





Abstract
We aimed to characterise the association of pulmonary hypertension due to hypoventilation and exercise capacity, and the haemodynamic and functional changes under noninvasive ventilation.
A retrospective analysis was carried out to assess haemodynamics and functional capacity in 18 patients with daytime pulmonary hypertension, due to hypoventilation, at baseline and after 3 months of noninvasive ventilation.
Patients presented with a mean±sd pulmonary artery pressure of 49±13 mmHg, preserved cardiac index (3.2±0.66 L·min−1·m−2), 6-min walking distance of 303±134 m and severely elevated N-terminal pro-brain natriuretic peptide (NT-proBNP) levels. Mean pulmonary artery pressure correlated negatively with maximum work rate (R= -0.72; p=0.03) and 6-min walking distance (R= -0.62; p=0.01). Following noninvasive ventilation we found a significant reduction of mean pulmonary artery pressure (-18 mmHg; p<0.001) and NT-proBNP levels (-2110 pg·mL−1; p=0.001), and improvement in the 6-min walking distance (+66 m; p=0.008) and maximum work rate (+18 W; p=0.028). Changes in work rate correlated inversely with pulmonary artery pressure (R= -0.75; p=0.031).
In this specific cohort with hypoventilation and severe pulmonary hypertension, pulmonary hypertension was associated with reduced exercise capacity. Following noninvasive ventilation, haemodynamics and exercise capacity improved significantly.
Abstract
Pulmonary hypertension due to alveolar hypoventilation is associated with functional impairment and improved by NIPPV http://ow.ly/pMYlL
Introduction
Interest in severe obesity hypoventilation syndrome (OHS) is growing because of its increasing incidence and associated high morbidity and mortality [1]. The rising number of patients with severe pulmonary hypertension (PH) due to alveolar hypoventilation is of particular concern. In obstructive sleep apnoea (OSA) and overlap syndrome, PH is rare and pulmonary artery pressure (PAP) is only mildly elevated. By contrast, in alveolar hypoventilation, PH is more frequently observed and of higher severity [2–6]. The pathogenesis of PH in patients with alveolar hypoventilation is still unclear. Hypoxia may lead to an increase in PAP, but significant interspecies and, in humans, interindividual differences in acute pulmonary vasoconstriction have been reported [3, 7–9]. Although carbon dioxide (CO2) and acidosis influence pulmonary vasoconstriction, not all patients with hypoventilation and hypercapnia develop PH [10, 11]. A high prevalence of pulmonary arterial and pulmonary venous hypertension was reported in obese patients in an autopsy study [12]. The positive correlation between body weight and PAP in OSA underscores the possible influence of obesity on pulmonary haemodynamics [3]. However, PH does not occur in all obese patients [6]. The extent of functional impact of PH in patients with hypoventilation is still unknown.
Current guidelines recommend treatment of the underlying disease for PH occurring due to lung diseases and ventilatory disorders [13, 14]. Oxygen administration alone stabilised, but did not reduce PAP in patients with chronic obstructive pulmonary disease (COPD) [15], and failed to improve haemodynamics in patients with chest wall diseases and OHS [16]. Following surgically induced weight loss, a long-term decline in PAP has been shown [6, 17]. Despite improving blood gases in patients with OSA and hypercapnia [18], application of continuous positive airway pressure (CPAP) had no effect on pulmonary haemodynamics in patients with OSA [19]. Noninvasive positive-pressure ventilation (NIPPV) in patients with OHS improved blood gases [20–23], vital capacity, expiratory reserve volume [21, 23], daytime sleepiness and dyspnoea [24, 25]. Moreover, long-term NIPPV has been found to increase serum leptin levels [26]. Patients with OSA and hypercapnia exhibited an increased chemo-responsiveness to CO2 and hypoxaemia under CPAP [23, 26, 27]. NIPPV was shown to have a positive effect on the haemodynamics of patients with alveolar hypoventilation due to thoracic restriction [28]. However, the effect of NIPPV on PH and exercise capacity of obese patients with alveolar hypoventilation, has not been studied.
The objective of this research was to study haemodynamics in a cohort of patients with daytime PH and alveolar hypoventilation, as well as to define the impact of PH on functional capacity. Furthermore, we aimed to analyse the effect of NIPPV on haemodynamics and functional capacity.
