





Abstract
The efficacy and safety of two doses of aclidinium bromide were evaluated in patients with moderate to severe chronic obstructive pulmonary disease (COPD).
In this 24-week, double-blind trial, patients were randomised to twice-daily aclidinium (200 μg or 400 μg) or placebo. The primary efficacy end-point was change in trough forced expiratory volume in 1 s (FEV1) at week 24. Other end-points included peak FEV1, health status (St George's Respiratory Questionnaire; SGRQ) and dyspnoea (Transitional Dyspnoea Index; TDI).
Overall, 828 patients were randomised. At week 24, significant improvements from baseline were observed with aclidinium 200 μg and 400 μg versus placebo for trough FEV1 (99 and 128 mL; both p<0.0001) and peak FEV1 (185 and 209 mL; both p<0.0001). Peak FEV1 improvements on day 1 were comparable with week 24. Aclidinium 200 μg and 400 μg produced significant improvements over placebo in baseline-adjusted mean SGRQ total score (-3.8 and -4.6 units; p<0.001 and p<0.0001) and TDI focal score (0.6 and 1.0 units; p<0.05 and p<0.001) at week 24. With both aclidinium doses, the incidence of anticholinergic adverse events was low, and similar to placebo.
Twice-daily aclidinium significantly improved bronchodilation, health status and dyspnoea, and was well tolerated in patients with COPD.
Chronic obstructive pulmonary disease (COPD) is an increasing public health problem that imposes a considerable burden in terms of morbidity, mortality and healthcare costs worldwide [1]. Although not curable, COPD is treatable, with bronchodilator therapy being central to the symptomatic management of the disease [2, 3].
Aclidinium bromide, a novel, inhaled long-acting muscarinic antagonist compound with low systemic activity, has been developed for the treatment of COPD. Initially, aclidinium was investigated as a once-daily drug. In phase III studies, once-daily aclidinium 200 μg significantly improved trough forced expiratory volume in 1 s (FEV1) in patients with COPD versus placebo [4], but this improvement was below the suggested minimum clinically important difference (MCID) of 100–140 mL [5, 6]. Therefore, additional clinical studies were conducted to investigate twice-daily aclidinium. A 2-week crossover study showed that aclidinium 400 μg b.i.d. provided 24-h bronchodilation that was statistically and clinically significant compared with placebo [7]. Subsequently, a 12-week phase III study (AClidinium in Chronic Obstructive Respiratory Disease; ACCORD COPD I) with aclidinium 200 μg and 400 μg b.i.d. reported significant improvements over placebo in bronchodilation, health status and COPD symptoms [8].
This paper presents results from a phase III study of longer duration (Aclidinium To Treat Airway obstruction In COPD patieNts; ATTAIN), which assessed the efficacy and safety of aclidinium 200 μg and 400 μg b.i.d. versus placebo over 24 weeks in patients with moderate to severe COPD.
METHODS
Study subjects
Male and female patients aged ≥40 yrs were included if they were current or former cigarette smokers with a smoking history of ≥10 pack-yrs and had a diagnosis of COPD according to Global Initiative for Chronic Obstructive Lung Disease criteria (post-bronchodilator FEV1/forced vital capacity (FVC) ratio of <70% and FEV1 <80% of the predicted value) [2]. Patients had to demonstrate good technique during lung function assessments according to American Thoracic Society/European Respiratory Society criteria [9].
Key exclusion criteria were: history or current diagnosis of asthma; respiratory tract infection or COPD exacerbation within 6 weeks (3 months if hospitalisation was required) before screening or during the run-in period; clinically relevant respiratory conditions other than COPD; unstable cardiac conditions, including myocardial infarction, within the previous 6 months; and contraindications to the use of anticholinergic drugs.
Inhaled salbutamol was permitted as needed, but was discontinued 6 h before and during study visits. The following concomitant medications were allowed if their administration had been stable for ≥4 weeks before screening: inhaled corticosteroids or oral sustained-release theophyllines; systemic corticosteroids at doses equivalent to 10 mg per day of prednisone or 20 mg every other day; and oxygen therapy (<15 h per day).
