lymph node samples, and the results for Xpert here confirm these findings [4, 6]. Interestingly, we observed that a concentration step for CSF increases Xpert sensitivity with unchanged specificity, probably by increasing the bacillary load in the cartridge input volume. While Xpert does not reach the sensitivity of culture, it could improve the diagnosis of CSF and lymph node TB in places where culture or other diagnostic tests are not available or where a rapid diagnosis of TB is necessary (as might be the case for TB meningitis).
The combined confidence intervals for sensitivity and specificity of Xpert versus culture and CRS (which includes culture) provide a range in which the “true” sensitivity and specificity are likely to fall. Future analyses could employ statistical models, such as latent class models, that incorporate knowledge about the imperfect accuracy of reference standards to provide a single plausible estimate for the accuracy of Xpert [36].
Strengths of our review include the use of a standard protocol, strict inclusion criteria, standardised data extraction, independent reviewers, a bivariate random-effects model for meta-analysis and pre-specified subgroups to account for heterogeneity. This data set involved comprehensive searching to identify studies as well as repeated correspondence with study authors to obtain additional data on the studies.
Our review also had several limitations. We acknowledge that we may have missed some studies despite the comprehensive search. In addition, the meta-analysis was limited by the small number of studies for the different sample types, particularly those using a CRS. In addition, low event rates (i.e. confirmed TB cases) limited the precision of our sensitivity estimates. Furthermore, sample processing was highly variable across and within studies, as there was no recommendation available on how to process nonrespiratory samples from the manufacturer or the WHO. Also, the CRS differed between studies. Because of this heterogeneity, the pooled estimates must be interpreted with caution.
The pooled sensitivity and specificity estimates in our meta-analysis might be overly optimistic for at least three reasons. First, the quality of some studies might have suffered from a lack of a representative patient spectrum (e.g. studies using convenience sampling). Second, all of the studies were performed in tertiary care centres or reference laboratories. Third, publication bias must to be considered [44]. However, 44% of studies were performed in low-prevalence settings. It is likely that patients in these settings present earlier with more paucibacillary disease, which might result in a decreased sensitivity of Xpert [45].
Given the limited data for the sample types and the large variation in sample processing, a detailed investigation of the best sample processing was not possible in this review. An optimised processing procedure might also need to be different for different sample types and might further improve Xpert performance. We therefore would encourage studies to focus on optimisation of sample preparation. Furthermore, additional research is needed on the diagnostic accuracy of Xpert on samples other than those assessed in this review (e.g. blood), and on the impact on patient-important outcomes.
Our review findings have informed an updated WHO policy on Xpert for EPTB [11]. WHO now recommends Xpert over conventional tests for the diagnosis of TB in lymph nodes and other tissues, and as the preferred initial test for the diagnosis of TB meningitis. A draft technical advisory document on the standard operating procedure for sample processing is now available from the WHO [46].
Acknowledgments
We wish to thank the following individuals for their contributions to this project: Vittoria Lutje (Liverpool School of Tropical Medicine, Liverpool, UK) and Matteo Zignol (WHO, Geneva, Switzerland), and all the authors of the studies analysed.
Footnotes
This article has supplementary material available from erj.ersjournals.com
Support statement: Development and publication of this manuscript was made possible with financial support from the US Agency for International Development. M. Pai is supported by the European and Developing Countries Clinical Trials Partnership (EDCTP-TBNEAT grant) and the Fonds de recherche du Québec – Santé (FRQS). N. Dendukuri is supported by a Chercheur Boursier salary award from the FRSQ. C.M. Denkinger is supported by a Richard Tomlinson Fellowship at McGill University and a fellowship of the Burroughs–Wellcome Fund from the American Society of Tropical Medicine and Hygiene. S.G. Schumacher is supported by the Quebec Respiratory Health Training Program. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflict of interest: Disclosures can be found alongside the online version of this article at erj.ersjournals.com
- Received January 9, 2014.
- Accepted March 8, 2014.
- ©ERS 2014
References










