





Abstract
We aimed to study the associations between the household use of cleaning sprays and asthma symptoms and control of asthma, in females from the Epidemiological Study on the Genetics and Environment of Asthma (EGEA).
Data were available for 683 females (mean age 44 yrs, 55% never smokers, 439 without asthma and 244 with current asthma). Both domestic exposures and asthma phenotypes (asthma symptom score, current asthma, poorly-controlled asthma (56%)) were evaluated as previously described in the European Community Respiratory Health Survey. Associations between the use of sprays and asthma phenotypes were evaluated using logistic and nominal regressions, adjusted for age, smoking, body mass index and occupational exposures.
Significant associations were observed between the weekly use of at least two types of sprays and a high asthma symptom score (OR (95% CI) 2.50 (1.54–4.03)) compared with a null score. Consistent results were observed for current asthma (1.67 (1.08–2.56)) and poorly-controlled asthma (2.05 (1.25–3.35)) compared with females without asthma. The association for current asthma was higher in females not reporting avoidance of polluted places (2.12 (1.27–3.54)) than in those reporting such avoidance (0.99 (0.53–1.85)).
The common use of household cleaning sprays is positively associated with a high asthma symptom score, current asthma and poorly-controlled asthma in females.
Previous studies have reported an excess risk for asthma in cleaners working in offices, hospitals or employed in private houses [1]. Results are consistent with an effect of cleaning agents both in the aggravation and new onset of asthma [1, 2]. Household cleaning substances are classified in the top five substances most frequently involved in exposure complaints in the 2009 report of the American National Poison Data System [3]. Bello et al. [4], who studied detailed tasks among hospital cleaners, classified the use of cleaning sprays as high risk for inhalation exposure. The use of cleaning products in spray form, at work and at home, may be an important risk factor for asthma [1, 5, 6]. One study has reported a dose–response relationship between the frequency of use and number of cleaning sprays used at home and asthma incidence [6].
Exposure to cleaning agents may represent an important public health issue, especially in females. Involvement in domestic tasks and home cleaning is a sex-related behaviour [7, 8]. Uncontrolled asthma was more frequent in females than in males [9], and domestic exposures might partly explain gender differences in asthma control [10]. Both at work and at home, females are likely to be at high risk, based on the potential deleterious effect of cleaning products, including those in spray form [11]. Other studies are necessary to confirm this deleterious role of household cleaning sprays on asthma activity and clinical expression of the disease.
The “healthy worker effect” is an important bias in occupational asthma [12, 13]. For domestic exposures, we hypothesise that a similar phenomenon of selection might be present but has not yet been studied. A “healthy home-cleaning effect” would be induced by the fact that people with cleaning task-related asthma symptoms may modify their behaviour to reduce the use of cleaning products, sprays or tasks.
In the Epidemiological Study on the Genetics and Environment of Asthma (EGEA), a detailed questionnaire regarding current domestic tasks was used along with precise asthma phenotypes. The aim of the present analysis was to assess, in females from the EGEA study, the associations between home cleaning, particularly the use of household cleaning sprays, and asthma activity. Specific hypotheses were: the use of household sprays as a risk factor for 1) poorly-controlled asthma, 2) a high asthma symptom score and 3) a potential “healthy home-cleaning effect”, evaluated by the avoidance of polluted places, in the association between domestic exposures and asthma.
MATERIAL AND METHODS
Population
EGEA is a cohort study based on an initial group of patients with asthma recruited (1991–1995) in chest clinics (probands, n=388) along with their first-degree relatives (n=1,244) and a group of population-based subjects (n=415). At the second survey (1,601 subjects with detailed questionnaires), detailed phenotyping was performed with lung function tests including methacholine challenge, skin prick tests (SPT) to 12 aeroallergens and total serum immunoglobulin (Ig)E (see flow chart and descriptive data in the online supplementary material) [9, 14]. The analysis is based on 683 females examined at the second survey, for whom detailed information regarding domestic exposures, in particular to sprays, was collected in 2003–2007 (244 with current asthma and 439 without asthma, with detailed phenotyping). The main analysis was focused on females, because few males used cleaning products and no associations were observed in males (online supplementary material).