This study was conducted in accordance with the Declaration of Helsinki, International Conference on Harmonisation/Good Clinical Practice Guidelines and local regulations. The protocol was approved by an independent ethics committee at each centre before study initiation. All patients gave written informed consent. The study was registered with ClinicalTrials.gov with identifier NCT01001494.
Study design
This was a double-blind, randomised, placebo-controlled, parallel-group phase III study conducted in nine European countries and South Africa. Following screening and a 2-week run-in period to assess disease stability, patients were randomised (1:1:1) to receive aclidinium 200 μg, aclidinium 400 μg or placebo b.i.d. for 24 weeks. All study treatments were administered via a multiple-dose dry powder inhaler (Genuair®; Almirall SA, Barcelona, Spain).
A sample size of 244 patients per treatment arm was estimated to provide at least 90% power to detect a difference of 90 mL in trough FEV1 between the aclidinium arms and placebo at week 24 with a two-sided 5% level of significance, assuming a standard deviation of 240 mL and adjusting for multiple treatment comparisons. The sample size provided sufficient power to detect treatment differences in the secondary end-points.
Measurements
Standardised spirometric measurements (FEV1, FVC and inspiratory capacity) [9] were conducted before the morning dose on day 1 (baseline) and during visits at weeks 1, 4, 8, 12, 18 and 24. Additionally, FEV1 and FVC measurements were obtained at 0.5, 1, 2 and 3 h post-dose and inspiratory capacity measurements at 3 h post-dose on day 1 and weeks 1, 4, 12 and 24. Inspiratory capacity was measured using an inspiratory manoeuvre to total lung capacity from stable tidal breathing [9]. All study centres had identical spirometry equipment, a detailed study manual and training. Spirometry data were electronically transmitted to a data management centre for quality review and only technically adequate measurements were accepted.
Health status was evaluated pre-dose at baseline and weeks 4, 12 and 24 using the St George's Respiratory Questionnaire (SGRQ). Dyspnoea was assessed at baseline using the Baseline Dyspnoea Index (BDI) and changes were measured using the Transitional Dyspnoea Index (TDI) at weeks 4, 12 and 24. The BDI and TDI were administered by an independent reviewer before study procedures.
Patients recorded COPD symptoms and relief medication use daily in an electronic diary; concomitant medications were recorded by the patient in a paper diary. At each visit, COPD exacerbations were identified by the investigator by reviewing records of COPD symptoms, use of daily relief medication and concomitant medications. COPD exacerbations were defined as an increase in COPD symptoms over at least 2 consecutive days, resulting in the increased use of short-acting bronchodilators and/or inhaled corticosteroids (mild exacerbation), treatment with antibiotics and/or systemic corticosteroids (moderate exacerbation), or hospitalisation (severe exacerbation).
Safety was assessed by adverse event monitoring, clinical laboratory data, blood pressure and 12-lead ECG.
Statistical analysis
The primary efficacy end-point was the change from baseline in morning pre-dose (trough) FEV1 at week 24. Secondary end-points were the change from baseline in peak FEV1 (highest FEV1 value observed within 3 h of morning dosing) at week 24 and the percentages of patients achieving clinically significant improvements in SGRQ total score and TDI focal score at week 24. For US regulatory requirements, trough and peak FEV1 values at week 12 were also assessed as primary and secondary end-points, respectively.
Efficacy analyses were performed on the intent-to-treat (ITT) population, defined as all patients who took one or more dose of study medication and had a baseline and one or more post-baseline FEV1 assessment. Missing data were imputed using last observation carried forward (LOCF). For spirometry data, linear interpolation and time-matched LOCF were applied. Changes from baseline in lung function parameters and SGRQ and TDI scores were evaluated using ANCOVA, with treatment group and sex as factors, and age and baseline value as covariates. The percentages of patients with clinically significant improvements in SGRQ (decrease of ≥4 units [10]) and TDI (increase of ≥1 unit [11]) scores were analysed using logistic regression with treatment group, sex, age and baseline value as covariates. Use of relief medication was analysed using normal scores ANCOVA, with treatment group and sex as factors, and age and corresponding normal score baseline as covariates. An annualised rate of COPD exacerbations was calculated using Poisson regression with correction for over-dispersion with treatment group, sex and baseline COPD severity as factors, and age as a covariate. Logistic regression, including treatment group and baseline COPD severity as covariates, was used to analyse the percentage of patients with one or more COPD exacerbation. Safety outcomes were analysed descriptively for the safety population, defined as patients who received one or more dose of study medication.
