





Abstract
The aim of this study was to establish which cut-off point for the forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ratio (i.e. fixed 0.70 or lower limit of normal (LLN) cut-off point) best predicts accelerated lung function decline and exacerbations in middle-aged smokers.
We performed secondary analyses on the Lung Health Study dataset. 4045 smokers aged 35–60 years with mild-to-moderate obstructive pulmonary disease were subdivided into categories based on presence or absence of obstruction according to both FEV1/FVC cut-off points. Post-bronchodilator FEV1 decline served as the primary outcome to compare subjects between the categories.
583 (14.4%) subjects were nonobstructed and 3230 (79.8%) subjects were obstructed according to both FEV1/FVC cut-off points. 173 (4.3%) subjects were obstructed according to the fixed cut-off point, but not according to the LLN cut-off point (“discordant” subjects). Mean±se post-bronchodilator FEV1 decline was 41.8±2.0 mL·year−1 in nonobstructed subjects, 43.8±3.8 mL·year−1 in discordant subjects and 53.5±0.9 mL·year−1 in obstructed subjects (p<0.001).
Our study showed that FEV1 decline in subjects deemed obstructed according to a fixed criterion (FEV1/FVC <0.70), but non-obstructed by a sex- and age-specific criterion (LLN) closely resembles FEV1 decline in subjects designated as non-obstructed by both criteria. Sex and age should be taken into account when assessing airflow obstruction in middle-aged smokers.
Abstract
Lower limit of normal cut-off best predicts accelerated lung function decline and exacerbation in middle-aged smokers http://ow.ly/qaZnz
Introduction
Chronic obstructive pulmonary disease (COPD) is characterised by irreversible airflow obstruction and progressive decline of lung function [1]. COPD is a major cause of morbidity and mortality [2, 3]. A recent worldwide study indicated an overall prevalence of spirometry-confirmed COPD among middle-aged and elderly people of approximately 10% [4].
The clinical COPD guidelines issued by the Global Initiative for Obstructive Lung Disease (GOLD) and the National Institute for Health and Care Excellence recommend that obstruction should be defined as a forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ratio at a fixed value of <0.70 [3, 5, 6]. In contrast, in their lung function guidelines, the American Thoracic Society (ATS) and the European Respiratory Society (ERS) advocate the use of a “lower limit of normal” (LLN) approach to define abnormally low FEV1/FVC values [7].
The fixed 0.70 cut-off point is probably not an accurate reflection of abnormal lung function at all ages, because it has been shown convincingly that the FEV1/FVC ratio declines with age in healthy persons [8, 9]. This could imply that by using a fixed cut-off point, some middle-aged and elderly people are incorrectly considered to have airflow obstruction while their FEV1/FVC is actually in the normal range.
A recent review of all published studies concluded that the prevalence of spirometry-confirmed COPD in middle-aged and elderly people is greater when using the fixed 0.70 threshold for the FEV1/FVC ratio than when using a LLN definition of the ratio. Discordant prevalence rates occurred in 4–20% of cases [10]. However, longitudinal studies are needed to determine which of the two approaches best predicts future COPD-related outcomes. The few studies that have looked at this so far used pre-bronchodilator FEV1 and evaluated all-cause mortality as an outcome, rather than COPD-specific mortality [11–13]. None of these studies were able to look at the most important marker of COPD prognosis, i.e. accelerated post-bronchodilator lung function decline.
Because the variability of pulmonary function increases with age and normal values for the FEV1/FVC ratio are highly skewed, a FEV1/FVC threshold based on the common method for calculating the LLN (i.e. simply calculating the fifth percentile of the distribution of z-scores of healthy never-smokers, assuming a normal distribution) may have limited diagnostic accuracy in an older population. Therefore, the so-called “LMS” (lambda, mu, sigma) method, has recently been recommended for calculating the LLN of the FEV1/FVC ratio [14, 15]. The aim of the study reported in this paper was to establish whether the fixed 0.70 or a LMS cut-off point for the FEV1/FVC ratio performs best in predicting accelerated post-bronchodilator lung function decline in middle-aged smokers. Pre-bronchodilator FEV1 decline and pre- and post-bronchodilator FVC decline were secondary outcomes. We also investigated which of the two approaches best predicts the risk of exacerbations and respiratory-related hospital admissions.
