





Abstract
Obstructive sleep apnoea (OSA) is a risk factor for stroke, but little is known about the effect of OSA and continuous positive airway pressure (CPAP) on the incidence of long-term, nonfatal cardiovascular events (CVE) in stroke patients.
A prospective observational study was made in 223 patients consecutively admitted for stroke. A sleep study was performed on 166 of them. 31 had an apnoea/hypopnoea index (AHI) <10 events·h−1; 39 had an AHI between 10 and 19 events·h−1 and 96 had an AHI ≥20 events·h−1. CPAP treatment was offered when AHI was ≥20 events·h−1. Patients were followed up for 7 yrs and incident CVE data were recorded.
The mean±sd age of the subjects was 73.3±11 yrs; mean AHI was 26±16.7 events·h−1. Patients with moderate-to-severe OSA who could not tolerate CPAP (AHI ≥20 events·h−1; n=68) showed an increased adjusted incidence of nonfatal CVE, especially new ischaemic strokes (hazard ratio 2.87, 95% CI 1.11–7.71; p=0.03), compared with patients with moderate-to-severe OSA who tolerated CPAP (n=28), patients with mild disease (AHI 10–19 events·h−1; n=36) and patients without OSA (AHI <10 events·h−1; n=31).
Our results suggest that the presence of moderate-to-severe OSA is associated with an increased long-term incidence of nonfatal CVE in stroke patients and that CPAP reduces the excess of incidence seen in these patients.
In Western countries, ischaemic stroke is the leading cause of long-term disability, and the second of death, after ischaemic heart disease [1]. In patients with previous stroke, the rate of recurrence varies between 8 and 15% over the first year; this rate rises to 30–40% after 5 yrs of follow-up, which is a major source of increased morbidity, mortality, quality-of-life deterioration and healthcare costs [2]. During the past few years, great efforts have been made to determine new preventable and treatable stroke risk factors. Early recognition of these factors seems essential to optimise therapeutic procedures, especially those with a known effective treatment [3].
Obstructive sleep apnoea (OSA) syndrome is a common condition that affects an estimated 4% of adult males and 2% of adult females of the general middle-aged population, and >20% of the elderly population [4,5]. Nasal continuous positive airway pressure (CPAP) is the most recognised and most cost-effective treatment for severe or symptomatic OSA [6]. Large-scale studies have established moderate-to-severe untreated OSA as an independent modifiable risk factor for stroke and other cardiovascular events (CVE) [7–9]. Other studies have concluded that stroke patients with OSA have an increased risk of premature death [10–12]. Meanwhile, some authors have demonstrated that CPAP reduces the risk of fatal and nonfatal CVE in severe OSA [9]. Furthermore, we have previously published a 5-yr follow-up study showing that CPAP treatment reduces the incidence of death in stroke patients with OSA [11]. However, to our knowledge, there is no study available that analyses the long-term impact of untreated severe OSA and CPAP treatment on the incidence of new nonfatal CVE in stroke patients. Since these questions might have important social and economic implications for public health, we undertook a 7-yr prospective observational follow-up study using the series we followed up from 2002 onwards [11,13], with the aim of analysing the long-term impact of OSA and CPAP treatment on the incidence of recurrent nonfatal CVE in patients who survive an ischaemic stroke.
METHODS
Patients
We followed up a cohort of patients consecutively admitted to hospital (Requena General Hospital, Valencia, Spain) with a diagnosis of acute ischaemic stroke (from January 2002 to June 2003) and have carefully recorded the incidence of new cardiovascular events and all-cause death. Those patients who passed the acute phase of the neurological event (alive ≥2 months after the onset of the stroke) were eligible for inclusion and undertook a sleep study. Patients previously treated with CPAP and those in a terminal stage of the disease at the time of the evaluation (Glasgow coma scale score <8) were excluded. Patients diagnosed with heart or respiratory failure, or with a predominance of central respiratory events (>50% recorded time) were also excluded. The study protocol was approved by our local ethics committee and all patients gave informed consent to inclusion in the study.
