





Figures
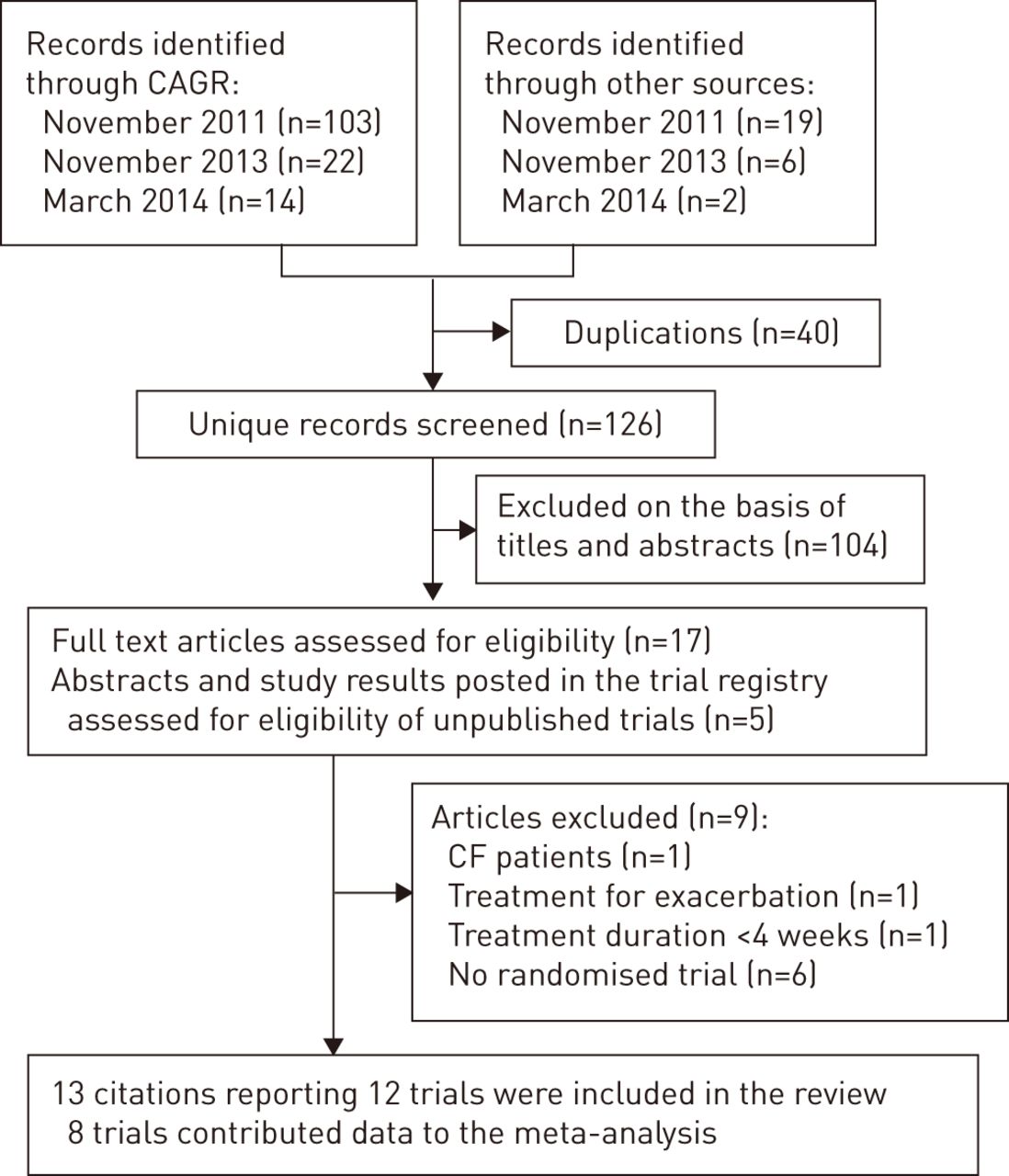
- Figure 1–
Flow diagram of study selection. CAGR: Cochrane Airways Group Register of Trials.
- Figure 2–
Effects of inhaled antibiotics on reduction of sputum bacterial load (log10 CFU·g−1). WMD: weighted mean difference; PA: Pseudomonas aeruginosa.
