





Abstract
It is not known whether vitamin D levels make a significant contribution to muscle dysfunction in chronic obstructive pulmonary disease (COPD).
In 104 COPD patients (mean±sd forced expiratory volume in 1 s 44±22 % predicted) and 100 age- and sex-matched controls, serum 25-hydroxyvitamin D (25(OH)D), 1,25-dihydroxyvitamin D (1,25(OH)2D) and parathyroid hormone (PTH) levels were measured and related to quadriceps strength and endurance. In a subset of 26 patients and 13 controls, quadriceps biopsy was performed and mRNA expression of myogenic regulatory factors (mrf) and fibre-specific myosin heavy chains (MHC) was determined.
COPD patients were weaker and less physically active than controls. 25(OH)D levels were similar in both groups (48.5±25.5 nmol·L−1 COPD versus 55.4±28.3 nmol·L−1 control, p=0.07) but PTH levels were significantly higher in patients (5.2±2.3 pmol·mL−1 versus 4.4±2.0 pmol·L−1, p=0.01). 1,25(OH)D was significantly correlated with strength in controls, but not in COPD patients and not with quadriceps endurance assessed using repetitive magnetic stimulation in COPD (n=35) or control (n=35) subjects. In controls, but not COPD patients, muscle biopsy analysis showed a negative relationship between 25(OH)D and MHCIIa expression (r2=0.5, p=0.01) and a positive relationship between mrf4 and MHCIIa expression (r2=0.5, p=0.009), and myogenic regulatory factor myf5 and MHCI expression (r2=0.72, p=0.004).
In contrast with healthy controls, muscle strength is not associated with vitamin D levels in COPD, which may represent vitamin D resistance.
Skeletal muscle weakness is an important complication of chronic obstructive pulmonary disease (COPD). Approximately 25% of patients with COPD develop significant weakness and it is associated with increased mortality[1, 2] Weakness is principally due to decreased activity, but other contributing factors, including systemic inflammation, oxidative stress and genetic susceptibility, have been implicated [3].
A number of studies have found an association between 25-hydroxyvitamin D (25(OH)D) and measures of muscle strength in healthy older people [4–6], and vitamin D supplementation decreases the risk of falls [7, 8]. Polymorphisms in the vitamin D receptor (VDR) have been shown to influence muscle strength in normal [9, 10] and COPD [11] populations. Patients with COPD have been shown to have an inadequate intake of vitamin D [12] and spend reduced time outdoors [13], both of which increase the risk of vitamin D deficiency. Janssens et al. [14] have shown that COPD patients have lower 25(OH)D levels than healthy smokers, and that 25(OH)D levels decreased with severity of disease. It is therefore plausible that vitamin D may play a role in the development of muscle weakness seen in COPD.
VDR knockout mice have been shown to have small and irregular muscle fibres with persistent expression of the myogenic regulatory factors (mrf) myf5 and myogenin [15]. In the same study, in vitro addition of 1,25-dihydroxyvitamin D (1,25(OH)2D) to myoblastic cell lines showed downregulation of these mrf.
The aim of the current study was to establish whether low vitamin D levels were associated with impaired skeletal muscle function in COPD patients. A significant association in COPD patients would increase the possibility that a supplementation strategy should be considered. Muscle function was measured using volitional and nonvolitional techniques. In a subset of patients, possible molecular mechanisms for the effects of vitamin D in muscle were investigated, focussing on the interaction between vitamin D with the expression of mrf and muscle-specific myosin heavy chain (MHC) expression.
SUBJECTS AND METHODS
Stable COPD outpatients and control subjects recruited by advertisement were studied. Subjects were excluded if they had significant comorbidities including unstable cardiovascular disease, malignancy or limiting musculoskeletal disorders. All subjects provided informed written consent and the study was approved by the Ethics Committee of the Royal Brompton Hospital, London, UK.