Assessment of baseline stroke and vascular risk factors
The diagnosis and location of acute ischaemic stroke were determined in accordance with international guidelines [2], based on the evaluation of existing neurological defects and brain computed tomography scans conducted within hours of the patient's admission and several days later. Functional disability and neurological impairment were evaluated using widely validated neurological scales: the Barthel index [14] (at discharge) and the Glasgow coma score (on admission) [15]. The Barthel index assesses daily activity on a scale of 0 to 100 (a score of 100 corresponding to full patient autonomy). Following a stroke, patients received anti-platelet treatment in all cases, and anticoagulant treatment in cases of atrial fibrillation, in the absence of contraindications.
Data were collected from all patients on demographic, clinical, sleep history and past Epworth Sleepiness Scale (ESS) [16]; and anthropometric and other past vascular risk factors, including arterial hypertension (defined according to international guidelines [17] or through the current use of antihypertensive drugs); smoking status (current (>10 cigarettes·day−1) or ever-/never-smoker); atrial fibrillation; diabetes mellitus; peripheral fibrinogen levels in mg·dL−1; hypercholesterolaemia (>250 mg·dL−1 in peripheral blood or current use of treatment); previous cardiovascular disease, including stroke, transient ischaemic attack and ischaemic heart disease with or without myocardial infarction; and carotid stenosis. Significant internal carotid stenosis was considered when >50% of the vascular lumen was affected, as assessed by transcranial Doppler flowmetry and magnetic resonance angiographic confirmation, where appropriate. In the stable phase of a stroke, an ECG and a blood sample test were carried out to reassess current or new vascular risk factors, as well as controlling them and optimising their treatment. A nonfatal event was defined as the occurrence of nonfatal myocardial infarction, stroke, or acute coronary insufficiency that needed coronary artery bypass surgery or percutaneous transluminal coronary angiography, or both. CVE data were recorded from our computer database on hospital admissions, primary-care visits and emergency-room visits.
Sleep studies and CPAP treatment
All the patients included in the study underwent a respiratory polygraphic evaluation in the stable phase of stroke (2 months after the acute episode). CPAP treatment was offered to all patients with an apnoea/hypopnoea index (AHI) ≥20 events·h−1. Nasal ventilation was measured using a nasal cannula. Respiratory events were identified by analysing the nasal flow as well as the thoracoabdominal bands and oxygen saturation records. Apnoea was considered if there was a decrease in the ventilatory signal by 75% or more for <10 s. Hypopnoea was defined as a decrease in ventilatory signal of 25 and 50%, with <3% decrease in arterial oxygen saturation. AHI was defined as the number of respiratory events documented per hour of recording. All respiratory events were classified by manual analysis and all variables were calculated per hour of total study time. After a period of acclimatisation, automatic titration was performed, following the procedure reported by our group [18]. All tests were performed in our hospital in rooms prepared for this purpose by trained personnel. Tests in which the patient claimed to have slept for at least 4 h were considered valid. Tests involving some technical malfunction were repeated. Patients were trained both in the hospital and at home by trained personnel to achieve the best possible adherence to CPAP. Throughout the study, contact was maintained with the patient to solve any possible problems, especially with respect to adverse effects or adjustments to the mask. Both diagnostic and autotitration polygraphic studies were performed, using a validated portable system (AutoSet Portable Plus II; ResMed, Sydney, Australia) as described previously[19].
Follow-up
Figure 1 shows the study design. After the diagnostic sleep study, four groups were established and subjected to follow-up: 1) patients without sleep apnoea (AHI <10 events·h−1); 2) patients with mild sleep apnoea (AHI 10–19 events·h−1); 3) patients with moderate-to-severe sleep apnoea (AHI ≥20 events·h−1) who could tolerate CPAP treatment; and 4) patients with moderate-to-severe sleep apnoea (AHI ≥20 events·h−1) who could not tolerate or were noncompliant with CPAP treatment. CPAP treatment was considered adequate when the system counter registered >4 h (>70% of the days) per night. All patients included in the study were followed up in our outpatient clinic at 1, 3 and 6 months, and every 6 months after that for 7 yrs (last date of follow-up: June 31, 2010) with the same standardised questionnaire used in our centre, to monitor adherence to treatment, and review their general status and the occurrence and date of new vascular events. At the end of the follow-up, any new cardiovascular events, along with the dates and causes, were carefully recorded from our computer database on hospital admissions, visits to the emergency room or primary care visits. In cases of doubtful information, we contacted patients' relatives by phone and an additional medical visit was arranged, if necessary.