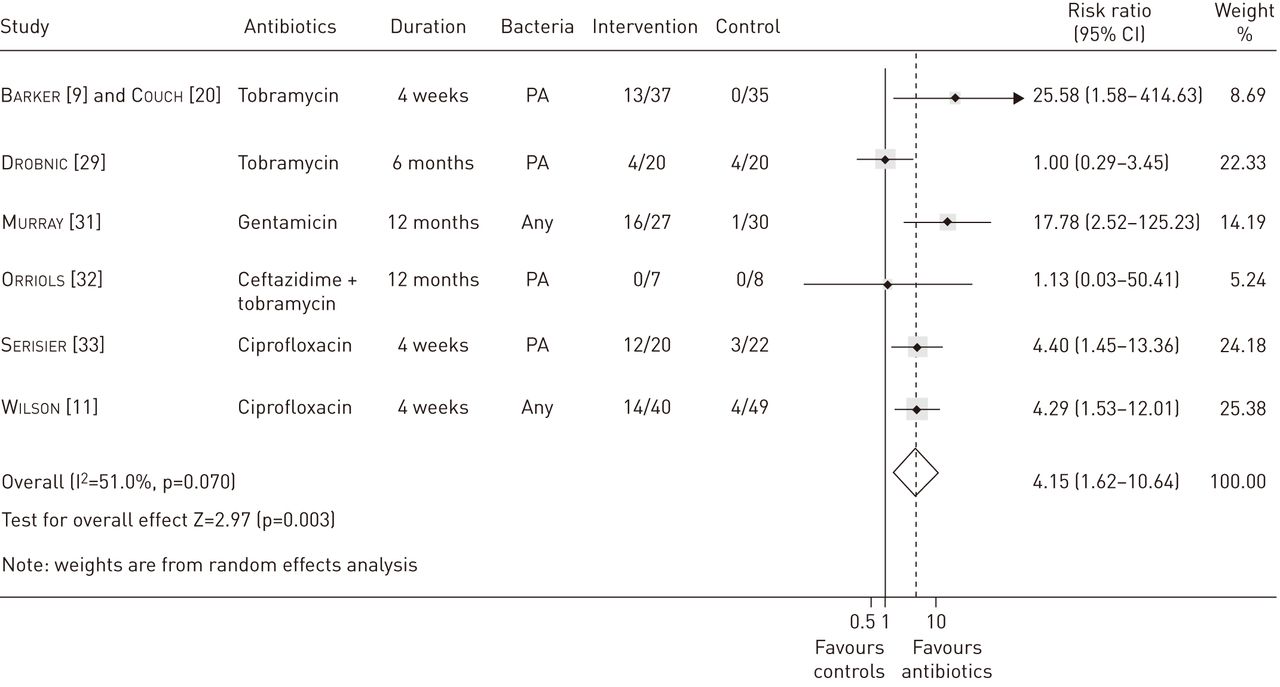
- Figure 3–
Effects of inhaled antibiotics on bacterial eradication from sputum. PA: Pseudomonas aeruginosa.


{kind=link}
{kind=link}
{kind=link}
Tables
- Table 1– Characteristics of included trials
Study Country Participants Intervention Control Study design Outcomes AIR-BX1 and AIR-BX2 trials 2013, sponsored by Gilead Sciences [21, 22, 23] Belgium, France, Germany, Italy, the Netherlands, Spain, UK, USA Inclusion criteria: adult patients (≥18 years) had non-CF bronchiectasis confirmed by HRCT, and had positive sputum culture for Gram-negative organisms Exclusion criteria: patients had hospitalisation within 14 days prior to the study, previous exposure to inhaled aztreonam, continuous O2 use >2 L·min−1, current treatment for non-TB mycobacterial infection or active TB infection within 1 year of enrolment or other serious medical conditions Aztreonam 75 mg via an eFlow nebuliser, three times a day, two 28-day on/off cycles AIR-BX1 (n=134) AIR-BX2 (n=136) Placebo via an eFlow nebuliser, three times a day, two 28-day on/off cycles 00AIR-BX1 (n=132) AIR-BX2 (n=138) International, multicentre, RDBPCT Primary: mean change in QoL-B scores from baseline to day 28 Secondary: mean change in QoL-B scores from baseline to day 84, time to first exacerbation Barker 2000 and Couch 2001, sponsored by PathoGenesis [9, 20] USA Inclusion criteria: adult patients (≥18 years) had bronchiectasis diagnosed by CT, and had grossly purulent sputum containing PA ≥104 CFU·g−1 Exclusion criteria: patients had CF, ABPA, acute pulmonary process requiring medical intervention, or had received antibiotics within 2 weeks prior to the study Tobramycin 300 mg via a jet nebuliser, twice daily, 4 weeks (n=37) Placebo (1.25 mg quinine sulfate) via a jet nebuliser, twice daily, 4 weeks (n=37) Multicentre, RDBPCT Primary: mean change in sputum PA density (log10 CFU·g−1) from baseline to week 4 Secondary: eradication of PA in sputum, clinical improvement, hospitalisation, PFT, adverse events, emergency of bacterial resistance Drobnic 2005, no sponsor [29] Spain Inclusion criteria: adult patients had bronchiectasis diagnosed by HRCT, and had ≥3 positive sputum cultures for PA during the 6 months before the study Exclusion criteria: patients had CF, tobramycin hypersensitivity, PA in sputum resistant to tobramycin, or had serum creatinine ≥1.5 mg·dL−1 Tobramycin 300 mg via a jet nebuliser, twice daily, 6 months (n=30) Placebo (0.9% saline) via a jet nebuliser, twice daily, 6 months (n=30) Crossover RDBPCT, with a one-month washout period Primary: number of exacerbations and hospitalisations Secondary: mean change in sputum PA density, eradication of PA in sputum, use of antibiotic, PFT, markers of systemic inflammation, SGRQ, adverse events, emergence of bacterial resistance Haworth 2014, sponsored by Profile Pharma Ltd [30] Russia, Ukraine, UK Inclusion criteria: adult patients (≥18 years) had clinically stable, non-CF bronchiectasis conformed by CT, had ≥2 positive sputum cultures for PA in the preceding 12 months and a positive sputum culture for PA at the screening visit Exclusion criteria: not stated Colistin 1 million IU via I-neb AAD system, twice daily, 6 months (n=73) Placebo (0.45% saline) via I-neb AAD system, twice daily, 6 months (n=71) Multicentre RDBPCT Primary: time to first exacerbation Secondary: severity of exacerbation, mean change in sputum PA density (log10 CFU·g−1), SGRQ, adverse events, emergence of bacterial resistance Murray 2011, supported by the Chief Scientist Office, Scotland [31] UK Inclusion criteria: adult patients had clinically stable bronchiectasis diagnosed by HRCT, had chronically infected sputum, had ≥2 