A systematic history including exacerbation rate and average daily dose (ADD) of oral corticosteroids in the preceding year was obtained. Vitamin D intake was assessed with a standardised recall questionnaire developed by ourselves, based on known dietary sources of vitamin D [16]. The Yale physical activity survey (YPAS) [17] and the St George's Respiratory Questionnaire were completed. Fat-free mass was measured with a Bodystat 1500 bioelectrical impedance device (Bodystat, Douglas, Isle of Man) using a disease-specific regression equation in COPD patients [18] and the device's internal algorithm for controls. Spirometry, plethysmographic lung volumes and gas transfer were obtained in COPD patients using a CompactLab system (Jaeger, Würzburg, Germany). Only spirometry was measured in control subjects.
104 patients with COPD and 100 control subjects were included in the study. Of these, 35 from each group had measurements of their quadriceps endurance taken and muscle biopsies were obtained from 26 patients and 13 controls. Further details of methods are included in the supplementary material.
Muscle strength and endurance
Quadriceps maximum voluntary contraction (QMVC), handgrip strength and sniff nasal inspiratory pressure (SNIP), as well as unpotentiated twitch quadriceps force (TwQ) in response to supramaximal magnetic femoral nerve stimulation, were measured as previously described [11, 19].
Quadriceps endurance was measured using repetitive magnetic stimulation with a Magstim Rapid 2 stimulator (Designworks, Windsor, UK) and a flexible mat coil placed over the body of the quadriceps [20]. Stimuli were delivered at a frequency of 30 Hz with a duty cycle of 0.4 (2 s on, 3 s off) for 60 trains of stimuli. The stimulator intensity was adjusted for each subject initially to generate 20% of their supine QMVC. Decay in force produced by consecutive trains was used as an index of endurance. Endurance curves were compared between COPD and control groups, and vitamin D-sufficient and -insufficient subjects within groups. Vitamin D insufficiency was defined as 25(OH)D levels of <75 nmol·L−1.
Serum measurements
Serum was stored and batch analysis of calcidiol (25(OH)D), calcitriol (1,25(OH)2D), high sensitivity C-reactive protein (hsCRP), interleukin (IL)-6, electrolytes and albumin was performed following study completion.
Muscle biopsy
Muscle biopsy samples were taken from the vastus lateralis of the dominant leg as described previously [20]. Real-time quantitative PCR analysis was performed for MHC1, MHCIIa, MHCIIx, the mrf myogenin, mrf4 and myf5 using the housekeeping gene human RPLPO for reference.
Statistical analysis
Descriptive statistics are reported as mean±sd or median (range). t-tests were used to compare means for parametric data and the Mann–Whitney test for nonparametric data. The Spearman rank test was used for correlations. Stepwise logistic regression was used to establish factors influencing muscle strength. Disease severity was considered in terms of % predicted; airflow obstruction (forced expiratory volume in 1 s), transfer factor of the lung for carbon monoxide (TL,CO) and gas trapping (residual volume (RV)/total lung capacity (TLC)). Regression with robust variances was used to compare endurance curves between COPD and control groups, and to compare vitamin D-sufficient and -insufficient subjects within groups. A p-value <0.05 was considered significant. Analysis was performed using SPSS for windows version 16.0 (SPSS Inc., Chicago, IL, USA) and STATA release 10.1 (StataCorp., College Station, TX, USA).
RESULTS
The groups were well matched for age and sex, but COPD patients were weaker and reported lower levels of physical activity (table 1). 15 patients had Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) stage 1 disease, 18 had GOLD stage 2, 39 had GOLD stage 3, and 32 had GOLD stage 4. The median ADD of prednisone, consumed mostly as short burst treatment for exacerbations, was 2 mg. Seven patients were taking regular low dose (<10 mg·day−1) oral prednisone. 27% of patients reported no exacerbations in the preceding year, with 22%, 14%, 11% and 26% having 1, 2, 3 or >4 exacerbations, respectively.