Methods
Study subjects were recruited from all consecutive 160 patients who presented to the Medical Mission Hospital (Würzburg, Germany) between October 2009 and July 2011 for further evaluation and treatment of PH. 18 patients met the criteria of daytime PH and alveolar hypoventilation and were retrospectively analysed (fig. 1). Patients with confirmed PH (mean PAP (mPAP) at rest ≥25 mmHg or mPAP at rest <25 mmHg and mPAP at exercise ≥50 mmHg or, if right heart catheterisation could not be performed, an echocardiographic systolic PAP ≥50 mmHg at rest and daytime CO2 of ≥45 mmHg or a mean night-time CO2 of ≥55 mmHg) were included. Exclusion criteria were chronic thromboembolic pulmonary hypertension or pulmonary arterial hypertension (PAH) associated diseases such as cardiac shunt, collagen vascular disease, porto-pulmonary hypertension, HIV-associated PAH, and drug- and toxin-induced PAH. Written informed consent was obtained from all patients prior to analysis. The study was approved by the Ethics Committee of the Medical Faculty of the Julius Maximilian University Würzburg (Würzburg, Germany).

Patient selection for retrospective analysis of 18 patients with pulmonary hypertension (PH) and alveolar hypoventilation.
Diagnosis was established according to current guidelines [13]. Echocardiography (Vivid7; GE Medical Systems, Solingen, Germany) was performed to measure systolic right ventricular pressure, and right and left ventricular function, as well as to rule out a cardiac shunt and significant valvular pathology. ECG (ECG 550020728; GE Medical Systems) was also performed. Body plethysmography (Masterscreen Body/Diff; CareFusion, Höchberg, Germany) was performed according to the European Respiratory Society statement [29]. Inspiratory mouth pressures were measured as described previously [30]. Computed tomography (Activion 16; Toshiba Medical Systems, Neuss, Germany) was conducted to rule out structural lung disease. A ventilation/perfusion scan (Technegas-Generator (Tetley Medical Limited, Lucas Heights, Australia) and E Cam Variable (Siemens Medical Solutions Inc., Hoffman Estates, IL, USA)) was performed to rule out pulmonary embolism. Blood gases were measured at rest and under exercise (ABL 800 Basic; Radiometer, Cadolzburg, Germany). Functional capacity was characterised by a 6-min walk test, carried out according to the American Thoracic Society (ATS) statement [31]. In capable patients, a bicycle cardiopulmonary exercise test (Masterscreen CPX (CareFusion) and E-bike basic PC plus (GE Medical Systems)) was performed according to the ATS and the American College of Chest Physicians (ACCP) statement [32]. Daytime right heart catheterisation was performed according to the guidelines using a Swan-Ganz catheter (Smith Medical, Grasbrunn, Germany) [15]. Measurements were conducted with the monitor system (IntelliVue MP70 (M8007A); Philips Medizinsysteme, Böblingen, Germany). A night-time cardiorespiratory polygraphy, including measurement of nocturnal oxygen saturation and CO2 tension (Somnocheck (Weinmann, Hamburg, Germany) and TOSCA (Radiometer GmbH, Willich, Germany)) was performed according to the ACCP guidelines [33]. Serum levels of N-terminal pro-brain natriuretic peptide (NT-proBNP) were measured by ECLIA (Elecys 2010; Roche Diagnostik, Mannheim, Germany).
All 18 patients with confirmed PH and alveolar hypoventilation were treated using noninvasive bi-level positive-pressure ventilation according to the guidelines of the German Respiratory Society [34] (using Harmony II (Respironics, Herrsching, Germany) or Stellar 150 (ResMed, Martinsried, Germany)). All patients were assessed by a routine follow-up 3 months after initiation of the ventilation therapy. The same diagnostic tests used at baseline were carried out during the follow-up.
Only the patients with data available at both baseline and the 3 month follow-up assessment were considered for analysing mean changes in each parameter. Statistical analyses were performed using Statistica (Version 10; StatSoft Inc., Tulsa, OK, USA). The mean and standard deviation were calculated. Correlations of the parameters were evaluated by Spearman test. Statistical significance was expressed as p-values with the Wilcoxon test and assumed if the p-value was <0.05.