Asthma and related phenotypes
Based on five asthma symptoms over the previous 12 months (wheezy breathlessness, woken up by chest tightness or by an attack of shortness of breath, attack of shortness of breath at rest or after exercise) the asthma symptom score was computed as previously proposed [15, 16]. A high score was defined by two or more symptoms. As in the European Community Respiratory Health Survey (ECRHS) [17, 18], current asthma referred to the report of asthma attacks or asthma treatment or asthma-like symptoms in the past 12 months [9]. Asthma control was assessed as described by Cazzoletti et al. [17] and already used in EGEA by Siroux et al. [9], based on the Global Initiative for Asthma (GINA) 2006–2010 guidelines combining diurnal and nocturnal respiratory symptoms, asthma attacks, lung function, hospitalisation for asthma and the use of reliever medication. Females with current asthma were classified as poorly controlled (i.e. uncontrolled or partly controlled) or controlled. Sensitivity analyses were performed for the following asthma sub-phenotypes: asthma severity, low lung function (forced expiratory volume in 1 s (FEV1) <80% predicted), bronchial hyperresponsiveness (BHR) (provocative dose causing a 20% fall in FEV1 <4 mg methacholine), positive skin prick tests (SPT+, any of 12 allergens), high total IgE (≥100 IU·mL−1) and blood eosinophilia (≥250 cells·mm−3). See online supplementary material for more details.
Assessment of exposure
Current domestic exposures (last 12 months) were recorded as in ECRHS [6], based on 24 domestic exposure variables including nine cleaning tasks and 15 cleaning agents (see online supplementary material). Exposure to home cleaning referred to the report of this task at least weekly as in Zock et al. [6]. Exposure to sprays was defined by the exposure to any of the eight types of sprays (furniture, glass-cleaning, carpet, mopping the floor, oven, ironing, air-refreshing, other use) at least once a week. Detailed analyses of those exposed (weekly) to two types of sprays were performed.
For a more comprehensive approach, domestic exposure patterns were defined through principal component analysis (PCA) based on the 24 exposure variables. PCA evidenced three domestic exposure patterns entitled “essential tasks”, “domestic wizard”, and “chemical products” (table 1).
In order to assess a potential “healthy home-cleaning effect”, we analysed a proxy of avoidance of cleaning products, i.e. “avoidance of polluted places”, assessed by four questions on the activity limitation domain (passive smoking, dust, pollution, perfume/odour) from the Asthma Quality-of-Life Questionnaire [19]. Participants with asthma were classified as “without avoidance of polluted places” if, from the seven-point scale of each of the questions, they reported “none of the time”, “hardly/any of the time” or “a little of the time”. Working as a cleaner or occupationally exposed to cleaning agents, assessed through an asthma job exposure matrix with an expert re-evaluation step [13, 20], was used for sensitivity analysis.
Statistical analysis
Associations between reported domestic exposures, exposure patterns and asthma-related phenotypes were evaluated using logistic regression, taking into account the familial structure of the data (Genmod; SAS, Cary, NC, USA) and nominal logistic regression analyses. In all the analyses on asthma sub-phenotypes, the females with a given asthma phenotype were compared to those without asthma. All analyses were adjusted for age, smoking status, body mass index (BMI) and occupational exposure to asthmogens.
RESULTS
The mean age of the females was 44 yrs, 55% were never smokers, and 36% had current asthma, of which 56% was poorly controlled asthma (table 2). Home cleaning, but not spray use, was significantly associated with age, BMI and diploma level, but not with other covariates.
Most of the females with asthma had childhood-onset asthma (<16 yrs). As expected, females with asthma had significantly more frequently low FEV1, BHR and SPT+, and high IgE and eosinophilia compared with females without asthma (online supplementary table E1).
