





Abstract
Childhood tuberculosis (TB) poses a high risk for morbidity and death. This study describes the characteristics of childhood TB in Israel and examines treatment outcomes. Data sources were the National TB Registry and the National Civil Census.
Between 1999 and 2010, 416 children (aged <18 years) had TB, averaging 1.5 per 100 000 children (range 0.6–3.2), demonstrating a declining trend. The average proportion of all TB cases reported annually that were in children was 8.4% (range 5.4–11.8%). Most (n=320, 79%) of the childhood TB cases were pulmonary. TB rates were highest for the 0–4-year age group and lowest for the 10–14-year age group.
Of all childhood TB cases, 236 (56.7%) were born in countries with high prevalence of TB: 214 were Israeli citizens who were Ethiopian-born and 22 were non-Israeli citizens. The overall childhood TB incidence in 2010 was 1.05 cases per 100 000 children. The incidence of TB for Israeli-born children, children whose parents were Ethiopian-born and children of migrant workers was 0.55 per 100 000, 7.5 per 100 000 and 50–100 per 100 000, respectively. Cultures were taken from 60% of all childhood TB cases. Most children (97.8%) achieved treatment success, while three children (0.7%) died.
Overall, rates of childhood TB rates in Israel are decreasing. However, children of parents born in countries with a high prevalence of TB are still at high risk of developing TB. Bacteriological confirmation should be encouraged to improve control of childhood TB.
Nearly 1 million cases of childhood tuberculosis (TB) are reported globally each year [1], and it is estimated that children <15 years of age comprise 11% of all TB cases worldwide [2]. Childhood TB is characterised by greater risk of severe disease and death than adult TB, especially among toddlers aged <2 years [3]. However, the management of childhood TB is not a priority as it poses a lesser threat to public health than adult TB does.
The descriptive epidemiology of childhood TB is important in characterising the trends of the disease and defining children at high risk of developing severe disease. Moreover, TB in young children reflects recent infection rather than secondary reactivation. Therefore, childhood TB is a direct consequence of adult TB. This may be used as a sentinel indicator of transmission in the community and evaluation of the effectiveness of the national TB control programme [4].
Israel is a developed country with 7.7 million people, of whom nearly 2.5 million are not native born [5]. Its gross domestic product is US$29 800 per person [6], and it is part of the World Health Organization (WHO) European region. The total TB incidence in Israel in 2010 was 4.9 cases per 100 000 people [1]. Childhood TB in Israel between 1990 and 1999 comprised 11% of all cases reported, predominantly among foreign-born children [7].
TB is a reportable disease in Israel by law, and each notification sent to the Ministry of Health includes demographic, clinical and laboratory information [8]. The notifications are verified and followed up by both the regional and central levels of the Ministry of Health, and treatment results are recorded. The national TB and HIV registries are matched periodically, as both diseases are reported nominally to the central level.
The present study describes the demographic, clinical and microbiological characteristics of childhood TB in Israel, and examines the treatment outcomes for the last decade, following the establishment of the National TB Control Programme in 1997.
METHODS
For the purposes of this study, childhood TB included all reports of children aged <18 years who either had culture-confirmed disease due to Mycobacterium tuberculosis complex isolated from sputum, body fluids or tissue. Also included were children whose clinician considered therapy with a full course of anti-TB treatment when the child's clinical, histological or radiological signs and/or symptoms were compatible with the diagnosis of TB. Pulmonary TB (PTB) was classified as a case of M. tuberculosis affecting the lung parenchyma, the tracheobronchial tree or the larynx, with or without a diagnosis of extrapulmonary TB (EPTB). EPTB was a case of M. tuberculosis affecting any site other than PTB. For EPTB with multiple sites, the site other than peripheral lymph nodes was considered to be the principal site. Treatment outcomes were defined according to WHO [9], and patients who were cured or had completed the treatment were considered to be successful.
The data source was the National TB Registry, managed by the Dept of Tuberculosis and AIDS at the Ministry of Health. Patients were classified by their country of birth, nationality and time spent in Israel since their arrival, according to the Israeli Population Registry at the Ministry of the Interior. The denominators used to calculate TB rates by age, sex and country of origin were mid-year estimates derived from the official census [10].