RESULTS
Patient characteristics
Of the 828 randomised patients, 819 patients were included in the ITT and safety populations. Figure 1 shows patient disposition. Baseline demographics and disease status were similar across treatment groups (table 1).
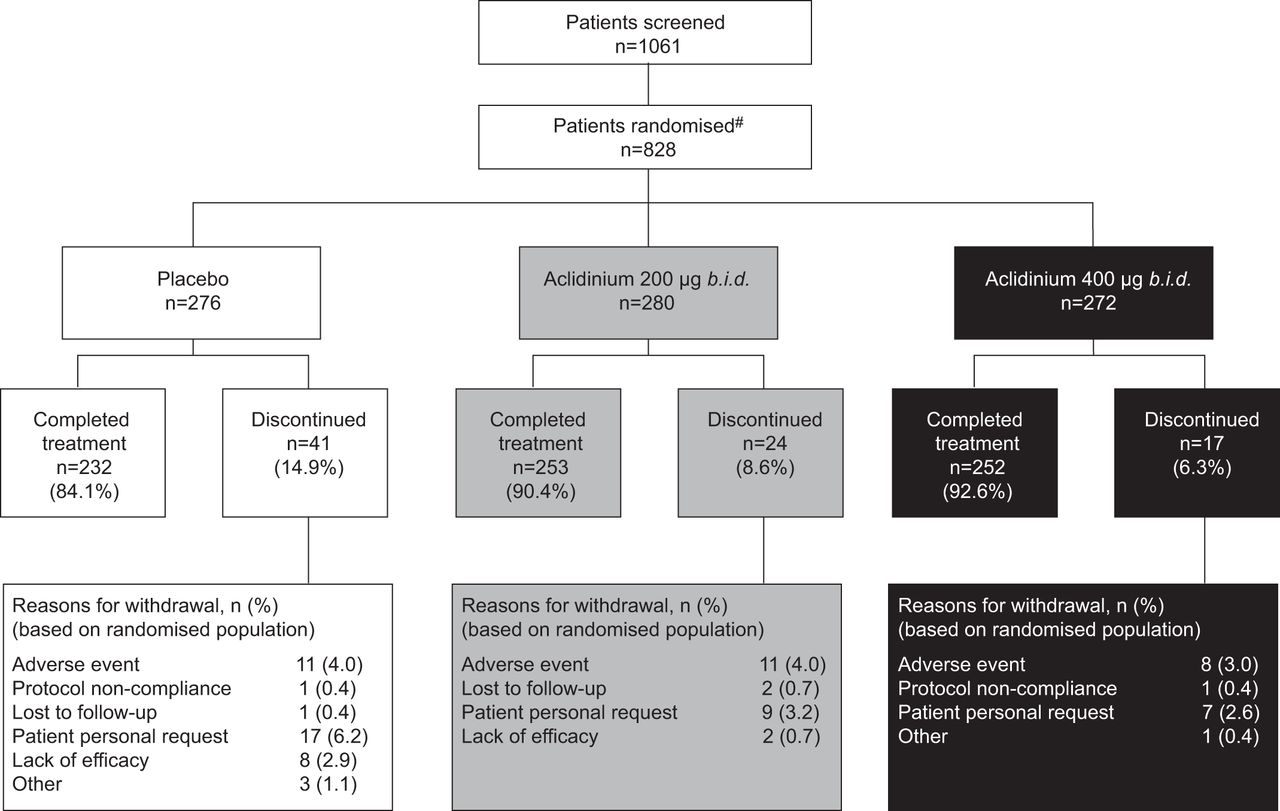
Patient disposition. #: nine patients from one centre were counted as randomised only due to missing baseline data; therefore, the numbers of patients who completed or discontinued treatment do not add up to the total number randomised.