Methods
Study design and population
We used data from the Lung Health Study [16, 17], a 5-year randomised controlled clinical trial in 5887 smokers aged 35–60 years with mild-to-moderate obstructive pulmonary disease. A full description of the design of the Lung Health Study can be found elsewhere [16–18].
Spirometry
Spirometry measurements were obtained during three screening visits and annually for a period of 5 years. Participants were tested before and after two inhalations of the bronchodilator isoproterenol. All spirometry tests were performed according to ATS standards [19]. More details about quality assurance of the spirometry tests can be found elsewhere [17].
Definitions of airflow obstruction and subject selection
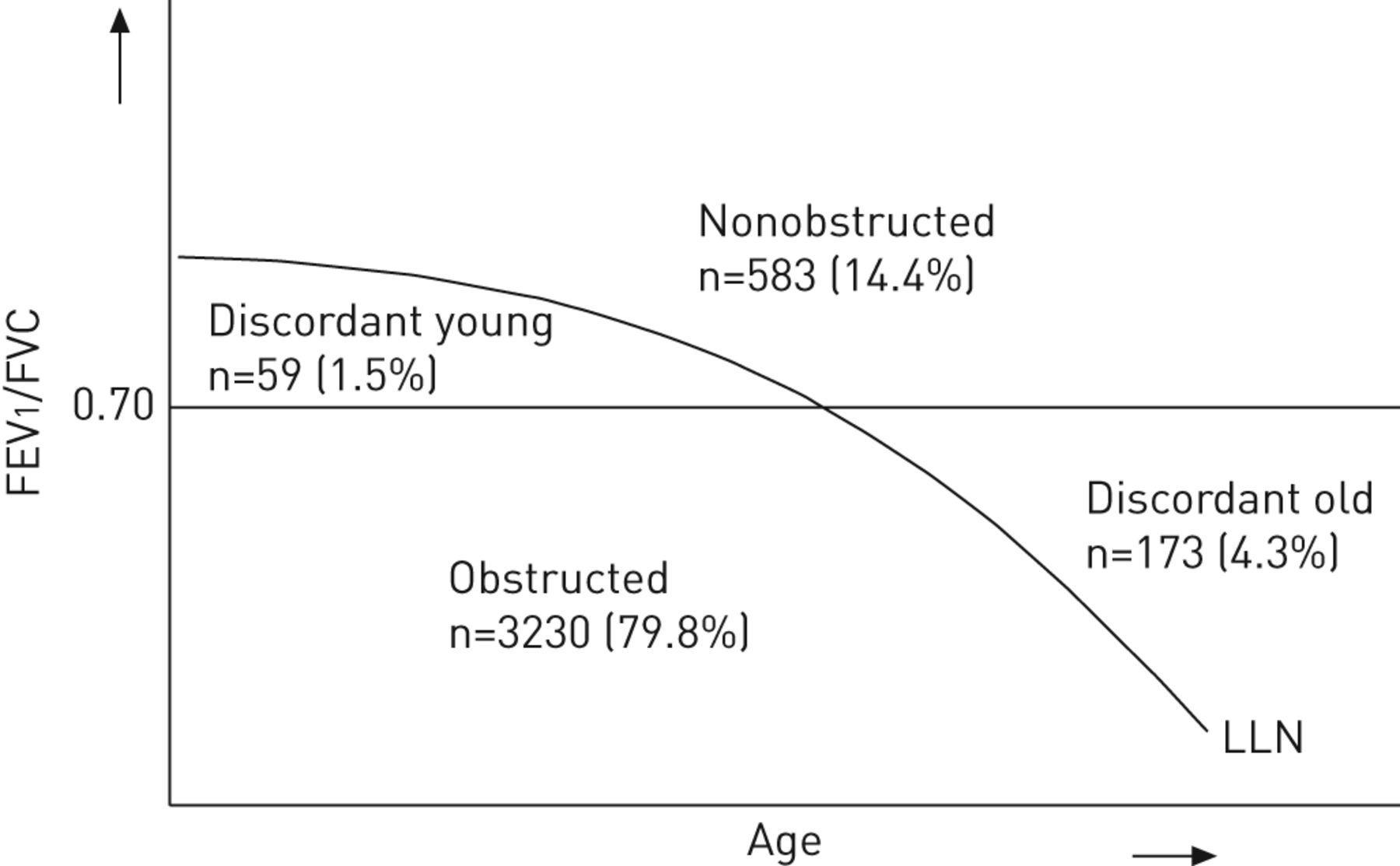
We defined the LLN using the LMS method (online supplementary material). The LMS method is a common approach for constructing growth charts in a biologically plausible way [15, 20–22] and is currently considered the best method to define the LLN [14]. The study population was subdivided into four categories based on the presence of airflow obstruction as defined by the LMS and the fixed 0.70 FEV1/FVC cut-off point definitions: 1) “LMS-/ fixed-” (absence of airflow obstruction according to both definitions, i.e. “nonobstructed” subjects); 2) “LMS+/fixed-” (presence of airflow obstruction according to the LMS definition, but absence of airflow obstruction according to the fixed definition, i.e. “discordant young” subjects); 3) “LMS-/fixed+” (absence of airflow obstruction according to the LMS definition, but presence of airflow obstruction according to the fixed definition, i.e. “discordant old” subjects); and 4) “LMS+/fixed+” (presence of airflow obstruction according to both definitions, i.e. “obstructed” subjects).
figure 1 illustrates these categories. We restricted our analysis to 4045 subjects who were consistently classified in the same category at the screening visits and the follow-up visit 1 year later (fig. 2).

Graphical representation of the different cut-off points and categories when defining airflow obstruction for a population sample. In reality, the curved lower limit of normal (LLN) line is right-shifted in females compared to males, which explains why discordant young subjects are predominantly female and discordant old subjects predominantly male. FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity.