Vitamin D levels did not differ significantly between groups, but parathyroid hormone (PTH) levels were higher in the COPD group, and the ratio of both 25(OH)D and 1,25(OH)2D to PTH were significantly lower in the COPD group (table 2). Relationships between vitamin D levels and lung function are presented in the online supplementary material.
Muscle strength
In the COPD patients, 25(OH)D, 1,25(OH)2D and PTH levels were not associated with any measure of muscle strength (fig. 1), either independently or in stepwise analysis including potential confounding factors. QMVC was independently associated with sex, TL,CO (% predicted) and albumin. Handgrip strength was associated with sex and age. SNIP was associated with sex and RV/TLC (table 3).

Correlations between 1,25-dihydroxyvitamin D (1,25(OH)2D) and measures of muscle strength in the chronic obstructive pulmonary disease (COPD) and control groups. a) Quadriceps maximum voluntary contraction (QMVC): COPD r= -0.04, p=0.73; control r=0.2, p=0.05. b) Twitch quadriceps force (TwQ): COPD r= -0.04, p=0.76; control r=0.30, p=0.01. c) Handgrip strength: COPD r= -0.08, p=0.44; control r=0.31, p=0.003. d) Sniff nasal inspiratory pressure (SNIP): COPD r= -0.01, p=0.91; control r=0.28, p=0.01.
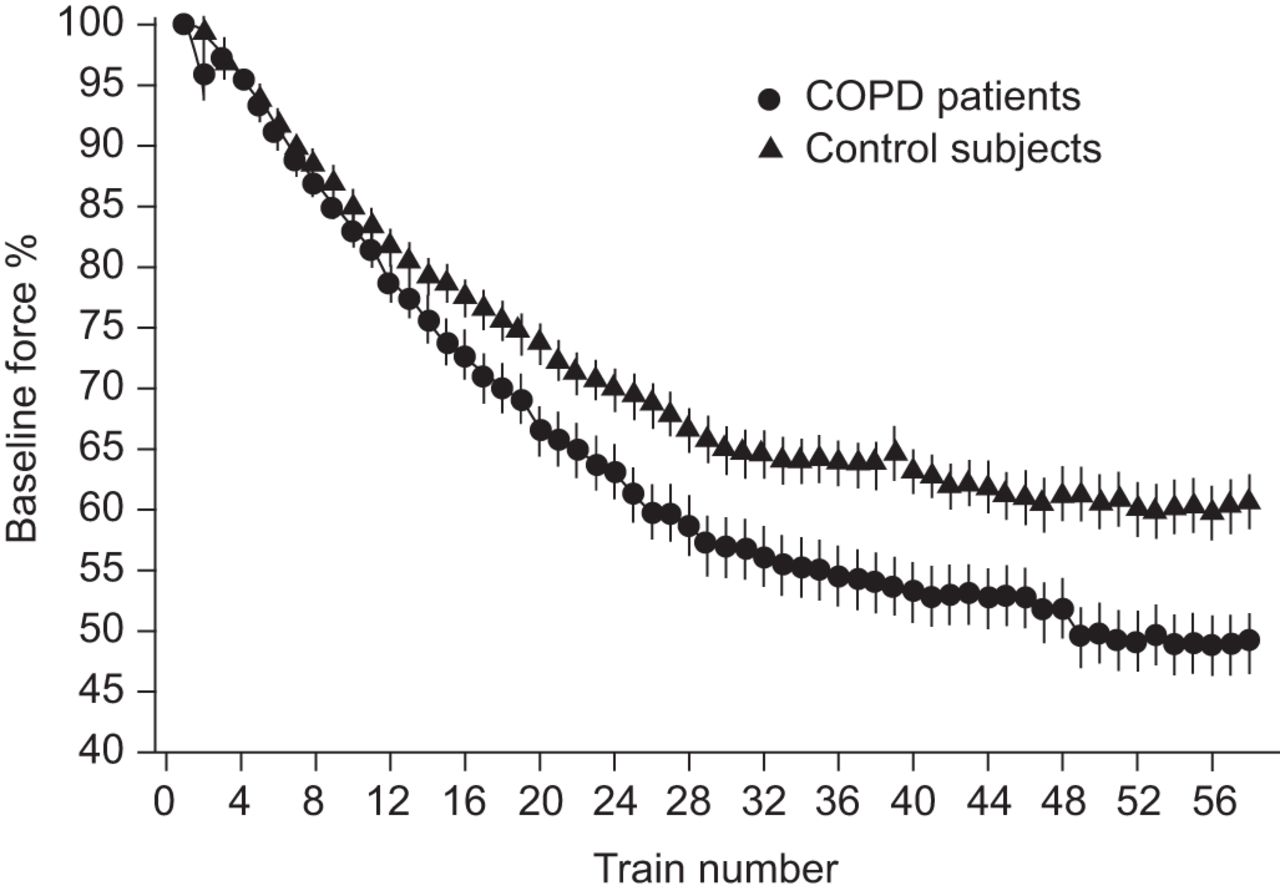
In the control group, 25(OH)D was significantly associated with TwQ (r=0.29, p=0.02), SNIP (r=0.22, p=0.04) and handgrip strength (r=0.20, p=0.05), but not with QMVC (r=0.18, p=0.07). 