Trend analysis was performed by Chi-squared test to yield the linear-by-linear association test using SPSS® programme 18.0 (SPSS, College Station, TX, USA). As this was routine epidemiological analysis on the non-nominal data within a standard public health database reporting system, ethical approval was not required.
RESULTS
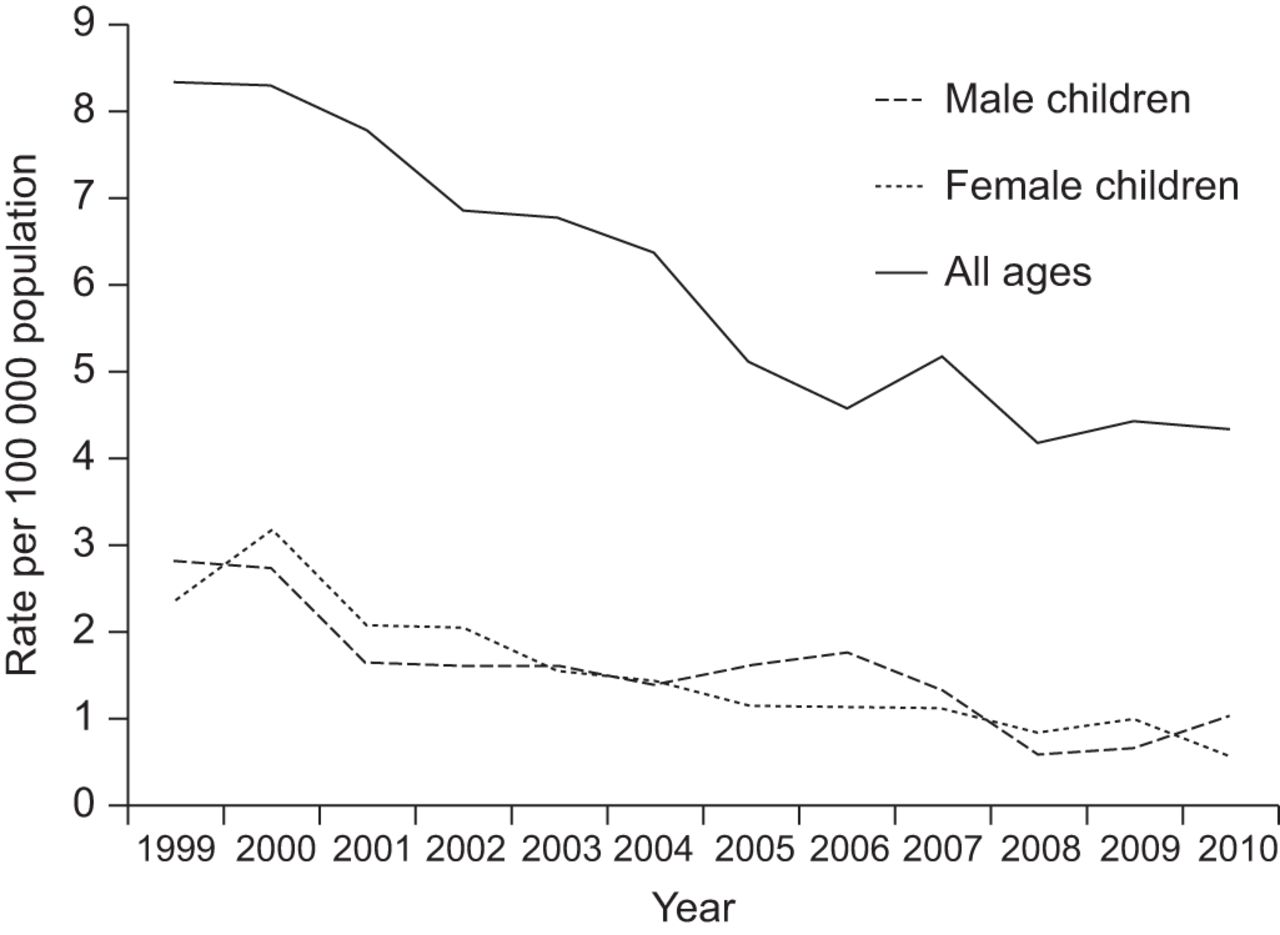
Between 1999 and 2010, 416 children in Israel aged <18 years were reported to have TB, in a decreasing trend from a peak of 3.2 per 100 000 children in the year 2000 to a nadir of 0.6 per 100 000 in 2010 (p=0.002). The average childhood TB rate for the entire study period was 1.5 per 100 000 (fig. 1). TB rates and trends were similar among male and female children (p=0.006 and p=0.003, respectively). During the study period, the average proportion of childhood TB of all cases reported each year in Israel was 8.4% (range 5.4–11.8%). Most (79%) of the children had PTB, while 21% had EPTB (table 1). The majority of the cases were in the 0–4-year age group, followed by the 5–9-year, 15–17-year and, finally, the 10–14-year age groups. TB-specific age-related rates were highest for the age groups 0–4 years and 15–17 years for most years, and lowest for the 10–14-year age group (p=0.03) (fig. 2).