Selection of study subjects from the Lung Health Study dataset.
Lung function decline
Accelerated lung function decline over time as the hallmark of disease progression can be considered the gold standard for obtaining a correct COPD diagnosis [10, 23]. Therefore, our primary outcome was the annual rate of post-bronchodilator FEV1 decline (see online supplementary material for secondary outcome).
Study definitions for exacerbations and hospital visits
Exacerbations were defined based on two items in the annual questionnaire. Respiratory-related hospital admissions were used as secondary outcomes (online supplementary material).
Smoking behaviour
Self-reported quit status for smoking cigarettes (yes/no) was recorded annually and validated by either salivary cotinine or carbon monoxide levels.
Statistical analysis
SAS software 9.2 (SAS Institute Inc., Cary, NC, USA) was used for all analyses. A random coefficient linear regression model with random intercept and random slope was used to estimate the annual decline (PROC MIXED). Smoking behaviour was included in the model as a time-dependent binary covariate. The comparison of the discordant old and obstructed categories (fig. 1) was the principal part of the analyses, but we also compared lung function decline between all discordant subjects and nonobstructed subjects.
ANOVA, t-test and Pearson’s Chi-squared test were used to determine if the four categories differed with regard to baseline characteristics, proportions of exacerbations and respiratory-related hospital admissions. A value of p<0.05 was considered to be statistically significant.
Results
Study subjects
The original Lung Health Study study population consisted of 5887 smokers aged 35–60 years. We excluded 1842 subjects because 1276 subjects were in different categories based on the fixed and LMS definitions for airflow obstruction during their baseline and first annual visits and 566 subjects had one missing spirometry result. From the 1276 subjects with unstable classification, 681 (53.4%) subjects lost their obstructed status and 595 (46.6%) subjects obtained an obstructed status. Ultimately, 4045 (68.7%) subjects could be included in the analysis (fig. 2). table 1 shows baseline characteristics for the study population and for the excluded subjects. The latter subjects showed higher spirometry values compared to the study population.