Avoidance of polluted places
Among the females with current asthma (n=244), 83 avoided passive smoking, dust, pollution, and perfume/odours (60, 41, 24 and 24, respectively), half of them for at least two reasons. The avoidance of polluted places was not significantly associated with home cleaning but was significantly associated with the use of sprays (table 2). The subjects who reported avoiding exposure to inhaled irritants also used sprays weekly less frequently than those who did not avoid polluted places (39% versus 57%). A significantly higher prevalence of avoidance of polluted places was observed in non-users of sprays (44% versus 27% in weekly users, p=0.01), in non-smokers (41% versus 14% in current smokers, p=0.001) and in females with adult-onset asthma (44% in adult-onset versus 31% in childhood-onset asthma, p=0.04). No associations were observed between avoidance of polluted places and atopy and diploma level.
Home cleaning
Using self-report assessment of home cleaning, no significant associations were observed (OR (95% CI) 1.38 (0.91–2.11)) with the asthma symptom score in univariate analysis. After adjustment for age, smoking habits, BMI, and occupational exposure, home cleaning (1.85 (1.16–2.94)) was significantly related to a high asthma symptom score (table 3).
No significant associations were observed between home cleaning and current asthma or asthma control (table 3), nor with any of the other studied asthma phenotypes (data not shown). Using PCA exposure assessment, “essential tasks” (second tertile, table 3) were positively and significantly associated with a high asthma symptom score and poorly controlled asthma. A significant negative association was observed for moderate exposure to the category of “domestic wizard” and current asthma (OR 0.61 (0.39–0.97)), whereas no associations were observed for the third derived factor.
Spray use
The use of at least two types of sprays per week was significantly associated with a high asthma symptom score before (2.68 (1.70–4.24)) and after adjustment (2.50 (1.54–4.03)) (table 3). For the use of at least two types of sprays, there was a significant trend according to the frequency of use (p-value for trend=0.0002) (table 4). Exclusion of the 40 females occupationally exposed to cleaning agents led to a significant association of similar magnitude (2.47 (1.50–4.07)). Odds ratios were close to 1 for participants with only one symptom. Stronger significant associations were observed between both the use of one and at least two types of sprays and a high asthma symptom score (3.20 (1.48–6.91) and 4.20 (1.78–9.93), respectively) when the analyses were performed only in females without asthma (n=54 females with a high symptom score and without asthma).
For current asthma, no significant associations were observed with the use of one spray weekly with an OR lower than one (0.68 (0.44–1.04)), whereas a significant association was observed for the weekly use of at least two types of sprays (1.67 (1.08–2.56)). The association was of borderline significance (1.50 (0.97–2.32), p=0.07) after exclusion of the females occupationally exposed.
For asthma control, similar results were observed: odds ratios were higher for poorly controlled asthma (table 3) and associations remained significant after the exclusion of females occupationally exposed, with similar magnitudes.
Analyses were also performed using the three most commonly used sprays. Significant associations were observed between exposure to furniture (n=92) and air refreshing (n=160) sprays and a high symptom score (2.06 (1.20–3.55) and 1.77 (1.14–2.73), respectively), and between glass cleaning sprays (n=161) and current asthma (1.46 (1.00–2.13)). No significant associations were observed with asthma control.
Selection bias
To evaluate selection bias, we classified females with asthma according to “avoidance of a polluted place” (yes/no) (table 5). For current asthma, ORs were higher in females without avoidance of polluted places than in those with avoidance, especially for the use of at least two types of sprays (ORs 2.12 (1.27–3.54) versus 0.99 (0.53–1.85)). A significant negative association was observed for the use of only one spray per week in females with current asthma and with an avoidance of polluted places compared with females without asthma (OR 0.38 (0.19–0.74)). Similar trends were observed for asthma control (table 4).