1,25(OH)2D was associated with QMVC (r=0.20, p=0.05), TwQ (r=0.30, p=0.01), SNIP (r=0.28, p=0.01) and handgrip (r=0.31, p=0.003) (fig. 1). After adjusting for confounding factors, 25(OH)D was not independently associated with any measure of muscle strength. However, 1,25(OH)2D was independently associated with handgrip strength and SNIP (table 4). Quadriceps endurance was significantly reduced in COPD patients (n=35) compared with controls (n=35) (Z=6.7%, 95% CI 2.1%–11.3%; p=0.004) (fig. 2) but did not differ between vitamin D-insufficient and -sufficient subjects in either study group.
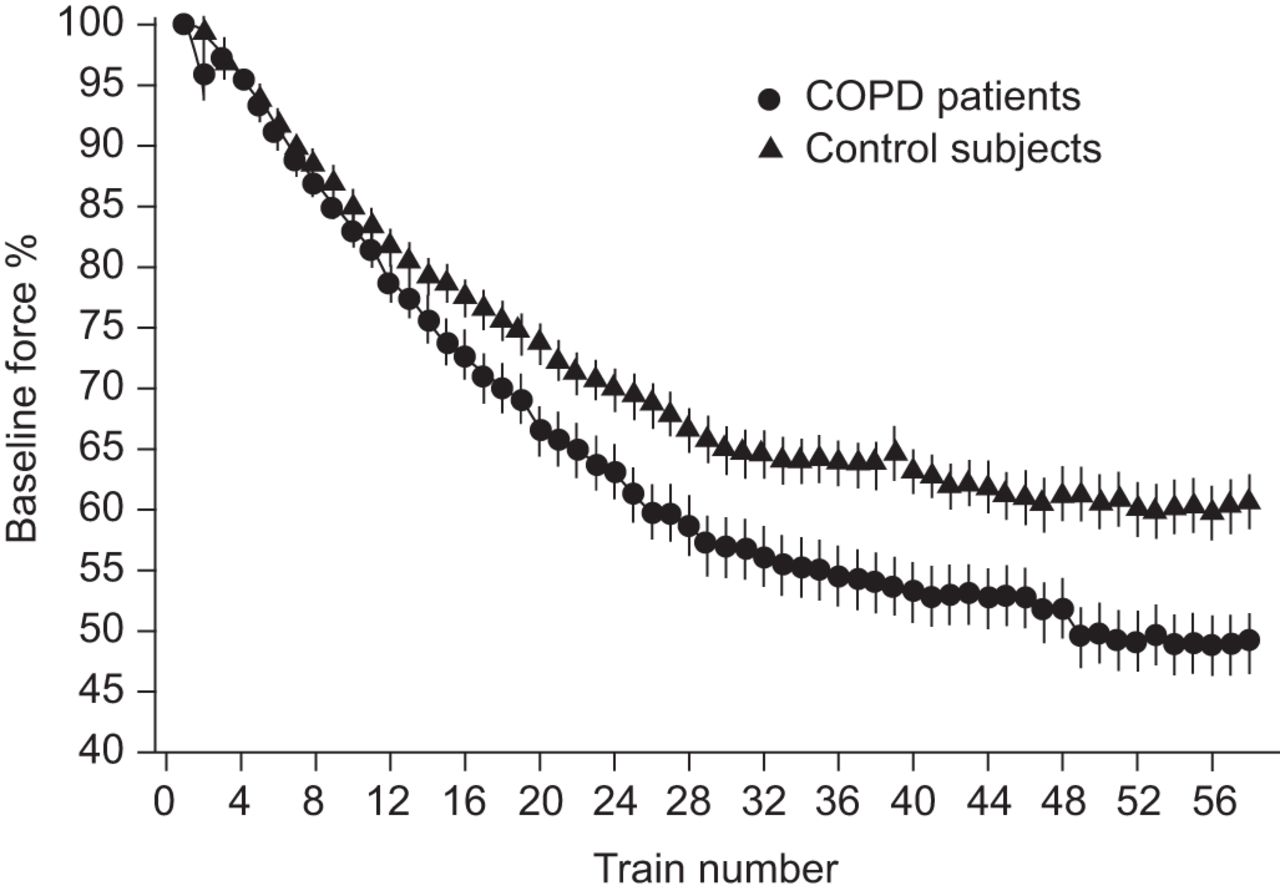
Quadriceps endurance in chronic obstructive pulmonary disease (COPD) patients and control subjects. Force declined more rapidly in COPD patients than controls in response to repetitive magnetic stimulation. Z=6.7 (95% CI 2.1–11.3%); p=0.004. Error bars represent the sem.
Factors affecting 25(OH)D levels
In a stepwise multivariate regression model involving all study subjects, ethnicity, age and daily vitamin D intake were independently associated with 25(OH)D levels (r2=0.11). Other factors not retained in the model were study group, number of pack-yrs, sex, body mass index, time of year measured, albumin, IL-6 or hsCRP. No association between inflammatory mediators and any measure of strength or body composition was noted (fig. S1).
54 (52%) COPD patients and 55 (55%) control subjects were taking some form of vitamin D supplement. Of those taking supplementation, a higher proportion of COPD subjects were taking vitamin D3 supplementation (46% in the COPD group versus 18% in the control