The nonobstructed category comprised 583 (14.4%) subjects, the discordant young category 59 (1.5%), the discordant old category 173 (4.3%) and the obstructed category 3230 subjects (79.8%).
table 2 shows the characteristics of the categories. The discordant young category showed a low proportion of males (6.8%) and the discordant old category a high proportion of males (87.9%), compared to the obstructed (61.2%) and nonobstructed categories (64.2%) (fig. 3).

Plotting age against baseline post-bronchodilator forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ratio for a) male (n=2513) and b) female (n=1532) subjects in the study population. Nonobstructed: not obstructed to any cut-off point; discordant young: obstructed according to the lambda–mu–sigma (LMS) cut-off point, but not the fixed; discordant old: obstructed according to the fixed cut-off point, but not the LMS; obstructed: obstructed according to both cut-off points.
With a mean±sd age of 55.5±3.4 years, the subjects in the discordant old category were significantly older than those in the obstructed category (48.6±6.6 years), the nonobstructed category (46.8±6.6 years) and the discordant young category (38.7±2.5 years). The mean post-bronchodilator FEV1 of 76.1±9.1% predicted in the obstructed category was lower than in the other three categories. The nonobstructed, discordant young and discordant old categories had mean±sd post-bronchodilator FEV1 values of 83.5±7.5% pred, 83.8±7.2% pred and 81.4±7.6% pred, respectively.
Lung function decline
table 3 shows the adjusted estimates of the mean annual decline in post-bronchodilator FEV1 and annual decline for the secondary outcomes for each of the categories. Mean post-bronchodilator FEV1 decline differed significantly between the categories (p<0.001). Subjects in the young discordant and old discordant categories showed mean post-bronchodilator FEV1 declines of 38.7 mL·year−1 and 43.8 mL·year−1, respectively. This was very similar to the decline in the nonobstructed category of 41.8 mL·year−1 (p=0.634 for the young discordant subjects and p=0.654 for the old discordant subjects), but significantly less than the decline in the obstructed category of 53.5 mL·year−1 (p=0.020 for the young discordant subjects and p=0.012 for the old discordant subjects).
Secondary outcomes
Spirometry
table 3 shows that the estimated decline of pre-bronchodilator FEV1, pre-bronchodilator FVC and post-bronchodilator FVC follow the same pattern as the post-bronchodilator FEV1 for the different categories. Analysis of pre-bronchodilator FEV1 values also indicated similarity in terms of decline between the discordant and nonobstructed categories (table 3) (p=0.672 for the young discordant subjects and p=0.091 for the old discordant subjects), but dissimilarity between the discordant and obstructed categories (p<0.001 for the young discordant subjects and p<0.001 for the old discordant subjects). The same results were observed for pre-bronchodilator FVC decline. Post-bronchodilator FVC decline did not differ significantly between the young discordant (35.9 mL·year−1) and obstructed (48.5 mL·year−1) subjects (p<0.092) and between the old discordant (41.0 mL·year−1) and obstructed (48.5 mL·year−1) subjects (p<0.102).