Efficacy
Lung function
At week 24, aclidinium 200 μg and 400 μg produced significant improvements from baseline in mean±se trough FEV1 compared with placebo (by 99±22 mL and 128±22 mL, respectively; p<0.0001 for both) (fig. 2). For both aclidinium doses, the improvement in trough FEV1 was statistically superior to placebo at all measured time points from week 1 to week 24, ranging from 77 mL (week 12) to 105 mL (week 18) for aclidinium 200 μg, and from 105 mL (week 12) to 140 mL (week 18) for aclidinium 400 μg (fig. 2; table 2).

Change from baseline in trough forced expiratory volume in 1 s (FEV1) over 24 weeks. Data are presented as least squares mean±se. #: p<0.0001 for both treatments versus placebo. There were no statistically significant differences between the two aclidinium arms.
Mean±se peak FEV1 significantly improved from baseline with aclidinium 200 μg and 400 μg versus placebo at week 24 (by 185±23 mL and 209±24 mL, respectively; p<0.0001 for both) (fig. 3). At week 12, the corresponding improvements were 182±21 mL and 191±21 mL, respectively (p<0.0001 for both). The improvement in peak FEV1 provided by both aclidinium doses was statistically superior to placebo at all time points from day 1 to week 24 (fig. 3 and table 2). Following the first dose of aclidinium, the increase in peak FEV1 over placebo on day 1 (187 mL, 400 μg) was comparable to that seen at study end (209 mL, 400 μg). The mean post-dose time to peak FEV1 was <2 h for aclidinium 200 μg and 400 μg at all time points except for day 1 (127 and 126 min, respectively).

Change from baseline in peak forced expiratory volume in 1 s (FEV1) over 24 weeks. Data are presented as least squares mean±se. #: p<0.0001 for both treatments versus placebo. There were no statistically significant differences between the two aclidinium arms.
Both aclidinium doses resulted in significant improvements over placebo in FVC and inspiratory capacity values throughout the study (table 2). Numerically greater improvements in trough FVC and trough inspiratory capacity were observed with the 400 μg versus 200 μg dose at all time points; these improvements were statistically significant (p<0.05) at weeks 1, 8, 12 and 18 for trough FVC and at weeks 1, 12 and 18 for trough inspiratory capacity. Aclidinium 400 μg also produced numerically greater improvements versus aclidinium 200 μg in peak FVC at all time points except week 12; these improvements were statistically significant (p<0.05) at weeks 1 and 24.
Health status
Significantly greater improvements from baseline in mean SGRQ total score were observed with both aclidinium doses versus placebo at all time points, except week 4 with aclidinium 200 μg (fig. 4). By week 24, the improvement over placebo in baseline-adjusted mean±se SGRQ total score was -3.8±1.1 units for aclidinium 200 μg (p<0.001) and -4.6±1.1 units for aclidinium 400 μg (p<0.0001). More patients had a clinically significant improvement in SGRQ total score (≥4 units) at week 24 with aclidinium 200 μg and 400 μg compared with placebo (56.0% and 57.3% versus 41.0%; odds ratio 1.83 and 1.87; p<0.001 for both).

Change from baseline in St George’s Respiratory Questionnaire (SGRQ) total score over 24 weeks. Data are presented as least squares mean±se. Values on or below the dotted line represent clinically significant improvement. **: p<0.01; #: p<0.0001 versus placebo.
Dyspnoea and relief medication use
Both aclidinium doses provided significantly greater improvements from baseline in TDI focal score compared with placebo at all time points, except week 12 for aclidinium 200 μg (fig. 5). The improvement over placebo in baseline-adjusted mean±se TDI focal score at week 24 was 0.6±0.3 units for aclidinium 200 μg (p<0.05) and 1.0±0.3 unit for aclidinium 400 μg (p<0.001). More patients treated with aclidinium 200 μg and 400 μg had a clinically significant improvement in TDI focal score (≥1 unit) at week 24 compared with placebo (53.3% and 56.9% versus 45.5%; odds ratio 1.47 and 1.68; p<0.05 and p<0.01, respectively).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change from baseline in Transitional Dyspnoea Index (TDI) focal score over 24 weeks. Data are presented as least squares mean±se. Values on or above the dotted line represent clinically significant improvement. *: p<0.05; **: p<0.01; ***: p<0.001 versus placebo.