Results
Baseline characteristics
Patients were selected as shown in figure 1. table 1 and online supplementary tables 2–3 show the characteristics of the 18 patients (11 females and seven males). Mean±sd age was 62±10 years, body mass index (BMI) was 36.1±9.8 kg·m−2 and body weight was 104±30 kg. 12 patients fulfilled the criteria of OHS. Three out of these 12 patients had concomitant COPD. In 5 patients COPD was the sole cause for hypoventilation.
Patients had a reduced vital capacity (VC) (51±19% predicted), forced expiratory volume in 1 s (FEV1) (43±18% pred), elevated residual volume (RV) (167±77% pred) and a mean total lung capacity of 94±33% pred. The cohort showed daytime hypercapnia and hypoxaemia, which was aggravated at night-time.
Apnoea/hypopnoea index (AHI) was elevated in two patients (30 events·h−1 and 60 events·h−1). The mean AHI of the other patients was 3±2 events·h−1. The maximum inspiratory mouth pressure was severely reduced to 3.3±1.9 kPa, and the respiratory load was 0.5±0.2 kPa.
Echocardiography showed signs of right ventricular dysfunction, but normal left ventricular systolic function. Early transmitral filling (E) to early diastolic mitral annular velocity (E′) ratio (E/E′) was 10±4. Left atrial (LA) volume was slightly elevated. We calculated the right atrial (RA)/LA volume ratio and found a value of 1.8±0.6 (online supplementary table 2).
Right heart catheterisation revealed severely elevated mPAP (49±13 mmHg). In 14 patients pulmonary artery wedge pressure (PAWP) was <15 mmHg, in three patients it was >15 mmHg. However, all patients showed a diastolic pulmonary pressure gradient >9 mmHg (23±10 mmHg) and a transpulmonary vascular gradient >12 mmHg (38 ±12 mmHg). Cardiac index was normal. Heart rate at rest was 75±10 per min and systemic blood pressure was 128/75±18/10 mmHg.
The mPAP correlated positively with BMI and maximum night-time CO2. The pulmonary vascular resistance (PVR) correlated negatively with the maximum inspiratory mouth pressure (fig. 2). There was a positive correlation of mPAP with alveolar–arterial oxygen tension difference (PA–aO2)(R=0.67; p=0.049) and minute ventilation volume (V′E)/CO2 output (V′CO2) (R=0.84; p<0.01) and a negative correlation between mPAP and respiratory exchange rate (RER) at maximum exercise (R= -0.80; p=0.01), as well as a negative correlation of PVR with end-tidal carbon dioxide tension (PETCO2) at the anaerobic threshold (R= -0.89, p<0.01). There was no significant correlation of PAP with night-time oxygen saturation, daytime oxygen tension at rest or exercise, left ventricular function or static and dynamic pulmonary volumes (data not shown).

Correlation of a) mean pulmonary artery pressure (mPAP) and body mass index (BMI) (n=17, r=0.62 (95% CI 0.20–0.85); p=0.008); b) mPAP and maximum night-time carbon dioxide tension (PCO2) (n=16, r=0.61 (95% CI 0.16–0.85); p=0.013); and c) pulmonary vascular resistance (PVR) and maximum inspiratory mouth pressure (PImax) (n=11, r= -0.68 (95% CI -0.91– -0.14); p=0.021).
Peak oxygen uptake and maximum work rate at exercise were reduced. Mean 6-min walking distance (6MWD) was 303±134 m. At baseline, we found normal values for heart rate reserve (33±19 per min), breathing reserve (31±26%) and a RER of 0.97±0.12. PETCO2 was normal at rest and increased during exercise. PA–aO2was elevated (online supplementary table 3). Serum NT-proBNP levels were elevated, but not correlated to exercise capacity.
Maximum work rate was inversely correlated with mPAP, PVR (fig. 3) and PA–aO2 (-0.72; p=0.03) and V′E/V′CO2 (-0.87; p<0.01). 6MWD was negatively correlated with mPAP (fig. 3) and positively correlated to PETCO2 at the anaerobic threshold (0.83; p=0.04).

Correlations of a) work rate and mean pulmonary artery pressure (mPAP) (n=9, r= -0.71 (95% CI -0.94– -0.10); p=0.03); b) work rate and pulmonary vascular resistance (PVR) (n=9, r= -0.80 (95% CI -0.96– -0.79); p=0.01); and c) 6-min walking distance (6MWD) and mPAP (n=16, r= -0.62 (95% CI -0.85– -0.18); p=0.01).