Spray use and asthma sub-phenotypes
Sensitivity analyses regarding the associations between the use of at least two types of sprays and asthma sub-phenotypes are presented in figures 1 and 2. Compared with the odds ratio for current asthma (OR 1.67 (1.08–2.56)), the odds ratios were higher for asthma with low FEV1 (2.67 (1.31–5.48)), for severe asthma (2.20 (1.20–4.04)), for asthma with high IgE (2.11 (1.25–3.57)), for asthma with a high symptom score (2.04 (1.30–3.22)) and for non-eosinophilic asthma (1.88 (1.16–3.06)). The weekly use of at least two types of sprays was significantly related to SPT+ asthma (1.66 (1.03–2.68)), with an odds ratio of similar magnitude for SPT- asthma (1.63 (0.78–3.39)), compared with females without asthma. Whatever the neutrophil levels, similar odds ratios were observed with the weekly use of at least two sprays (1.66 (1.05–2.65), 1.54 (0.75–3.13), for ≤5,000 cells·mm−3 and >5,000 cells·mm−3, respectively).
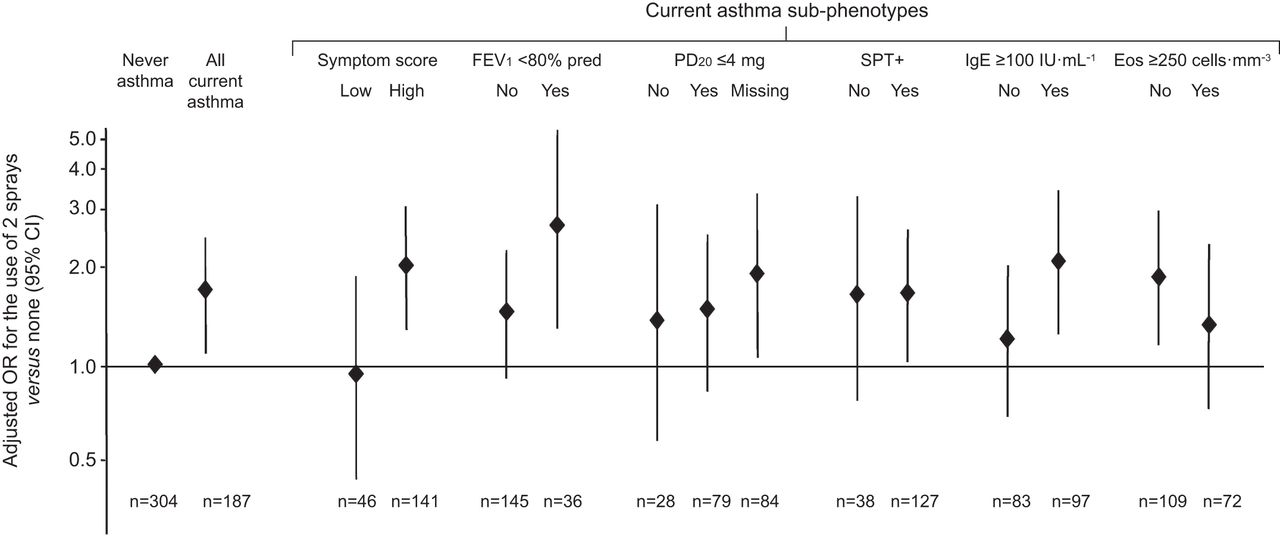
Association of domestic exposures to two sprays with current asthma sub-phenotypes. Odds ratios (95% CI), expressed with “never asthma” as reference, were adjusted for age, smoking habits, body mass index and occupational exposure to asthmogens. Symptom score was defined following Sunyer et al. [15] and Pekkanen et al. [16]. Low/high symptom scores referred to score <2/≥2 asthma-like symptoms (out of a maximum of five, see methods), respectively. Per cent predicted forced expiratory volume in 1 s (FEV1) was based on values from Stanojevic et al. [21]. Missing data for provocative dose causing a 20% fall in FEV1 (PD20) to methacholine challenge were mostly due to low FEV1 values (challenge not performed when FEV1 % pred <80%). Skin prick test positivity (SPT+) refers to a wheal >3 mm for any of 12 allergens. Blood eosinophilia (Eos) (≥250 cells·mm−3) was defined as previously reported in the Epidemiological Study on the Genetics and Environment of Asthma by Nadif et al. [22].