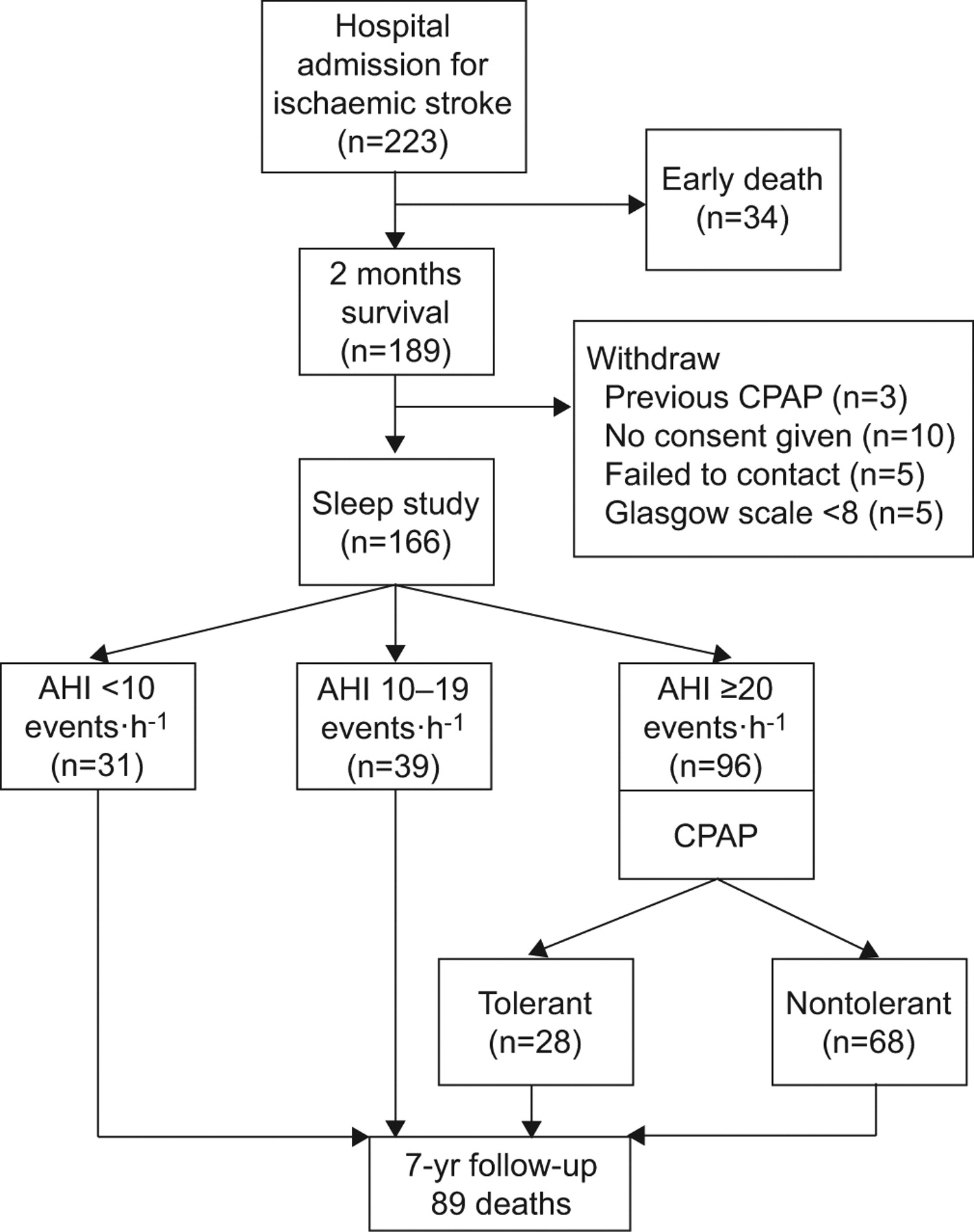
Flowchart of the patients in the study. CPAP: continuous positive airway pressure; AHI: apnoea/hypopnoea index.