Effect of noninvasive positive-pressure ventilation
NIPPV was performed as follows: inspiratory positive airway pressure 21±3 mbar, expiratory positive airway pressure 5.5±1 mbar, inspiratory time 1.4±0.2 s, frequency 20±3.5 min−1 and oxygen flow 2.9±1.9 L·min−1. Mean±sd duration of NIPPV was 5.4±2.6 h. table 1 shows the treatment effect of NIPPV at 3 month follow-up. Systolic, diastolic and mean PAP (-18 mmHg; p<0.001) and PVR (-199 mmHg; p<0.001) were decreased compared with pretreatment values (fig. 4); cardiac index and PAWP were not significantly changed. There was an improvement in exercise capacity, as indicated by a significant increase in maximum work rate (+18 W) and 6MWD (+66 m) (fig. 5).
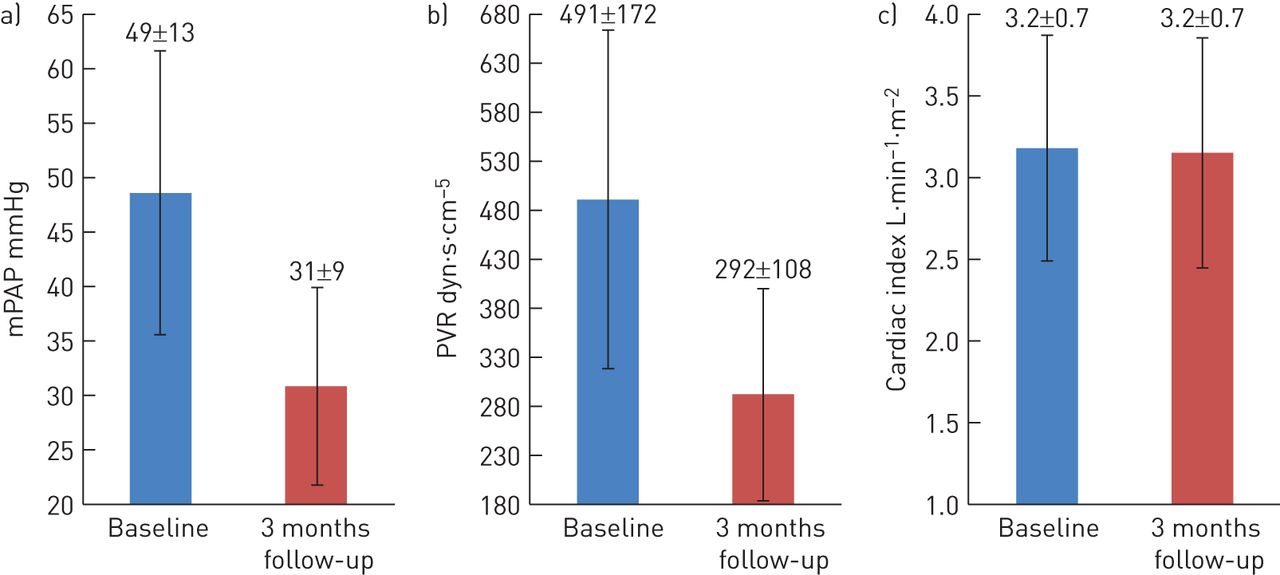
Changes in haemodynamic parameters after 3 months of noninvasive positive-pressure ventilation. a) Change in mean pulmonary artery pressure (mPAP), n=16; p<0.001. b) pulmonary vascular resistance (PVR), n=16; p<0.001. c) Change in cardiac index, n=15; p=0.807.

Changes to exercise capacity and N-terminal pro-brain natriuretic peptide (NT-proBNP) levels after 3 months of noninvasive positive-pressure ventilation. a) Change in 6-min walking distance (6MWD), n=16; p=0.008. b) Change in work rate, n=9; p=0.028. c) Change in NT-proBNP serum concentration, n=13; p=0.001.