group). A separate analysis of those subjects not taking supplements showed a significantly lower dietary vitamin D intake in COPD compared with control subjects (982±611 iu in COPD versus 1,287±658 iu in controls, p=0.01), and significantly lower 25(OH)D levels (COPD 41.5±24.6 nmol·L−1 versus controls 54.8±32.9 nmol·L−1, p=0.03). No measure of strength differed between patients who were or were not taking vitamin D supplements.
Analysis of 25(OH)D levels according to the time of year measured showed a different pattern in the COPD and control groups. While levels in subjects measured between November and February were similar in both groups, levels in subjects measured between March and October were significantly higher in the control group but not in the patients (fig. 3).

Variation in 25-hydroxyvitamin D (25(OH)D) level in chronic obstructive pulmonary disease (COPD) and control groups according to time of year measured. Data are presented as 95% CI. #: mean difference 5.6, p=0.31; ¶: mean difference 14.2, p=0.03. Horizontal line represent the mean.
Muscle biopsy analysis
Quadriceps muscle mRNA analysis was available for 26 COPD patients and 13 control subjects. MHC1 mRNA expression was lower in the COPD group compared with controls (4.19±0.41 versus 3.88±0.42, p=0.04), while expression of MHCIIa (COPD 2.98±0.67 and control 2.97±0.43, p=1.00) and MHCIIx (COPD 3.82±0.59 and control 3.78±0.52, p=0.82) was similar in both groups. No difference was seen in mRNA expression for any of the mrf between the COPD and control groups.