Childhood and adult tuberculosis incidence in Israel, by sex, and comparison to the overall incidence rate, 1999–2010.

Rates of childhood tuberculosis in Israel, by age group, 1999–2010.
Of all children in the study period, 62.2% (260) were not Israeli born: 214 (51.5% of all children) were born in Ethiopia, 24 (5.8%) were born in the former Soviet Union and 22 (5.3%) were children of migrant workers who were not Israeli citizens (fig. 3). The number of new TB cases diagnosed annually in the migrant workers group is increasing, in contrast to all other groups classified by origin (p<0.001).

Country of birth and citizenship of childhood tuberculosis cases in Israel, 1999–2010.
In 2010, most (95.3%) of the 1 903 900 children who were Israeli citizens aged ≤18 years were Israeli born [10]. The overall annual incidence of childhood TB in Israel in 2010 was 1.05 cases per 100 000 children, and the incidence of childhood TB among Israeli-born children was 0.55 cases per 100 000 children. The incidence for Israeli-born children whose parents were not of Ethiopian origin was 0.33 per 100 000 children. If at least one of their parents was Ethiopian-born, the rate was then 7.5 cases per 100 000 children. The childhood TB incidence for Israeli-born Arabs was 0.44 cases per 100 000 children. The highest incidence of childhood TB was calculated for children of migrant workers, estimated to be 50–100 cases per 100 000 children, depending on the predicted size of the population of children of migrant workers.
When calculating the gap between the date of arrival in Israel and the date of reporting of disease, it was found that among children who migrated to Israel, disease notification decreased rapidly within their first 2 years in Israel. Of the 251 children who migrated to Israel and were diagnosed with TB during the study period, 146 (58.1%) developed childhood TB within the first year and 24 (9.6%) within the second year of their arrival (fig. 4).

Childhood tuberculosis in child immigrants in Israel, by years after arrival in Israel, 1999–2010.
PTB was reported in 328 (78.8%) cases and EPTB was diagnosed in 88 (21.2%) cases. The most common sites for EPTB were lymph nodes (n=55, 62.5%), followed by the pleura (n=9, 16.4%) and meninges of the brain (n=5, 5.7%) (fig. 5).

Site of extrapulmonary childhood tuberculosis (TB) in Israel, cumulative data, 1999–2010. n=88.
Samples were taken and cultured from 60% of all cases during the study period in a generally decreasing trend (p<0.001). Of all the cultures performed, 54.5% were found to be M. tuberculosis positive (fig. 6): 75.6% for PTB and 24.3% for EPTB. Drug susceptibility testing was performed on all culture-positive samples, and multidrug resistant (MDR) M. tuberculosis was reported sporadically, with no childhood case of MDR being reported in the last 3 years of the study.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mycobacterium tuberculosis culture results of all childhood tuberculosis (n=262) and multidrug resistant (MDR) cases (n=9), 1999–2010.
Average overall treatment success for the all children during the entire study period was 97.8%, ranging from 92.6% in 1999 to 100% in most other years. Death occurred in three cases (0.7%) due to tubercular meningitis, four (1.0%) failed to complete TB treatment and one (0.2%) was referred to another medical centre. Only one childhood TB case was HIV infected.