Statistical analysis
Baseline data were tabulated as mean±sd for quantitative variables and as absolute values (percentage) for qualitative or dicochomic variables. The comparison of baseline variables between groups was assessed using one-way ANOVA with Bonferroni correction to compare groups in pairs. The primary endpoint in our study was the occurrence of an incident nonfatal CVE. Nonadjusted survival was calculated by the Kaplan–Meier method, with data censored at the time of the end of follow-up. The log-rank test was used to assess differences between groups. Cox proportional hazard regressions (stepwise forward) were used to assess the independent impact of several cut-off levels of AHI and the effect of CPAP treatment on the time to the first nonfatal CVE from the onset of stroke, after adjustment for the following confounding variables (full adjusted model): age, sex, stroke severity (Barthel index), previous stroke or transient ischaemic attack, previous ischaemic heart disease, previous atrial fibrillation, arterial hypertension, diabetes mellitus, hypercholesterolaemia, fibrinogen levels (mg·dL−1), body mass index (BMI) (kg·m−2), current smoking and the presence of significant carotid stenosis (>50%). Hazard ratios and 95% confidence intervals were used to assess the unadjusted and adjusted relationships between the studied variables and the primary outcome. The number needed to be treated in order to prevent a nonfatal CVE with CPAP treatment was also calculated. As an additional analysis, the risk of fatal CVE was estimated in the studied groups, using the same adjustment variables for the analysis of the nonfatal CVE risk. All the reported variables are two-sided and a p-value of 0.05 was considered significant. All the statistical analyses were performed with a commercial statistical package (SPSS 14.0; SPSS Inc., Chicago, IL, USA).
RESULTS
Figure 1 shows that, out of 223 consecutive patients admitted to our centre with a diagnosis of ischaemic stroke, 189 survived for >2 months after the ischaemic cerebrovascular episode. After the exclusion criteria were assessed, a sleep study was performed on 166 patients from this group at 58±12 days after the neurological event. 31(18.7%) patients showed an AHI <10 events·h−1; 39 (23.5%) patients had an AHI between 10 and 19 events·h−1 and 96 (57.8%) patients had an AHI ≥20 events·h−1. The mean age of the whole group was 73.3±11, range 38–97 yrs (59% male). The mean AHI was 26±16.7 events·h−1 with only 2.1±3.3 events·h−1 of central events, and the mean ESS was 9.1±3.4. The main baseline characteristics of the four follow-up groups are shown in table 1. There were no statistically significant differences between groups, except for age. During the follow-up there were 89 deaths (53.6%), distributed as follows in the studied groups: AHI <10 events·h−1 (12 out of 31 deaths; seven of cardiovascular origin (six new fatal strokes and one from myocardial infarction)); AHI 10–19 events·h−1 (17 out of 39 deaths; nine of cardiovascular origin (five new fatal strokes and three of cardiac origin)); AHI ≥20 events·h−1 without CPAP treatment: (46 out of 68 deaths; 31 from cardiovascular diseases (21 new fatal strokes and eight of cardiac origin)) and, finally, IAH≥20 with CPAP treatment (14 out of 28 deaths; seven cardiovascular deaths (five from new strokes and two from myocardial infarction)). Five patients failed to remain in touch after the sleep study but no patients lost contact during the follow-up. None of the patients presented a predominance of central respiratory events. The BMI did not significantly change between the four groups studied during the follow-up.
Incidence of new CVE in OSA patients
44 incident nonfatal CVE were observed during follow-up (26.5%) (table 2). For the purposes of investigation, two groups of OSA severity without CPAP treatment were established (AHI ≥20 events·h−1 versus AHI <20 events·h−1). The risk of nonfatal CVE in patients with an AHI ≥20 events·h−1 without CPAP treatment (n=68; 26 CVEs) was higher than in patients with an AHI <20 (n=70; 13 CVEs) (unadjusted HR 2.45, 95% CI 1.28–4.7; p=0.007), especially for a new ischaemic stroke (19 versus seven). After adjustment for 13 confounding variables (see statistical analysis; fully adjusted model), the risk did not significantly change (adjusted HR 2.15, 95% CI 1.11–4.13; p=0.022). When patients with an AHI <20 events·h−1 were further subdivided into those without OSA (AHI <10 events·h−1; n=31) and those with mild disease (AHI from 0 to 19 events·h−1; n=39), the differences between their adjusted nonfatal CVE risks did not change significantly (six versus seven nonfatal CVE) (table 3). The following patients did not adhere to the anticoagulant treatment: five with atrial fibrillation, two in the AHI <10 events·h−1 group, two in the AHI 11–29 events·h−1 group and one in the AHI >20 events·h−1 with CPAP group. The 7-yr risk of fatal cardiovascular events in the studied groups is shown in table 4.