Over 24 weeks, the mean total daily use of relief medication was significantly reduced from baseline with aclidinium 200 μg (by 0.61 puffs per day; p=0.0002) and aclidinium 400 μg (by 0.95 puffs per day; p<0.0001) compared with placebo. The percentage of days without the need for relief medication over 24 weeks was significantly increased over placebo by 11% for both doses of aclidinium (p<0.001 for both).
COPD exacerbations
The rate of exacerbations of any severity was lower with aclidinium 200 μg and 400 μg versus placebo (0.43 and 0.40 versus 0.60 per patient per year, respectively). Compared with placebo, the rate ratio with aclidinium 200 μg was 0.72 (95% CI 0.52–0.99; p<0.05) and 0.67 (95% CI 0.48–0.94; p<0.05) with aclidinium 400 μg. The frequency of moderate or severe exacerbations was also lower for aclidinium 200 μg and 400 μg versus placebo (0.35 and 0.34 versus 0.47 per patient per year, respectively), but the rate ratios did not reach statistical significance (0.74, 95% CI 0.53–1.04 and 0.72, 95% CI 0.51–1.02; p=0.08 and p=0.06, respectively).
Safety
The percentage of patients with at least one treatment-emergent adverse event was similar for placebo, aclidinium 200 μg and aclidinium 400 μg (57.1%, 54.5% and 53.5%, respectively). Table 3 shows adverse events reported by ≥2% of patients in any treatment group.
Potential anticholinergic adverse events occurred with an incidence of <1% in any treatment group and were reported at a similar or lower incidence in the aclidinium 200 μg and 400 μg groups compared with placebo, except for urinary tract infection (0.7%, 2.2% and 0.7%, respectively). The percentage of patients reporting dry mouth was low and similar in each group (placebo: 0.4%; aclidinium 200 μg: 0.7%; aclidinium 400 μg: 0.4%).
The percentage of patients experiencing a serious adverse event was similar across the three groups (placebo: 5.5%; aclidinium 200 μg: 4.3%; aclidinium 400 μg: 5.6%). The most common serious adverse event by preferred term was COPD exacerbation, which was reported by 3.7%, 1.4% and 0.7% of patients in the placebo, aclidinium 200 μg and aclidinium 400 μg groups, respectively. Other preferred terms were reported as serious adverse events by no more than one patient in any treatment group. No serious adverse events were considered by the local investigator to be related to study medication. Three patients died during the study; one each in the placebo (road traffic accident), aclidinium 200 μg (myocardial infarction) and aclidinium 400 μg (acute cardiac failure) groups. None of the deaths was thought to be related to treatment.
No clinically relevant changes from baseline in laboratory parameters or blood pressure were observed in any group. The mean changes from baseline in 12-lead ECG parameters were generally small, with no apparent treatment- or dose-related trend: two patients (placebo: n=1; aclidinium 200 μg: n=1) had a QT interval corrected for heart rate using the Fridericia formula (QTcF) of >500 ms, and five patients (placebo: n=2; aclidinium 200 μg: n=3) had a change in QTcF of >60 ms.
DISCUSSION
This study showed that, in patients with moderate to severe COPD, aclidinium 200 μg or 400 μg b.i.d. significantly improved lung function assessments over 24 weeks compared with placebo. The improvement in trough FEV1 with aclidinium 400 μg was 128 mL at week 24. Improvements in trough FEV1 with aclidinium 400 μg ranged from 105 (week 12) to 140 mL (week 18) throughout the study, which is consistently within the proposed MCID of 100–140 mL [5, 6]. However, the improvement in trough FEV1 with aclidinium 200 μg was lower, ranging from 77 mL (week 12) to 105 mL (week 18). Aclidinium 400 μg also showed numerically greater improvements over the 200 μg dose for FVC, inspiratory capacity and peak FEV1 values. This is one of the first bronchodilator trials to report inspiratory capacity. For both aclidinium doses, the improvement in peak FEV1 on day 1 was comparable with week 24.