{kind=link}
{kind=link}
Association of domestic exposures to ≥2 sprays with current asthma sub-phenotypes, defined by composite scores (severity and control). Odds ratios (95% CI), expressed with “never asthma” as reference, were adjusted for age, smoking habits, body mass index and occupational exposure to asthmogens. Asthma severity was assessed, as previously described in detail by de Marco et al. [18], following the 2002–2006 Global Initiative for Asthma (GINA) principles, combining clinical features of the patients and asthma treatment level at the time of examination. Asthma control was assessed, as described by Cazzoletti et al. [17] and already used in the Epidemiological Study on the Genetics and Environment of Asthma by Siroux et al. [9], based on the GINA 2006–2010 guidelines, combining diurnal and nocturnal respiratory symptoms, asthma attacks, lung function, hospitalisation for asthma and use of reliever medication.
Significant or borderline significant associations were observed between the weekly use of at least two sprays and childhood- and adult-onset asthma (2.02 (1.20–3.40), 1.60 (0.91–2.81), respectively), with a higher odds ratio for poorly controlled adult-onset asthma (2.29 (1.15–4.54)).The associations between asthma symptom score, asthma status and the use of sprays have been investigated after stratifying on smoking habits, diploma and SPT, and led to similar results. Significant associations were observed between the use of at least two sprays (versus no spray) and a high asthma symptom score (versus no symptom) in never smokers (3.17 (1.60–6.29)) and in smokers (2.54 (1.57–4.10)), in females without (3.69 (1.82–7.48)) and with university diploma (1.87 (0.94–3.71); p=0.07), as well as in females without (2.59 (1.19–5.67)) and with atopy (2.76 (1.32–5.78)). Significant associations were observed between the use of at least two types of spray (versus no spray) and current asthma in never smokers (1.96 (1.08–3.55)) and in smokers (2.79 (1.12–6.99)), in females without university-level diplomas (1.91 (1.06–3.44)) and with a lower odds ratio (1.55 (0.83–2.91)) for those with university-level diplomas. Associations remained similar after adjustment for diploma level (instead of occupational exposure).
DISCUSSION
The domestic use of at least two types of spray per week was significantly and positively associated with a high asthma symptom score and asthma activity (assessed either by current asthma or poorly controlled asthma). Consistent results were observed after stratification on smoking habits, diploma level and atopy. Our results also suggest a selection bias in the use of domestic sprays which may mask or underestimate the associations between sprays and asthma phenotypes. Our results are consistent with those from the single previous epidemiological survey, in which a dose–response relationship was observed between household cleaning sprays and adult-onset asthma [6]. No association was observed among men, probably because only a small number of them (7%) use at least two sprays per week, with an odds ratio of 0.90 for current asthma. The present work suggests that domestic exposure to cleaning sprays, for which increasing use has been observed [23], may represent a public health issue in females.
Domestic use of sprays and asthma in females
Our results are consistent with a deleterious effect in the use of cleaning sprays on asthma phenotypes and with previous results on household exposure [6], from nurse cohorts [5] and cleaners in offices or private homes [1]. The lack of association between home cleaning, evaluated both by self-report and by PCA, and asthma phenotypes, is an argument in favour of the specific effect of products in spray form.
The use of cleaning sprays involved a high risk for inhalation exposure [4]. Peak concentrations of 2-buthoxyethanol (major ingredient of their selected sprayed products) may approach occupational exposure limits and remain in the air after completion of the cleaning task [24]. The deleterious effect of products in spray form such as waterproofing sprays [25], pesticide/insecticide sprays [26, 27] or hair sprays [28] has been established for several diseases.