CPAP tolerance and impact on incidence of nonfatal CVE
CPAP treatment was offered to 96 patients (AHI ≥20 events·h−1). 43 (44.8%) did not adhere to treatment and abandoned it within the first 6 months. During the follow-up 25 more patients left the treatment or were noncompliant with respect to CPAP. The mean duration of the treatment in the noncompliant group was 1.4±1.2 yrs. At the end of the follow-up, only 28 (29.2%) patients were considered as having had good long-term adherence to CPAP treatment (mean 6.1±2.4 h) and the AHI decreased on the night of titration from 26 to 4.1 events·h−1.
Figure 2 shows the curve for survival free of nonfatal CVEs based on the unadjusted Kaplan–Meier model of each of the four studied groups. The incidence of nonfatal CVE in patients with moderate-to-severe OSA who had complaints about CPAP treatment (n=28; five (17.9%) CVEs) was similar to that recorded in patients without OSA or with mild disease. In contrast, moderate-to-severe OSA patients who did not tolerate CPAP treatment (n=68; 26 (38.2%) CVEs) had a significantly greater fully adjusted incidence of nonfatal CVE during the follow-up, as compared with the other studied groups (HR 2.87, 95% CI 1.11–7.71; p=0.03) (table 3). In the group of patients who tolerated CPAP, there was no significant correlation between the number of hours of CPAP use and the risk of new nonfatal CVE. The percentage of CVE of ischaemic stroke origin was significantly higher in the group of moderate-to-severe OSA who did not tolerate CPAP treatment than in the other studied groups (p=0.021) (table 2). The number needed to be treated in order to prevent one new CVE with CPAP treatment was 4.9 patients (95% CI 2–19).

{kind=link}
{kind=link}
Kaplan–Meier cardiovascular event-free survival curve for patients with moderate-to-severe obstructive sleep apnoea (OSA) (apnoea/hypopnoea index (AHI) ≥20 events·h−1) noncompliant with continuous positive airway pressure (CPAP) versus control group without OSA (AHI <10 events·h−1; log-rank test p=0.001) versus mild OSA (AHI 10–19 events·h−1; log-rank test p=0.017) and moderate-to-severe OSA treated with CPAP (log-rank test p=0.013).
DISCUSSION
Two important observations have arisen from our study. First, we provide the first evidence that survivors from ischaemic stroke with nontreated moderate-to-severe OSA showed an increased long-term incidence of a nonfatal CVE, particularly another ischaemic stroke, independent of the severity of the initial neurological event and other cardiovascular risk factors, age and sex. Secondly, we provide the first evidence that long-term CPAP treatment provided protection against the appearance of a new nonfatal CVE, achieving an incidence similar to patients without OSA or mild disease.
In keeping with other transverse and longitudinal studies [6,7], very recent new data from the Sleep Heart Health study [8] confirm an increased adjusted incidence of stroke in a wide community-based sample of males with AHI >19 events·h−1 (HR: 2.86) and female with AHI >25 events·h−1. Furthermore, Sahlin et al. [10] have reported a higher risk of long-term mortality in stroke patients with OSA (AHI >15 events·h−1; HR 1.76), with similar results to those of our group (AHI >20 events·h−1; HR 2.91) [11].
However, few long-term data have been published on the incidence of nonfatal CVE in patients who have suffered a stroke, a group of patients with both a high cardiovascular risk profile and high healthcare costs. Only one study published by our group reported a short-term (18-month follow-up) increase in the incidence of CVE in stroke patients with AHI >20 events·h−1 without CPAP treatment [13]. The present study, using the same series with a higher number of patients and a follow-up very much longer (7 yrs), showed that stable stroke patients with a nontreated AHI ≥20 events·h−1 had a more than two-fold increase in the cumulative incidence of nonfatal CVE, particularly another ischaemic stroke, over a 7-yr period, compared with stroke patients with an AHI <20 events·h−1, independent of other known risk factors for stroke, such as hypertension, atrial fibrillation and a previous cerebrovascular event. Muñoz et al. [20] showed that the probability of a stroke event in elderly people (between 70 and 100 yrs of age) increased only when the AHI was >20 events·h−1. In accordance with these results, we chose this AHI cut-off level as the point where CPAP treatment was first prescribed.