In the control group, MHCIIa was associated with both 25(OH)D and 1,25(OH)2D (r2=0.47, p=0.01 and r2=0.35, p=0.03; respectively), but there were no associations between MHC expression and vitamin D in COPD patients (fig. 4). In the control group, there was a trend for an association between 25(OH)D and the mrf as follows: myf5 (r2=0.38, p=0.08), mrf4 (r2=0.32, p=0.06) and myogenin (r2=0.30, p=0.07), but mRNA expression of mrf and 1,25(OH)2D was not correlated. No association was seen between mRNA expression of mrfs and either 25(OH)D or 1,25(OH)2D in COPD.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Associations between 25-hydroxyvitamin D (25(OH)D), myogenic regulatory factor (mrf) expression and fibre-type expression in chronic obstructive pulmonary disease (COPD) and control subjects between: a) 25(OH)D and myosin heavy chain (MHC)IIa expression (COPD r2=0.00, p=1.0; control r2=0.47, p=0.01); b) 25(OH)D and mrf4 expression (COPD r2=0.00, p=0.88; control r2=0.32, p=0.06); c) mrf4 expression and MHCIIa expression (COPD r2=0.00, p=1.0; control r2=0.52, p=0.009); and d) myogenic regulatory factor myf5 expression and MHCI expression (COPD r2=0.01, p=0.68; control r2=0.72, p=0.004).
In the control subjects, a number of associations were found between mrf and fibre type mRNA expression: mrf4 was most strongly associated with MHCIIa (r2=0.52, p=0.009), while myf5 was most strongly associated with MHCI (r2=0.72, p=0.004). In the COPD group, no association was found between either mrf4 or myf5 and any fibre type. In the subgroups undergoing biopsy, as in the main study groups, an association between 25(OH)D and muscle strength in control subjects but not COPD subjects was confirmed (COPD r2=0.07, p=0.22 and control r2=0.40, p=0.02, for handgrip strength). MHCIIa expression (but not MHC1 or MHCIIx expression) was associated with quadriceps strength in control, but not COPD, subjects (COPD r2=0.03, p=0.45 and control r2=0.36, p=0.03).
DISCUSSION
The main findings of the present study are that, first, there was no relationship between either 25(OH)D or 1,25(OH)2D and measures of muscle strength in subjects with COPD, although in the control group, 1,25(OH)2D was independently associated with measures of muscle strength. Secondly, quadriceps endurance was not associated with vitamin D levels in either group. Thirdly, the 25(OH)D/PTH ratio was significantly lower in COPD patients. In addition, in the muscle biopsy subgroup, there were two significant findings that have not been previously demonstrated. In control subjects, but not COPD patients, 25(OH)D was negatively associated with MHCIIa mRNA expression, and there were strongly positive associations between mrf4 and MHCIIa expression and myf5 and MHC1 expression.
Significance of findings
A number of studies have supported a link between vitamin D and skeletal muscle function [4–7, 9–11], but there is relatively little data about the mechanisms involved. Analysis of a small number of biopsies from people with osteomalacia has shown atrophy of type II muscle fibres with infiltration of fat, fibrosis and glycogen granules [21]. Two studies, both in elderly females, have looked at changes in muscle fibre morphology with vitamin D supplementation. Sorensen et al. [22] showed an increase in type IIa fibre diameter and percentage after 3–6 months of calcium and the vitamin D analogue 1 α-hydroxycholecalciferol. Sato et al. [23] gave 1,000 iu per day of vitamin D2 over 2 yrs and showed an increase in type II fibre diameter and percentage. VDR knockout mice have a 20% reduction in size of all fibre types compared with wild-type controls, and show abnormalities in mrf that are involved in growth and differentiation of myocytes [15]. Other demonstrated actions of 1,25(OH)2D in skeletal muscle include upregulation of calcium transport [24] and regulation of phospholipid metabolism [25]. Nongenomic or rapid effects of vitamin D have also been documented, including regulation of intracellular calcium [26] and activation of mitogen-activated protein kinase C pathways [27].