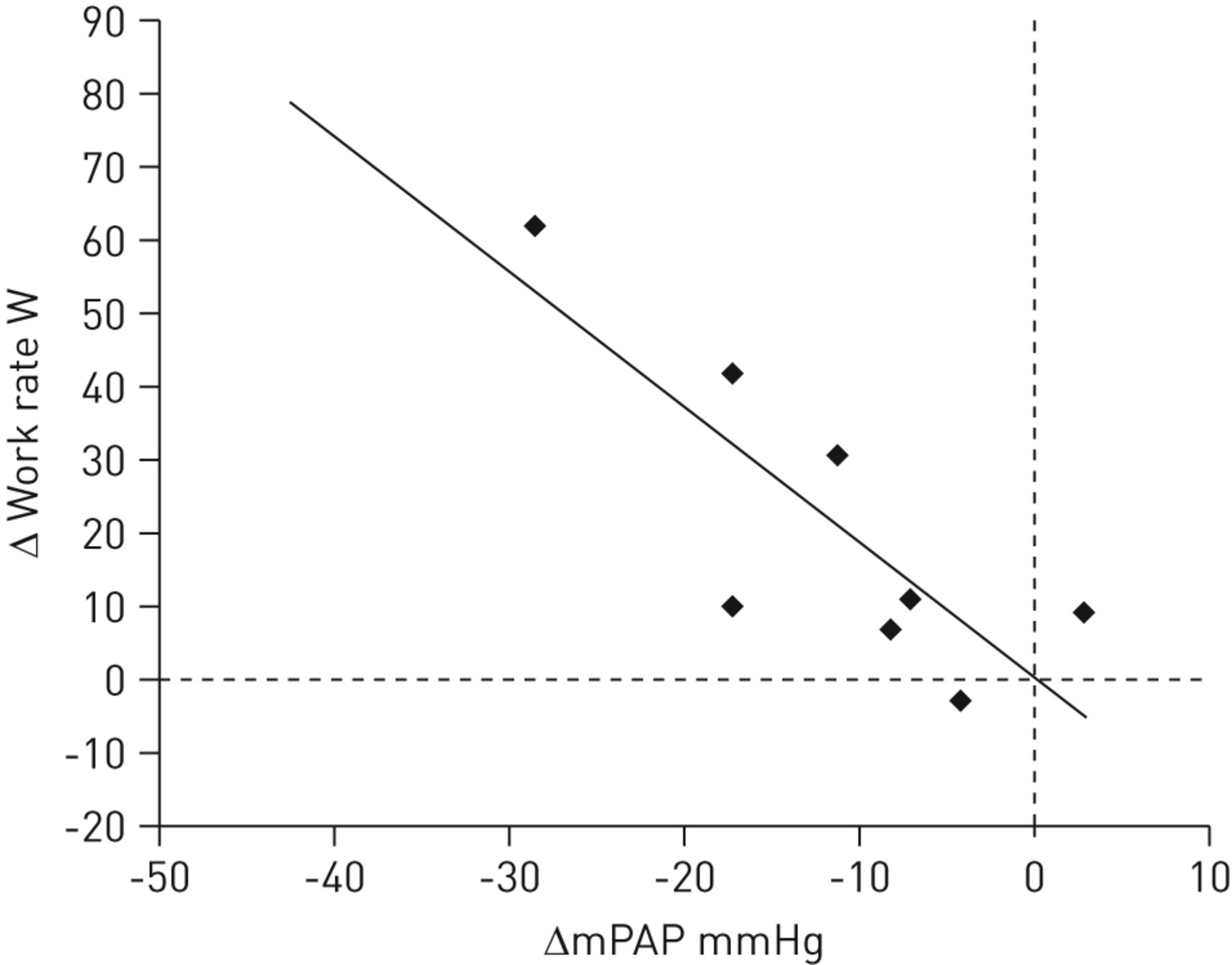
There was no change in systemic blood pressure, heart rate, left ventricular ejection fraction and E/E’ following NIPPV. The volume of the RA decreased from 97±57 mL to 65±34 mL (p=0.002), whereas the volume of the LA increased from 57±33 mL to 77±45 mL (p=0.002); the ratio of RA/LA volume decreased. There was no change in LV performance, measured by echocardiography, but RV function improved after 3 months of NIPPV. Consistent with the improved cardiac function, serum levels of NT-proBNP decreased significantly (table 1 and fig. 5). The haemodynamic improvement correlated positively with the increase in maximum work rate (fig. 6). Following NIPPV, FEV1 and VC increased, RV and intrathoracic gas volume decreased (not shown). O2 saturation and CO2 tension improved at night and daytime. There was no correlation between improved exercise capacity and changes in lung function (data not shown).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between change (Δ) in mean pulmonary artery pressure (mPAP) and change in maximum work rate after 3 months of noninvasive positive-pressure ventilation. n=8, R= -0.75 (95% CI -0.952– -0.096); p=0.031.