Little is known about the impact of CPAP treatment on stroke patients with OSA. Our group published data showing that CPAP treatment was effective in decreasing the excess of new CVE after 18 months of follow-up [19] and the excess of all-cause mortality after 5 yrs of follow-up [11]. However, this short follow-up period (only 18 months) did not allow us to obtain robust conclusions.
Using the same cohort from the two latest studies [11,19], but with a 7-yr follow-up, the present study shows that CPAP treatment provides protection from the excessive incidence of nonfatal CVE in OSA patients who have suffered from a stroke, especially another ischaemic stroke, when compared with OSA patients with no tolerance for this treatment. On the basis of these results, we calculated that five patients would have to be treated with CPAP in order to avoid a CVE. It is possible that some other mechanisms could be involved in this positive impact of CPAP, over and above the positive impact on blood pressure levels. Some authors have shown that CPAP treatment decreases some other known cardiovascular risk factors in stroke patients, including carotid stenosis, fibrinogen levels and some atheromatosis and inflammatory markers [21], but, in the present study, we did not directly analyse the impact of CPAP on these cardiovascular factors. As additional information from this study, it can also be concluded that the risk of fatal CVE in the group with an AHI >20 events·h−1 without CPAP treatment after a 7-yr follow-up was higher compared with the control group, the group with mild-to-moderate OSA and the OSA group with adequate adherence to CPAP.
The present study does, however, have a series of limitations that require comment. The first limitation derives from the introduction of a selection bias when comparing those patients who tolerate CPAP therapy with those with no tolerance, since intolerant patients could have a distinct profile for adherence to other treatments and, as a consequence, an increase in their cardiovascular risk. Although this could be the case, we used a multivariate statistical analysis in order to take into account all the confounding parameters (full model) that were considered relevant for explaining the differences seen in the incidence of CVE. Moreover, a recent publication concluded that treatment with CPAP made no difference to adherence to cardiovascular treatment in patients with OSA [22], although this phenomenon cannot be ruled out in patients with stroke. We also think that the performance of a 7-yr follow-up study using a randomised placebo design could have ethical implications due to the long follow-up period. Furthermore, non-CPAP users had a higher general cardiovascular risk profile compared with CPAP users in our study. Although the adjusted multivariate analysis in the full model tried to exclude this influence, it cannot be ruled out that the group differences between treated and untreated OSA patients may be explained, at least in part, by differences in comorbidity factors.
The second limitation derives from the low percentage of adherence to CPAP treatment in our patients (nearly 30%). This limitation is a constant in all studies in this field, on account of the great difficulty in treating stroke patients with CPAP (especially those with chronic sequelae) and the lack of somnolence in most cases. In this respect, a specialised team trained both patients and their family members to use CPAP effectively, both during rehabilitation in hospital and at home, in order to achieve the greatest possible adherence to CPAP. Finally, we did not control the changes in cardiovascular risk factors from basal values or the differences between the groups in the quantity of drugs prescribed (or adherence to these drugs), although these factors might influence the results. We did, however, maintain a strict control of the intake of oral anticoagulants in our centre. Five patients either did not follow this treatment or had to be withdrawn because of side-effects, but no significant differences were found between the study groups.
In conclusion, our results suggest that, after a follow-up period of 7 yrs, the incidence of nonfatal CVE is greater than expected in stroke patients with moderate-to-severe OSA not treated with CPAP, independent of any known confounding factors. Even though the CPAP compliance was low, this treatment has proved to be effective in avoiding recurrent nonfatal CVE and might play an important role as a secondary prevention of stroke. After further taking into account the high prevalence of both ischaemic stroke and OSA in the general population, as well as the significant percentage of stroke patients with sleep-disordered breathing [23], it can been seen that the number of neurological events that could be avoided with CPAP treatment would be substantial, with all the positive consequences that this implies in terms of morbidity, mortality, loss of quality of life and healthcare costs. The less-than-optimal compliance with this treatment, however, means that there is a need for more studies to investigate formulas for improving adhesion to CPAP therapy among ischaemic stroke patients. In view of the importance of the subject and the observational nature of this study, further clinical trials are needed to confirm our results.
Footnotes
Support Statement
This study has received a public grant from Sociedad Valenciana de Neumología.
Statement of Interest
None declared.
- Received January 21, 2011.
- Accepted July 22, 2011.
- ©ERS 2012
REFERENCES