Exacerbations
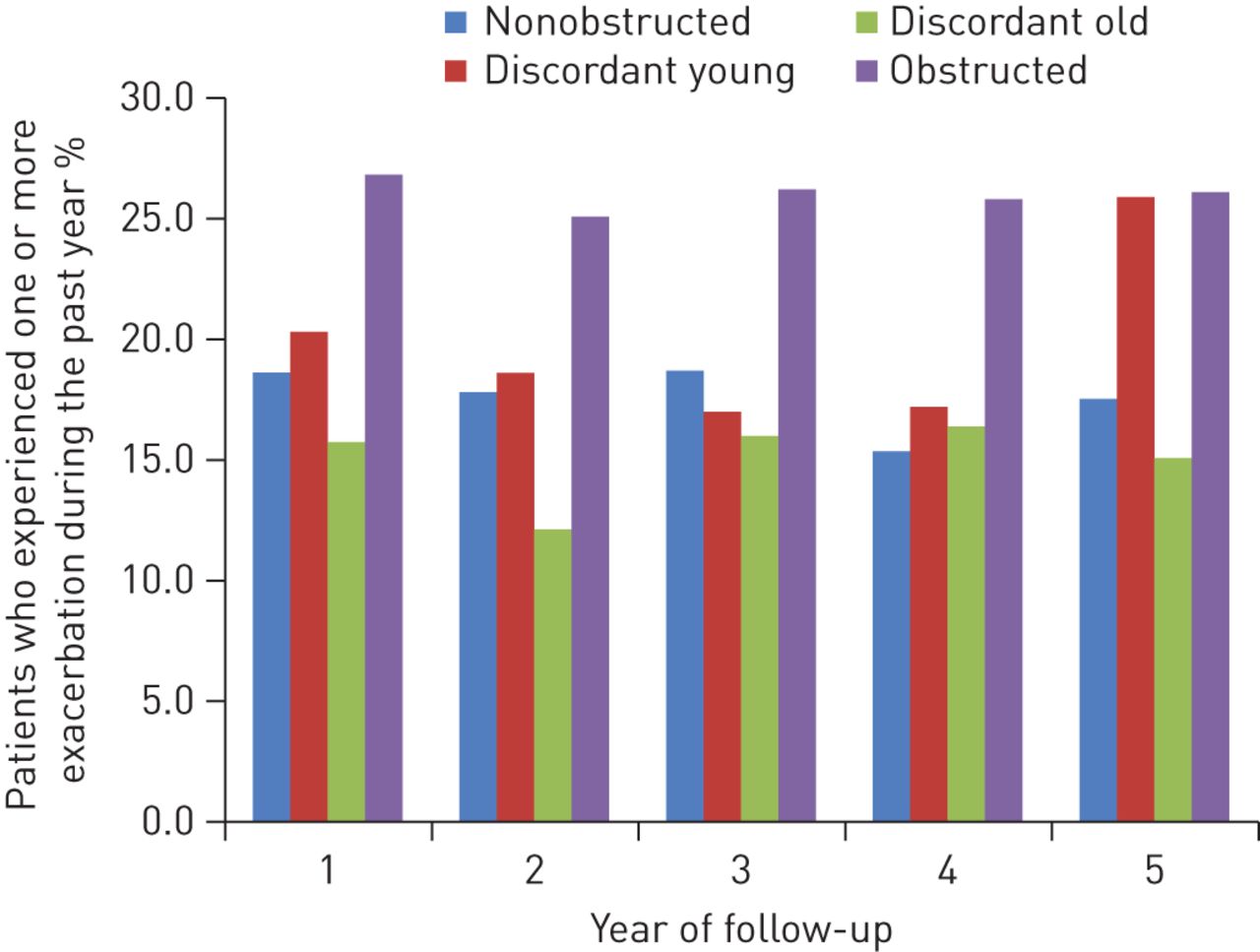
figure 4 shows the proportion of subjects who experienced one or more exacerbation during the past year, measured annually over a 5-year observation period. At all visits, the overall differences in the proportion of subjects with exacerbations between the categories were statistically significant (p<0.001). The obstructed category showed the highest proportion of subjects with exacerbations (26.8%), while the discordant old category showed the lowest proportion (15.7%). During the study period, the proportion of subjects with one or more exacerbations was stable for most categories except for the young discordant category, which started with a proportion of 20.3%, decreased to 15.5% during the following visits and increased to 25.9% at the last annual visit.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proportion of subjects who experienced one or more exacerbation during the past year.
Hospital visits
During the 5-year follow-up period 22 respiratory-related hospital admissions were registered in the obstructed category and no respiratory-related hospital registration in the other three categories.