Vitamin D appears particularly to influence type II fibres and the quadriceps in COPD patients shows an increase in the proportion of type IIa fibres and a reduction in their cross-sectional area. Therefore, the complete lack of association between vitamin D and muscle strength in the COPD population is unexpected. Quadriceps endurance was significantly reduced in COPD patients, but in contrast to strength, which was influenced by vitamin D level in controls, there was no effect of vitamin D on endurance observed in either group. This may be because the predominant effect of vitamin D is on type II fibres, although studies in VDR knockout mice suggest otherwise [15].
Only one cross-sectional study [28] has looked at 25(OH)D levels and handgrip strength in patients with advanced lung disease referred for lung transplant, of whom ∼50% had COPD. This study found no association between the two parameters but, in COPD muscle, weakness occurs predominantly in the muscles of locomotion [28].
One explanation for this lack of effect of vitamin D in COPD is that it is masked by other processes, or simply that the magnitude of effect is small in comparison with other phenotypic modulators of muscle strength. However, even when we adjusted for factors thought to drive muscle atrophy, including physical activity level, disease severity and exacerbation rate, there was still no relationship.
An alternative hypothesis is that there is resistance to the actions of vitamin D in COPD patients. Although no significant difference was seen between the levels of 25(OH) or 1,25(OH)2D in our study groups, PTH was significantly higher and the 25(OH)D/PTH ratio significantly lower in COPD patients. PTH maintains serum calcium in the normal range through actions on the kidneys, bone and vitamin D, and is tightly regulated by 1,25(OH)2D. PTH levels increase with age. This is thought to reflect decreased calcium absorption and it has been hypothesised that post-menopausal females have resistance to 1,25(OH)D in the gut, although this has not been confirmed [29]. The raised PTH in our COPD group suggests that there may also be increased resistance to vitamin D in the gut with less calcium absorption, despite similar levels of 25(OH)D. This process could drive increased bone resorption and may explain why COPD patients have a high risk of osteoporosis. There are a number of potential mechanisms through which vitamin D resistance could occur. 1α-hydroxylase (CYP27B1) converts 25(OH)D to 1,25(OH)2D, which binds to VDRs present in the target organ. The VDR then forms a heterodimer with retinoic acid receptor before it can bind to DNA and effect a response via gene transcription. The VDR is also present in the cytoplasm and has been shown to have nongenomic effects. Decreased activity of CYP27B1, or decreased expression or inappropriate activity of the VDR could result in resistance. The levels of 1,25(OH)2D were similar in both groups, which suggests that any mechanism of resistance would involve the VDR and its interactions. Potential influences on the vitamin D pathway in skeletal muscle in COPD include the presence of inflammation, oxidative stress, reduced capillarity, muscle hypoxia and physical inactivity. It is noteworthy that, in our study, we found no relationship between either systemic inflammation and vitamin D levels or between systemic inflammation and any measure of muscle function.
COPD has been hypothesised to be a disease of ageing [30], and evidence is accumulating to support this, with demonstration of senescence markers in the lungs of COPD patients [31] and the finding of a positive association between telomere length and lung function in COPD [32]. Vitamin D also controls many genes involved in ageing [33], and higher vitamin D levels have been associated with longer telomere length, even after adjustment for age and other confounding factors [34]. VDR concentrations in muscle [35] and duodenum [36] have been shown to decrease with age and it is possible that decreased concentrations may be present in COPD patients causing a relative resistance to 1,25(OH)2D, which may be the link to accelerated ageing in COPD. In our muscle samples, we could not measure VDR protein levels and were therefore unable to explore this hypothesis further.