DISCUSSION
Childhood TB (<18 years) rates in Israeli citizens were lower than in adults and have declined significantly over the decade 1999–2010 across the sexes, all ages and countries of origins of the children or their parents. The only exceptions were children who were not Israeli citizens and children who were born to parents of Ethiopian origin. Both remain a public health concern.
The overall proportion of childhood TB in the entire TB caseload in Israel was higher in comparison to reports from other developed countries [11]–[13]. The reason is possibly associated with the relatively high birth rate in Israel (average of 3.03 children per mother, 2010 data [10]) and may also be related to the unique age distribution in Israel, where 28.4% of all citizens are in the 0–14-year age range; higher than the proportions published in other developed countries [14]. As children are mainly infected from adult cases, it is possible that more children in Israeli households are exposed to adults with active TB compared with European countries. Nevertheless, the overall rate of childhood TB per 100 000 Israeli children was lower than that reported in other developed countries [6], [15].
Disease rates were higher in the 0–4-year age group and lowest at ages 10–14 years, the so-called “safe school years” [16], and increased again in adolescence, corresponding with other publications [2], [4]. PTB in our study was the most common clinical manifestations of childhood TB, and infected lymph nodes accounted for the majority of EPTB cases, which is also in agreement with other publications [17].
In our study, the annual childhood TB rate in Israel was half the rate reported in the previous decade [7]. In addition, the ethnic composition of the affected children changed: the proportion of non-Israeli born children citizens to all childhood cases has reduced, while the proportions of Israeli-born and children of migrant workers have increased. The decline in the number of foreign-born child citizens reflects the decrease in Jewish migration to Israel during the first decade of the third millennium. The high rate of childhood TB in children whose parents were born in Ethiopia remains a public health concern, as it suggests recent and active transmission in this small community in Israel, comprising only ∼1.5% of the entire Israeli population [10]. The risk of TB transmission within members of a closed community of migrants lingers even in the second generation after parental migration. The high rate of TB incidence among children who migrated from Ethiopia or were born to Ethiopian parents is only partially responded to by the universal screening of all Jewish newcomers from Ethiopia [18]. Some researchers [19], [20] have suggested repeated screening procedures up to 2 years following arrival, as performed in the Netherlands [21] and Belgium [22]. However, as most cases in Israel are diagnosed within the first year following their arrival and special medical care is provided for those Ethiopian migrants during the first few years following their arrival [7], [21], the need for this intervention is questionable in the local Israeli setting.
Another area of concern is the increasing TB rate among children who are not Israeli citizens and were born to worker immigrants, similar to that reported from Europe [23] and the USA [24]. Not a single child from this group was reported in the decade previous to the study period [7], reflecting a changing pattern of labour migration to Israel, which includes more females and families in comparison to the period 1990–1999. According to the contact investigation records, which were performed by the health departments, most children were infected by their parents sharing the same household. Some were also involved in outbreaks, in line with publications from other countries [4], [11], [25]. As suggested by Sandgren et al. [23], for this particular epidemiological situation, the high rates in children who were not born in Israel do not represent the epidemiology of TB in Israel, but rather reflect local outbreaks or transmissions in communities populated by foreign-born individuals. Israel has become a desired destination for migrant workers since the early 1990s, and most of these migrant workers originate in countries with a high prevalence of TB.
It is estimated that ∼226 000 work migrants are presently resident in Israel with 5000–10 000 children [26]. Similarly to Israeli citizens, migrant workers are entitled to free medical diagnosis and treatment related to TB. The treatment costs for both documented and undocumented migrant workers are covered by the Ministry of Health. Documented migrant workers are screened for TB when applying for a work visa. Undocumented migrants, who are detained in correctional facilities for the misdemeanour of crossing the Israeli border without a valid visa, are screened for TB upon incarceration. It is recommended that health professionals use the opportunity of TB screening of migrants to inform them of the possibility that TB may develop in later stages. Migrant workers should also be notified that free TB treatment is available in all TB clinics in Israel and that care is disconnected from deportation regulations. In addition, migrants should be educated about the risk of transmission of M. tuberculosis to their children and its possible outcome.