Discussion
In this study, we focused on the rate of lung function decline in subjects identified as obstructive by the fixed 0.70 FEV1/FVC cut-off point but as nonobstructive by a LMS cut-off point for this ratio. In addition we found a small category of younger people, predominantly females, with presence of airflow obstruction according to the LMS definition, but absence of airflow obstruction according to the fixed definition. The mean annual post-bronchodilator FEV1 decline in the subjects in both discordant categories was very similar to subjects who were nonobstructive according to both definitions. However, post-bronchodilator FEV1 decline was 9.7 mL·year−1 lower than the mean decline in subjects with FEV1/FVC values below both cut-off points (“obstructed category”).
During the study period, the proportion of subjects with at least one exacerbation was stable for most categories, except for the young discordant category, in which we observed an increase to the same level as in the obstructive category at the end of the study period. Although this category (n=59) had the lowest mean annual post-bronchodilator FEV1 decline, this notable increase in exacerbations in year 5 might be an indication of development or progression of early COPD. However, this observation should be interpreted with caution: because of the small number of subjects in this group, a few subjects changing status has a considerable influence on the percentage developing more symptoms. In the old discordant category, the proportion of subjects with at least one exacerbation was consistently lower than in the obstructed category and comparable with the proportion in the nonobstructed category. Together with the finding that the mean lung function decline is similar to the nonobstructed category, this is an indication that subjects in the old discordant category do not suffer from a progressive chronic obstructive condition, i.e. COPD.
We chose to analyse respiratory-related hospital admissions because we consider this a better indicator of prognosis of COPD than all-cause hospitalisations. We are aware of the fact that it is challenging to assign exactly one primary cause for hospitalisation. However, in the Lung Health Study all participant-reported hospitalisations were verified by checking the hospital records, coding by an experienced coder and checking by a panel of three expert physicians. So we believe it is a reliable outcome measure. The number of respiratory-related hospital admissions was small (22 during the 5 years of follow-up), but they all occurred in the obstructed category. The relative young age of the study population (35–60 years) and the fact that they were not selected because of a previous diagnosis of COPD and mainly had mild-to-moderate obstruction are possible explanations for this low number of respiratory-related hospital admissions.
Comparison with existing literature
In a recent analysis of the Lung Health Study cohort, Drummond et al. [24] concluded that individuals with lower baseline FEV1/FVC ratio have more rapid decline and worse mortality, and that it may be necessary to lower the threshold to FEV1/FVC <0.65 or Z-scores < -2.0 to identify those at increased risk of a more rapid fall in FEV1. Several studies have shown that lung function decline is accelerated in individuals diagnosed with COPD [1, 25, 26]. However, these studies did not focus on the definition of airway obstruction itself, but only used the current GOLD criteria in their final analysis. Other studies have reported high rates of false positive diagnostic interpretations when the fixed and LLN definitions for airflow obstruction are used to classify subjects as obstructive [27–31]. False-positive interpretations may cause erroneous diagnoses in individuals and inflation of COPD population prevalence rates [32]. This proportion of false positives increased with age, as the variance of FEV1/FVC increased with age. Our research group previously showed that as much as 43% of subjects aged >80 years were wrongly labelled as having airway obstruction when using the fixed 0.70 cut-off for the ratio in comparison to a LLN definition [33]. While these studies are good examples of how prevalence figures differ when using a cross-sectional design and different cut-off points, they do not provide information regarding the longitudinal course of clinical markers of COPD prognosis or actual disease outcome. In a previous study we have shown that in a primary care cohort of undiagnosed adults, lung function below the normal range and early respiratory signs predicted the development and progression of COPD in the next five years [34].