exacerbations in the past year, and had FEV1 >30% predicted Exclusion criteria: patients had CF, active pulmonary disorders (TB, sarcoidosis, ABPA), COPD, poorly controlled asthma, creatinine clearance <30 mL·min−1, vestibular instability, or had hypersensitivity to aminoglycosides Gentamicin 80 mg via a jet nebuliser, twice daily, 12 months (n=32) Placebo (0.9% saline) via a jet nebuliser, twice daily, 12 months (n=33) Multicentre, randomised, single-blind, placebo-controlled trial Primary: mean change in sputum bacterial load (log10 CFU·g−1) Secondary: sputum analysis (volume, purulence, MPO, free elastase, bacterial eradication), acute exacerbation, PFT, SGRQ, LCQ, markers of systemic inflammation, adverse events, emergence of bacterial resistance ORBIT-1 trial 2011, sponsored by Aradigm Corp. [24, 25] Australia, Canada, Germany, UK, USA Inclusion criteria: adult patients (≥18 years) had clinically stable, non-CF bronchiectasis confirmed by HRCT, and had PA airway infection Exclusion criteria: patients had either changes in regimen or initiation of azithromycin, hypertonic saline, bronchodilators or oral steroids within 28 days prior to study, had received investigational drug or device within 28 days prior to study, or had any serious or active medical or psychical conditions Liposomal ciprofloxacin 100 mg (n=30), 200 mg (n=32) via a nebuliser, once daily, 28 days Matching placebo via a nebuliser, once daily, 28 days (n=33) International, multicentre, RDBPCT Primary: mean change in sputum PA density (log10 CFU·g−1) from baseline to day 28 Secondary: acute exacerbations, PFT, quality of life scores, safety and tolerability Orriols 1999, no sponsor [32] Spain Inclusion criteria: adult patients had bronchiectasis diagnosed by bronchography, CT or both, had ≥3 positive sputum cultures for PA during the year prior to study, and had been treated at least once with oral ciprofloxacin in the past 3 months because of exacerbation Exclusion criteria: patients had CF, immunodeficiency, enzymatic deficiency, congenital disease, hypersensitivity or bacterial resistance to β-lactams or aminoglycosides, or had kidney failure Tobramycin 100 mg + Ceftazidime 1000 mg via a jet nebuliser, twice daily, 12 months (n=8) Symptomatic treatment with oxygen, bronchodilators and corticosteroids (n=9) Randomised, open-label, controlled trial Microbiological study (bacterial eradication) of sputum, hospitalisation, use of antibiotic, PFT, adverse events, emergence of bacterial resistance Serisier 2013, sponsored by Aradigm Corp. [33] Australia, New Zealand Inclusion criteria: adult patients had clinically stable bronchiectasis diagnosed by CT, PA airway infection, and had ≥2 exacerbations requiring antibiotic therapy in the preceding 12 months Exclusion criteria: patients had CF, ABPA, or pulmonary non-TB mycobacterial infection DRCFI (liposomal ciprofloxacin 150 mg + free ciprofloxacin 60 mg) via PARI LC sprint nebuliser, once daily, three treatment cycles of 28 days “on” inhaled therapy, 28 days “off” (n=20) Matched placebo (liposomal 15 mg or 0.9% saline) via PARI LC sprint nebuliser, once daily, three treatment cycles of 28 days “on” inhaled therapy, 28 days “off” (n=22) International, multicentre, RDBPCT Primary: mean change in sputum PA density (log10 CFU·g−1) from baseline to day 28 Secondary: eradication of PA in sputum, acute exacerbation, PFT, 6MWT, SGRQ, adverse events and tolerability, emergence of bacterial resistance Tabernero 2014, no sponsor [28] Spain Inclusion criteria: adult patients had non-CF bronchiectasis diagnosed by HRCT, had chronic PA airway infection after an acute exacerbation admission and appropriate antimicrobial therapy Exclusion criteria: not