A selective bacille Calmette–Guérin (BCG) vaccination strategy is followed in Israel, and includes children who have migrated from countries with high TB prevalence or whose parents migrated from such a country. This recommendation is supported by the high incidence of TB found in our study among children of migrants or children who themselves migrated from high prevalence countries. Conversely, the higher incidence of TB among those children may raise the question of the effectiveness of a BCG vaccination programme [15].
Diagnostic difficulties pose one of the greatest challenges for childhood TB management. TB is often not considered in the differential diagnosis of children, especially in settings where rates are low. TB can mimic many common childhood diseases, as well as pneumonia, generalised bacterial and viral infections, malnutrition and HIV. An additional challenge is the difficulty related to the collection of bacteriological samples, as children, especially toddlers and infants, may not produce sputum. Gastric aspiration, an alternative technique to collecting sputum that has been swallowed by the child, is an unpleasant procedure that requires hospital admission, trained personnel, overnight fasting for up to three consecutive nights and attention to infection control.
This might explain our study's sub-optimal 60% culture rate, which is, nevertheless, higher than the 42.3% reported from the WHO European region [23]. Furthermore, culture yield, when performed in Israel, had better results than those published elsewhere [11], [15], [27], [28]. Without a definitive TB diagnosis, treatment is often initiated on clinical judgment alone, aided by algorithms based on exposure history, clinical features, chest radiography and tuberculin tests [28], [29]. It is assumed that a fraction of all childhood TB is not diagnosed upon illness, but accidentally diagnosed at a later stage or resolved spontaneously and thus remains completely unnoticed [30]. Consequently, some cases of primary TB infection in children are therefore not reported at all.
Treatment success rates were high and achieved 100% in some years, higher than results from other developed countries [15], [23]. This represents the high level of care for children. The satisfactory treatment outcomes in Israel can be partially accounted for by the practice of administering directly observed therapy to all child patients, which cannot be supervised by the parents, but only by an alternative care-giver.
Childhood TB may be used as an indirect measure of the level of transmission in the community, and thus reflects the effectiveness of the National TB Control Programme [23]. The low TB rate in Israeli-born children, particularly those whose parents were not born in Ethiopia, probably describes more accurately the dynamic of TB epidemiology in Israel. Our results confirm that childhood TB is decreasing among all children's age groups, including the youngest. They also show the decline in the childhood versus adult incidence ratio, suggesting a lower transmission rate, in spite of a continuous inflow of migrants to Israel from countries with high TB prevalence.
This study is subject to some limitations. First, it relies on surveillance data, and therefore does not include important clinical data on the patients, such as date of BCG vaccination, the results of tuberculin skin testing and findings on chest radiography. However, the data are comprehensive and include the entire cohort of childhood cases reported in Israel within the study period. Secondly, this study lacks a reliable estimate of children who are not Israeli citizens and allows us only to estimate the rate rather than to make a more precise calculation.
In conclusion, this study describes an in-depth analysis of the epidemiological trends of childhood TB in Israel in the decade to 2010 and demonstrates decreasing overall rates. However, the Israeli National TB Programme has been facing new challenges since the beginning of the new millennium. Children who were born in countries with a high prevalence of TB, and those whose parents were born in those areas, are still at risk for acquiring TB, particularly the children of migrant workers. Treatment success is high, even though three children died during the study period. Finally, analysis of bacteriological confirmation of childhood TB should be encouraged in order to systematise appropriate treatment and improve childhood TB control.
Acknowledgments
We are grateful to M. Yehuda (Dept of Tuberculosis and AIDS, Ministry of Health, Jerusalem, Israel) for maintaining the records of the National TB Registry in updated and in exceptionally complete form, and to Z. Wiexelboim (Dept of Tuberculosis and AIDS, Ministry of Health, Jerusalem) for record linkage with the National HIV Registry. We wish to extend our appreciation to J. Brandt (Wolfson Medical Center, Jerusalem) for her English editing, word processing expertise and contributions. We also wish to thank the doctors, nurses, community workers and laboratory personnel, all of whom were responsible for the treatment success of these children with TB.
Footnotes
Statement of Interest
None declared.
- Received February 25, 2012.
- Accepted June 20, 2012.
- ©ERS 2013
REFERENCES