The use of a fixed cut-off point also seems to cause misclassification of airflow obstruction in younger adults (i.e. aged <45 years), as has recently been reported by Cerveri et al. [35]. These misclassified (or “underdiagnosed”) subjects were more likely to develop COPD in the following 9 years, and had higher respiratory-related healthcare than subjects without airflow obstruction according to LLN cut-off points. In our current study, the fixed 0.70 FEV1/FVC cut-point identified 94.1% of subjects with evidence of airflow obstruction according to LLN cut-points. This misclassification is small compared to the result reported by Cerveri et al. [35] but our study population was rather different, with a higher proportion of obstructed subjects (81.3% versus 9.3%) and a substantial history of cigarette smoking in all study subjects.
Studies that use the LMS method are still scarce as it is a novel way to define airflow obstruction. Stanojevic and co-workers [15, 22] proposed the use of the LMS method because this method improves the accuracy of reference data for pulmonary function and, as a consequence, results in less misdiagnosis when defining airflow obstruction.
Some may argue that the use of a statistically derived cut-off point overly complicates the interpretation of spirometry when diagnosing airflow obstruction. However, even simple office spirometers and computer software can calculate the LMS and could easily be reprogrammed to display it. Even when not available, a graphical aid similar to growth charts used in children could be provided to support interpretation of spirometry tests.
Strengths and limitations
The main strength of this study is that we were able to look at post-bronchodilator FEV1 values instead of pre-bronchodilator FEV1 as used by all previous studies that have looked at detection of airflow obstruction [14, 36]. This ensures that subjects with reversible obstruction were correctly considered as being obstructive, as there is a general consensus among COPD experts and guidelines that post-bronchodilator measurement of the ratio should be used when diagnosing COPD and assessing the severity of airflow obstruction. The quality of the spirometry tests in the Lung Health Study was very high, resulting in accurate estimates of lung function decline for the different categories [17].
Another strength is the availability of longitudinal data for 4045 subjects, allowing us to follow lung function decline in different categories of obstruction for several years. This enabled the subdivision of our study cohort into four categories, while each category still contained a substantial number of subjects. The novel LMS method was used, which describes the relationship between lung function, height and age for both sexes more precisely than the LLN method does.
Because the goal of our study was to compare clearly defined and consistent groups of subjects based on fixed and LMS definitions for airflow obstruction, we only included those subjects who did not shift between categories during their baseline and first annual follow-up visit. As a consequence 1276 (24%) subjects were excluded from the analysis. This finding shows that a one-off spirometry test does not seem to be sufficient to determine airflow obstruction in a substantial proportion of subjects, and suggests that a COPD diagnosis should not be based on a single spirometry test. Excluding these subjects clearly comes at the cost of generalisability. Therefore, our analysis should be seen as a “proof-of-concept” study regarding the presumption that when diagnosing COPD, it is more appropriate to use sex- and age-specific cut-off points for the FEV1/FVC ratio than it is to use a “one size fits all” fixed (0.70) cut-off point.
Conclusion
In conclusion, our study shows that when looking at the cross-sectional description of the study population, the prevalence of airflow obstruction in 35–60-year-old smokers with mild-to-moderate obstructive pulmonary diseases greatly differs when different cut-off points for the FEV1/FVC ratio are used. In addition, the discordant categories seem to be comprised of subjects who have a less accelerated decline in post-bronchodilator FEV1 than those in the obstructed category. We recommend the use of the LMS approach when defining airflow obstruction in the process of diagnosing COPD. Recently, the Global Lungs Initiative has published new spirometric lung function reference values, which were also based on the LMS method [37].
Acknowledgments
This manuscript was prepared using Lung Health Study (LHS) research materials obtained from the National Heart, Lung, and Blood Institute (NHLBI) Biologic Specimen and Data Repository Information Coordinating Center and does not necessarily reflect the opinions or views of the LHS or the NHLBI.
Footnotes
This article has supplementary material available from www.erj.ersjournals.com
Support statement: Funding of this study was supported by Radboud university medical center, Nijmegen, The Netherlands.
Conflict of interest: Disclosures can be found alongside the online version of this article at www.erj.ersjournals.com
- Received October 5, 2012.
- Accepted March 13, 2013.
- ©ERS 2014
References