Discussion
To our knowledge, this is the first study to demonstrate a severe negative association between PH and exercise capacity in patients with alveolar hypoventilation and preserved cardiac index. The findings strongly support positive treatment effects of NIPPV on haemodynamics and functional capacity in these patients.
All patients showed hypoventilation with night-time and daytime hypercapnia and hypoxaemia. 12 patients were obese and fulfilled the criteria of OHS [33].
The mean mPAP of our cohort was much higher than previously reported [1, 5, 28]. These patients could represent a specific phenotype of severe PH associated with hypoventilation that is different from the majority of patients with hypoventilation. In obese patients, histological findings indicating PH seemed to be more frequent than the prevalence of PH reported in clinical studies [12]. Right heart catheterisation has not been routinely carried out in other studies dealing with PH and alveolar hypoventilation. Recently, Marik et al. [1] provided a detailed analysis of patients with OHS, but did not measure haemodynamics invasively. Since echocardiography is difficult to perform in obese patients, the noninvasive approach is prone to underestimate both prevalence and severity of PH in these patients. Moreover, the higher number of patients with severe PH in our study might be due, in part, to selection bias, as we studied patients who were referred with suspected PH for evaluation and treatment.
In an autopsy study, Haque et al. [12] found histological features of pulmonary arterial and pulmonary venous hypertension in 72% of obese patients compared with only 26% and 6% of nonobese controls. In our study, all but one patient underwent right heart catheterisation. Although mitral flow pattern might reflect a type 1 diastolic dysfunction, LA area was normal and LA volume was only slightly elevated [35]. Most of our patients had evidence for severe pre-capillary PH. Only three patients had PAWP >15 mmHg; however, pulmonary artery mean-to-capillary wedge pressure and pulmonary artery diastolic-to-capillary wedge pressure gradients were severely elevated, reflecting a relevant pre-capillary component of PH [36].
Systemic blood pressure at rest was normal and, despite severely elevated mPAP, patients responded with an increase in systolic blood pressure during exercise.
In patients with PAH and vasculopathy, cardiac index decreases with progressive disease [37]. In our cohort with severe PH and alveolar hypoventilation, cardiac index was normal or slightly elevated, which we interpret as a compensation for hypoventilation, ventilatory failure and hypercapnic hypoxia. Hypoventilation can occur in the context of a variety of disorders [5, 6, 28], but it is still unclear how hypoventilation and PH develop. In our study, the majority of patients did not have a sleep-related breathing disorder. Only two patients (AHI 30 events·h−1 and 60 events·h−1) presented with severe sleep apnoea syndrome, indicating that OHS is not inevitably associated with sleep apnoea.
Five patients had COPD alone, three more had both COPD and OHS, resulting in an overall reduction of FEV1 and VC in our cohort. Reduced lung volumes may have been affected by reduced strength of breathing. Compared with published data for healthy cohorts, the patients in our study had reduced maximum inspiratory mouth pressure as a sign of disturbed respiratory muscle strength and elevated respiratory load [30]. We assume that hypercapnia and hypoxaemia were a consequence of hypoventilation.
We found an inverse correlation between PVR and maximum inspiratory mouth pressure. Reduced strength of breathing might be a cofactor for hypoventilation, which was associated with PH in our patients. Conversely, it is conceivable that in patients with severe PH, respiratory muscle function is altered leading to reduced inspiratory mouth pressure as described by Meyer et al. [38].
The positive correlation of mPAP with BMI and night-time CO2tension, but not with oxygen tension, lung volumes or left ventricular function suggest that PH was driven by BMI and hypercapnic vasoconstriction.