Another potential explanation for the difference seen in PTH levels between the two groups could be the presence of magnesium deficiency, as this can cause a blunted PTH response to low vitamin D levels [37] with subsequent reduced bone turnover. Although magnesium is predominantly an intracellular ion, serum concentrations did not differ between groups, making this unlikely to be a significant factor.
The results of the muscle biopsy substudy support the presence of vitamin D resistance, as associations seen at the molecular level in normal subjects were absent in COPD subjects. The mrf have been shown to be influenced by 1,25(OH)2D in vitro, and are persistently upregulated in VDR knockout mice (this is more fully referenced in the online supplementary material) [15]. mrfs have been extensively studied in embryogenesis and in cell culture models, where they have been shown to play an important role in skeletal muscle development. MyoD and myf5 commit stem cells to a myogenic lineage while myogenin and mrf4 stimulate the transition to multinucleated myofibres. However, less is known of their function in adult muscle. mrf4 expression does persist into adult life, while the other mrfs decrease shortly after birth and subsequently increase with ageing and in disease states. MyoD and myogenin mRNA have been shown to increase after resistance exercise training in both young and old people, while myf5 mRNA increases only in the young.
While they clearly have an ongoing role in adult muscle that has yet to be clearly elucidated, the present results suggest that mrf4 and myf5 may be important regulators of muscle fibre type. One study in adult rats has demonstrated high levels of myogenin mRNA in muscles that predominantly consist of slow fibres with high levels of myoD mRNA in those that consist predominantly of fast fibres. However, levels of mrf4 mRNA did not differ between muscles, while myf5 mRNA was virtually undetectable. Our findings are supported by another study looking at promoter/reporter gene constructs of mrf4, which has shown a region that promotes mrf4 specifically in fast muscle fibres.
Study limitations
This is a large cross-sectional study with a well-phenotyped cohort of COPD patients and a control group matched for age and sex. However, as with any cross-sectional study, it is only possible to look for significant associations and we are not able to establish cause and effect relationships. The population was predominantly Caucasian living in the UK and results must be applied with caution to other populations. One limitation of the study may be the use of the YPAS as a measure of physical activity rather than direct measurement. This is a recall questionnaire and therefore has inherent problems associated with it. However, it is a useful tool for comparing populations, it has been validated in older people, the physical activity score has been shown to correlate with maximal oxygen uptake, and discriminated between patients and controls in the present study [17]. A limitation is that biopsies were performed only in a proportion of subjects; however, the relationships between vitamin D levels and strength seen in the subgroups matched those in the whole population, suggesting that they were representative.
Conclusion
The relationship between vitamin D and muscle strength observed in normal subjects is not present in COPD patients, despite a similar range of levels. We have also demonstrated an association between certain myogenic regulatory factors and fibre type expression in normal subjects but not COPD patients. These results are surprising and raise the possibility of vitamin D resistance in COPD. Further molecular studies investigating VDR expression and post-transcriptional effects of vitamin D in skeletal muscle of COPD patients are required to explore this hypothesis further. Several prospective trials of vitamin D supplementation are underway to establish its impact on exacerbations in COPD, but it may be that higher doses of supplementation or even nonhypercalcaemic vitamin D analogues may be necessary to impact on skeletal muscle impairment in COPD patients.
Acknowledgments
We would like to thank the patients and healthy subjects who participated in this study for their time and cooperation. We acknowledge the assistance of the staff in the Lung Function Laboratory of the Royal Brompton Hospital and D. Hosking (David Evans Research Centre, Nottingham University Hospitals, Nottingham, UK) for his helpful comments on our manuscript.
Footnotes
This article has supplementary material available from www.erj.ersjournals.com
Support Statement
This study was funded by a grant from The Moulton Foundation and supported by the NIHR Respiratory Disease Biomedical Research Unit at the Royal Brompton and Harefield NHS Foundation Trust and Imperial College London (London, UK) who part fund M.I. Polkey's salary.
Statement of Interest
None declared.
- Received March 12, 2012.
- Accepted April 22, 2012.
- ©ERS 2013
REFERENCES