stated Colistin 1 million IU via a nebuliser, twice daily, 1 year (n=20) Conventional therapy, 1 year (n=19) Randomised, open-label, controlled trial Primary: need for hospital readmissions Secondary: sputum microbiology, clinical symptoms, PFT, adverse events TR02-107, 2009, sponsored by Insmed Inc. [26, 27] Bulgaria, Greece, Hungary, India, Serbia, Ukraine Inclusion criteria: adult patients (≥18 years) had non-CF bronchiectasis diagnosed by HRCT, had chronic PA airway infection, had SaO2 ≥90% while breathing room air, and were able to produce ≥0.5 g sputum Exclusion criteria: patients had CF, ABPA, aspiration of foreign body, pulmonary TB or non-TB mycobacterial infection, history of lung transplantation, FEV1 <50% predicated, use of any type of antibiotics within 4 weeks prior to the study, evidence of biliary cirrhosis with portal hypertension Arikace (liposomal amikacin) 280 mg or 560 mg, via an eFlow nebuliser, once daily, 28 days (n=44) Matched placebo (liposomes in 1.5% saline) via an eFlow nebuliser, once daily, 28 days (n=20) International, multicentre, RDBPCT Primary: adverse events Secondary: mean change in sputum PA density, acute exacerbation, hospitalisation, PFT, SGRQ Wilson 2013, sponsored by Bayer Pharma AG [11] Australia, Germany, Spain, Sweden, UK, USA Inclusion criteria: adult patients (≥18 years) had non-CF bronchiectasis diagnosed by HRCT, had ≥2 exacerbations requiring systemic antibiotics or ≥1 hospitalisation for intravenous antibiotics in the previous 12 months, had stable disease in the preceding 30 days, and were able to produce sputum (≥5 mL) that was culture positive for potential respiratory pathogens Exclusion criteria: patients had active non-TB mycobacterial infection, recent significant haemoptysis, use of nebulised antibiotics as maintenance treatment, or use of systemic antibiotics for exacerbation within 4 weeks before randomisation Ciprofloxacin 32.5 mg via dry powder for inhalation, twice daily, 28 days (n=60) Matching placebo via dry powder for inhalation, twice daily, 28 days (n=64) International multicentre, RDBPCT Primary: mean change in sputum bacterial load (log10 CFU·g−1) from baseline to day 28 Secondary: acute exacerbation, hospitalisation, sputum analysis (bacterial eradication, volume, colour), PFT, markers of systemic inflammation, SGRQ, adverse events, emergence of bacterial resistance CF: cystic fibrosis; HRCT: high-resolution computed tomography; TB: tuberculosis; RDBPCT: randomised, double-blind, placebo-controlled trial; QoL-B: quality of life-bronchiectasis; CT: computed tomography; PA: Pseudomonas aeruginosa; ABPA: allergic bronchopulmonary aspergillosis; PFT: pulmonary function test; SGRQ: St George’s Respiratory Questionnaire; FEV1: forced expiratory volume in 1 s; COPD: chronic obstructive pulmonary disease; MPO: myeloperoxidase; LCQ: Leicester Cough Questionnaire; DRCFI: dual release ciprofloxacin for inhalation; 6MWT: 6-min walk test; SaO2: arterial oxygen saturation.
- Table 2– Adverse events of inhaled antibiotics in patients with non-cystic fibrosis bronchiectasis
Adverse events Events/patients Trials n Risk ratio (95% CI) p-value I2 % Antibiotic group Control group Death 7/304 (2.3) 4/286 (1.4) 8 1.28 (0.44–3.71) 0.65 0 Withdrawal due to adverse events 37/304 (12.2) 35/286 (12.2) 8 1.00 (0.67–1.50) 0.99 0 Bronchospasm 26/260 (10.0) 6/266 (2.3) 7 2.96 (1.30–6.73) 0.01 0 Cough 15/97 (15.5) 14/101 (13.9) 2 0.54 (0.03–0.52) 0.69 76.3 Haemoptysis 6/97 (6.2) 5/101 (4.9) 2 1.26 (0.39–4.01) 0.70 0 Data are presented as n/N (%), unless otherwise stated.
Supplementary material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Files in this Data Supplement:
{kind=link}
{kind=link}