Due to the preserved cardiac index, it was unclear whether PH has a functional impact on patients with alveolar hypoventilation. Our study subjects had a marked impairment of functional capacity as shown by reduced 6MWD, maximum work rate and maximum oxygen uptake. Since heart rate and breathing reserve were normal, our patients were not affected by cardiac or ventilatory limitation in the strictest sense. However, in patients with hypoventilation, breathing reserve has to be interpreted with caution. PA–aO2 was elevated, reflecting a limitation in gas exchange. We noticed high V′E/V′CO2 slope was associated with lower V′CO2 and RER, probably reflecting inefficient ventilation, which may have contributed to earlier termination of exercise and reflect poor respiratory function. We found a negative correlation between mPAP and work rate or 6MWD (fig. 4), indicating the importance of pulmonary haemodynamics for normal exercise capacity. However, low RER and increasing PETCO2 under exercise reveals that this specific cohort is different from patients with PAH, i.e. our observations concerning the physiology on exercise are compatible with respiratory rather than haemodynamic limitation.
Although correlation does not prove causality, the fact that NIPPV was associated with a significant decrease in mPAP, which then correlated with an increase in maximum work rate, suggests that PH can have a substantial functional impact on patients with severe PH due to alveolar hypoventilation despite having normal cardiac index.
The cardiopulmonary exercise testing was carried out by nine patients. This was not due to selection bias, but it merely reflects that many of these severely ill patients are unable to perform cardiopulmonary exercise testing due to morbid obesity or severity of disease.
Although our study population had normal cardiac index and normal systolic left ventricular function, the patients showed echocardiographic signs of right ventricular dysfunction and elevated serum NT-proBNP levels. NT-proBNP levels did not correlate with 6MWD, maximum work rate and cardiac index, but the levels still indicate a poor prognosis according to the published literature. Patients with obesity hypoventilation have increased mortality, as shown by several reports [1, 24, 39], and NT-proBNP levels seem to have a prognostic impact on PAH [40, 41]. This argues for a possible role of NT-proBNP serum levels as a biomarker for patients with alveolar hypoventilation and needs to be explored in a prospective trial.
To our knowledge, this is the first report about the effect of NIPPV on haemodynamics and exercise capacity in a cohort of obese patients. The high mortality rates of patients with OHS and PH underscore the need for early and effective treatment [1]. For PH secondary to structural lung disease and ventilatory disorders, current treatment guidelines recommend focusing on management of the underlying disease [13, 14]. Despite these recommendations, it is still unclear whether this will improve PH or not. In our cohort, after 3 months NIPPV therapy, PAP and PVR decreased significantly (p<0.001), without affecting cardiac index and PAWP.
Interestingly, following NIPPV, the RA volume decreased while LA volume increased. Not surprisingly, this resulted in a decrease of the RA/LA volume ratio. These findings suggest that NIPPV decreased RA pressure as a consequence of improving PAP and PVR. The reduction of the RA volume then allows improved filling of LA.
Moreover, we found an improvement in 6MWD and maximum work rate. Interestingly, decreased mPAP correlated with increased maximum work rate under exercise. There was no correlation to daytime and night-time blood gases, underscoring the relevance of pulmonary haemodynamics for exercise capacity in this patient group. Patients with poor compliance to NIPPV (using it on <50% of nights and for <4 h·night−1, n=5) did not show an improvement in PAP and functional capacity, further supporting an overall benefit of NIPPV in these patients.
Our study is limited by a relatively small number of subjects and the single-centre observational design. However, the robustness of the data, including the fact that PH was determined by right heart catheterisation, allows us to postulate that NIPPV can improve haemodynamics and functional capacity in patients with PH due to alveolar hypoventilation. It should be noted that the increase in 6MWD in our study was higher than treatment effects reported in studies with vasoactive drugs for PAH [42–45].
Conclusion
The present study shows an association between the elevated PAP and reduced exercise capacity of patients with alveolar hypoventilation and severe daytime PH despite preserved CI. In these patients the use of NIPPV was associated with improved daytime haemodynamics and functional capacity. A larger prospective study should be initiated to confirm these data.
Acknowledgments
We thank S. Karl (Institute of Mathematics, University of Würzburg, Würzburg, Germany) for statistical support during this study.
Footnotes
For editorial comments see page 12.
This article has supplementary material available from www.erj.ersjournals.com
Conflict of interest: Disclosures can be found alongside the online version of this article at www.erj.ersjournals.com
- Received September 17, 2012.
- Accepted May 14, 2013.
- ©ERS 2014
References