Improving health status and relieving symptoms are important goals in the management of stable COPD [2]. As the relationship between these outcomes and changes in FEV1 is poor, it is important to measure directly the effect of treatment on health status and symptoms [5]. At 24 weeks, the mean improvement with aclidinium 400 μg versus placebo exceeded the MCID for SGRQ total score and equalled the MCID for TDI focal score. Such large improvements in SGRQ score are reported relatively rarely in clinical trials. With both aclidinium doses, approximately 15% more patients had an improvement that exceeded the SGRQ MCID compared with placebo. For the TDI score, 8% and 11% more patients exceeded the MCID with aclidinium 200 μg and 400 μg, respectively, compared with placebo. These improvements are likely to translate into a noticeable benefit for patients and clinicians in routine clinical practice.
In the placebo arm, FEV1 response declined during the study, whereas SGRQ total score and TDI focal score improved. A similar lack of concordance between FEV1 and SGRQ has been observed in numerous other bronchodilator studies [12].
This study was not powered for exacerbations and the population was not enriched by recruiting patients with a history of frequent exacerbations, as reflected by the modest exacerbation rate in the placebo group. Despite the low rate of exacerbations, both aclidinium doses significantly reduced the rate of exacerbations of any severity compared with placebo. However, these results need to be confirmed in adequately powered trials. There was a similar trend in reduced rates for moderate or severe exacerbations in a second, similar, phase III study [8].
Aclidinium 200 μg and 400 μg b.i.d. for 24 weeks was well tolerated, with no differences between the safety profiles of the two doses. The incidence of anticholinergic adverse events in both aclidinium groups was low and similar to placebo. Moreover, no serious anticholinergic adverse events occurred in any of the study arms. The low incidence of anticholinergic adverse events reported with aclidinium is consistent with earlier studies, which showed that aclidinium is rapidly hydrolysed in human plasma into inactive metabolites [13, 14].
Overall, both aclidinium b.i.d. doses significantly improved bronchodilation, health status, COPD symptoms and exacerbations (any severity). The study was not powered to detect statistically significant differences between doses. However, the 400 μg dose consistently demonstrated numerically greater efficacy compared with the 200 μg dose and produced clinically significant improvements in lung function, health status and symptoms that were not observed with the lower dose. The range of improvement in trough FEV1 observed with aclidinium 400 μg over the study period (105–140 mL) was comparable with results from 6- to 12-month studies of tiotropium, in which improvements ranged from 120 to 150 mL [15–18]. This is consistent with observations from an earlier phase II study, in which aclidinium 400 μg b.i.d. produced 24-h bronchodilation that was similar to tiotropium 18 μg once daily [7]. The improvement in trough FEV1 with aclidinium 400 μg in the present study was also similar to that observed with the same dose in a previous 12-week, phase III study (124 mL at study end) [8]. The 12-week study showed clinically significant improvements in dyspnoea with aclidinium 400 μg; the improvements in health status were statistically but not clinically significant, which may be because the study duration was not long enough for clinical significance to be reached. As both aclidinium doses had a similar safety profile, the risk–benefit profile appears to support aclidinium 400 μg as the appropriate dose for treatment.
In conclusion, given the sustained bronchodilatory effect and low rate of anticholinergic effects, aclidinium b.i.d. may be an effective new long-acting muscarinic antagonist treatment option for patients with stable moderate or severe COPD, with the risk–benefit profile favouring the 400 μg dose.
Acknowledgments
We thank all the ATTAIN study investigators and PAREXEL International Limited. We also thank S. Gladwin from Complete Medical Communications, who provided medical writing support funded by Almirall, SA, Barcelona, Spain.
Footnotes
Support Statement
This study was funded by Almirall, SA, Barcelona, Spain, and Forest Laboratories, Inc., NY, USA.
Clinical Trial
This study was registered with ClinicalTrials.gov with identifier NCT01001494.
Statement of Interest
Statements of interest for all authors, and for the study itself, can be found at www.erj.ersjournals.com/site/misc/statements.xhtml
- Received December 23, 2011.
- Accepted March 5, 2012.
- ©ERS 2012
REFERENCES