We observed an association between the use of at least two sprays and IgE-dependent asthma and non-eosinophilic asthma. Further analyses are needed to clarify the underlying mechanisms that may lead to a deleterious effect of sprays on asthma.
Exposure assessment
One limitation of our study relates to the self-reporting of spray exposure, which may lead to misclassification errors, recall bias and biased estimates [2]. One could hypothesise that those with asthma and bronchial hyperactivity may feel uncomfortable using sprays and may therefore remember more details and provide a more precise report or exaggerate the use of sprays (self-report). However, in a recent paper comparing self-reported occupational exposure to cleaning/disinfecting agents and an expert assessment in the EGEA study, we observed that the validity of self-reported exposure to sprays was good (Cohen's κ coefficient 0.84; sensitivity 95%; specificity 91%) [29]. For home cleaning, results were similar whatever the exposure assessments (self-report, “essential tasks”) and asthma phenotypes. No associations were observed between the three most common sprays taken separately and poorly controlled asthma. It was not possible to study specific types of sprays any further due to sample size.
Selection bias or protective effect
Recent European studies [13, 30, 31] support the importance of the healthy worker effect in occupational asthma [12]. This phenomenon might even be more important for domestic exposures because it is easier to alter behaviour in domestic habits as opposed to occupational ones. A “healthy home-cleaning effect” implies that females with asthma might use fewer sprays or cleaning products than those without asthma.
For home cleaning, a significant association was only observed with a high asthma symptom score, and the lack of association for asthma might be explained by a healthy home-cleaning effect (which might be more important for diagnosed asthma than for symptoms). Odds ratios for associations between exposures and disease were always higher for a high asthma symptom score than for current asthma, consistent with a selection bias. It was not possible to study the association between health status and avoidance of polluted places only recorded for participants with asthma, which is a limitation of our study.
For exposure to at least two types of spray, odds ratios were higher in females without avoidance of polluted places than in those with avoidance. The potential selection bias might be higher for sprays than for home cleaning in general. Females may choose which type of products they will use to clean their home. The Asthma Quality-of-life Questionnaire, not originally designed to study avoidance, has been shown to be valid and reproducible [19]. However, to study selection bias in an optimal way all domestic exposure histories need to be taken into account, as performed previously to study the healthy hire effect in the EGEA survey [13]. We hypothesise that a selection bias could explain the lack of association of asthma characteristics with the use of one spray. Such a selection bias could also occur, at a lesser extent, for the use of two sprays and underestimate the association. As it has not been explored before, the hypothesis of a selection bias needs to be considered with caution.
An alternative hypothesis is the protective effect of moderate use of cleaning products on asthma. Individuals with asymptomatic asthma or poorly-controlled asthma might use, in order to keep their home clean, cleaning products and sprays more often than those without asthma. Studies among children with asthma have shown that an improvement of cleaning practices (to have a “clean” home) reduces asthma symptoms [32]. In our study, odds ratios <1 for the use of one spray per week and the first tertile of “domestic wizard” and “chemical products” is consistent with this hypothesis. It remains possible that an unstudied confounding factor may explain the finding. Further studies are needed to clarify this point.
Asthma phenotypes
One strength of the EGEA survey is that participants with asthma were well phenotyped. Asthma status at follow-up has been checked carefully by respiratory epidemiologists and clinicians (F. Kauffmann, V. Siroux and I. Pin) and was defined to favour specificity (if there was any doubt, the participant was classified as being without asthma). The asthma symptom score showed a good ability to detect risk factors [15, 16] and was used in both the ECRHS [33] and the EGEA surveys [13]. Current asthma and asthma control were defined as previously in both the EGEA [9] and ECRHS surveys [17]. For the use of at least two sprays, consistent results were observed with sub-phenotypes such as severe asthma, high symptomatic asthma, asthma with low FEV1, IgE-dependent asthma and non-eosinophilic asthma. However, in the current study, due to the sample size issue, it is difficult to disentangle whether the use of domestic sprays is associated more with a high asthma symptom score, poorly controlled or more severe asthma, as all phenotypes are strongly correlated.
Public health implications
An excess risk of asthma in cleaners has been reported for cleaners in offices, hospitals, private homes and in homemakers doing their own domestic work [1], with a potentially high risk in females typically exposed to household cleaning products [11]. Many people are exposed worldwide, both at work and at home, to cleaning agents in spray form, with an increase of use in the last decade [23]. Personal care and household products represented three-quarters of the aerosol products in Europe, which is the world's largest producer, with 5.1 billion aerosols produced in 2009 out of the 12 billion worldwide [23]. Domestic products might be less toxic than industrial cleaning agents. However, household cleaning substances are classified in the top five substances most frequently involved in all human exposure complaints [3]. Whereas occupational exposure is controlled and monitored, this is not the case for the general consumer [34]. Furthermore, homemakers have no training on the potential toxicity of the products used. In conclusion, more research is needed on hazards related to domestic use of cleaning sprays.
Acknowledgments
EGEA cooperative group: Coordination: F. Kauffmann, F. Demenais (genetics; INSERM U946, Paris, France), I. Pin (clinical aspects). Respiratory epidemiology: M. Korobaeff (EGEA1; INSERM U700, Paris, France), F. Neukirch (EGEA1; INSERM U700, Paris, France), I. Annesi-Maesano (INSERM 707, Paris, France), F. Kauffmann, N. Le Moual, R. Nadif, M.P. Oryszczyn (INSERM CESP/U1018, Villejuif, France), V. Siroux. Genetics: J. Feingold (INSERM U393, Paris, France), E. Bouzigon (INSERM U946, Paris, France), F. Demenais, M.H. Dizier (INSERM U946, Paris, France), I. Gut (CNG, Evry, France), M. Lathrop (CNG, Evry, France). Clinical centres: Grenoble: I. Pin, C. Pison; Lyon: D. Ecochard (EGEA1), F. Gormand, Y. Pacheco; Marseille: D. Charpin (EGEA1), D. Vervloet; Montpellier: J. Bousquet; Paris Cochin: A. Lockhart (EGEA1), R. Matran (now in Lille); Paris Necker: E. Paty, P. Scheinmann; Paris-Trousseau: A. Grimfeld, J. Just. Data and quality management: J. Hochez (EGEA1; INSERM ex-U155, Paris, France), N. Le Moual, C. Ravault (INSERM ex-U780, Paris, France), N. Chateigner (INSERM ex-U794, Paris, France), J. Ferran (Grenoble, France).
The authors would like to thank all those who participated in the setting of the study and in the various aspects of the examinations involved: interviewers, technicians for lung function testing and skin prick tests, blood sampling, IgE determinations, coders, those involved in quality control, data and sample management and all those who supervised the study in all centres. The authors are grateful to the three CIC-Inserm at Necker, Grenoble and Marseille, (France) who supported the study and in which participants were examined. They thank O. Montanguon and P. Carteron for statistical analysis, G. Vasseur for job coding, V. Bassot (all from INSERM, Villejuif, France), A. Bedbrook (INSERM, Montpellier, France) and anonymous reviewers for their helpful suggestions. They are indebted to all the individuals who participated, without whom the study would not have been possible.
Footnotes
This article has supplementary material available from www.erj.ersjournals.com
Support Statement
This study was funded by the French Agency of Health Safety, Environment and Work (AFSSET, EST-09-15); Merck Sharp & Dohme; Hospital Program of Clinical Research (PHRC)-Paris; and the National Research Agency - Health Environment, Health-Work Program (ANR-SEST 2005).
Statement of Interest
A statement of interest for the present study can be found at www.erj.ersjournal.com/site/misc/statements.xhtml
- Received November 13, 2011.
- Accepted March 15, 2012.
- ©ERS 2012
REFERENCES










