





Abstract
The aim of this study was to investigate whether intratracheal administration of a new synthetic surfactant that includes the cationic, hydrophobic 21-residue peptide KLLLLKLLLLKLLLLKLLLLK (KL4), might be effective in reducing ischaemia–reperfusion injury after lung transplantation.
Single left lung transplantation was performed in Landrace pigs 22 h post-harvest. KL4 surfactant at a dose of 25 mg total phospholipid·kg body weight−1 (2.5 mL·kg body weight−1) was instilled at 37°C to the donor left lung (n = 8) prior to explantation. Saline (2.5 mL·kg body weight−1; 37°C) was instilled into the donor left lung of the untreated group (n = 6). Lung function in recipients was measured during 2 h of reperfusion. Recipient left lung bronchoalveolar lavage (BAL) provided native cytometric, inflammatory marker and surfactant data.
KL4 surfactant treatment recovered oxygen levels in the recipient blood (mean±sd arterial oxygen tension/inspiratory oxygen fraction 424±60 versus 263±101 mmHg in untreated group; p=0.01) and normalised alveolar–arterial oxygen tension difference. Surfactant biophysical function was also recovered in KL4 surfactant-treated lungs. This was associated with decreased C-reactive protein levels in BAL, and recovery of surfactant protein A content, normalised protein/phospholipid ratios, and lower levels of both lipid peroxides and protein carbonyls in large surfactant aggregates.
These findings suggest an important protective role for KL4 surfactant treatment in lung transplantation.
- C-reactive protein
- inflammation
- ischaemia–reperfusion injury
- lipid peroxidation
- lung surfactant
- protein carbonyls
Ischaemia–reperfusion (I/R) injury associated with lung transplantation manifests clinically with vascular permeability, oedema and hypoxaemia 1, 2. Severe I/R injury causes lung damage similar to acute respiratory distress syndrome (ARDS) and represents the prime cause of acute graft dysfunction in the early post-transplantation period 1, 2. Inflammatory mediators released by resident donor macrophages, and recruitment and activation of circulating recipient neutrophils are believed to play a significant role in the cascade of events leading to lung dysfunction 2. Alteration of the alveolar surfactant system is another important factor contributing to lung dysfunction after lung transplantation during the early reperfusion period 3–7.
Exogenous surfactant therapy has been investigated as a therapeutic approach to minimising I/R injury following lung transplantation. In various experimental 8–13 and clinical 14–18 lung transplantation studies, animal-derived surfactants have been administered at different times over the course of the injury, either to the donor (before ischaemia) 8, 10, 12, 13, 16 or to the recipient (before 9–11, 17 or after 12–15, 18 reperfusion). Animal-derived surfactants consist of lipid extract preparations obtained from either bovine or porcine sources 19. Common components in these preparations are phospholipids (PLs), mainly 1,2-dipalmitoylphosphatidylcholine (DPPC), and the hydrophobic surfactant proteins (SP)-B and SP-C. Currently, efforts are underway to develop synthetic surfactants, as surfactants from animal sources raise microbiological, immunological, economic and purity concerns. New synthetic surfactants consist of combinations of synthetic lipids and either synthetic or recombinant peptides 19. A synthetic lung surfactant formulation has been developed based upon a cationic and hydrophobic 21-residue lysine and leucine peptide (KL4; KLLLLKLLLLKLLLLKLLLLK) 20. The KL4 peptide mimics the amino acid sequence of the various peptides taken from SP-B, as it has groups of hydrophobic residues separated by hydrophilic basic residues. The KL4 peptide and SP-B appear to function by inducing lateral stability to the surfactant monolayer 21. The KL4 surfactant is comprised of DPPC, 1-palmitoyl-2-oleoyl-phosphatidylglycerol (POPG), palmitic acid and KL4 peptide. This synthetic surfactant has successfully undergone multicentre clinical trials for the prevention of neonatal respiratory distress syndrome (RDS) 22, 23. Comparisons between KL4 surfactant and a nonprotein-containing synthetic surfactant, colfosceril palmitate (Exosurf®, Glaxo Wellcome, Brentford, UK), indicated that the KL4 surfactant is more effective in preventing the development of RDS, and reducing the incidence of bronchopulmonary dysplasia and RDS-related mortality 22, 23.
The objective of this study was to investigate whether intratracheal instillation of KL4 surfactant to the donor left lung prior to explantation: 1) recovers arterial oxygenation in recipients; 2) improves the composition, alveolar metabolism and biophysical activity of surfactant isolated from transplanted lungs; and 3) reduces the inflammation of the graft.
MATERIALS AND METHODS
For detailed experimental procedures, see the online supplementary material.
Animals and experimental groups
Single left lung transplantation procedures were performed in weight-matched pairs of large (17–23 kg) Landrace × Large White pigs, as described previously 5, 7. A total of 28 pigs was divided randomly into two groups: 1) an untreated group (n = 12; six donors and six recipients) and 2) a KL4-surfactant-treated group (n = 16; eight donors and eight recipients). KL4 surfactant was provided by Discovery Laboratories Inc. (Warrington, PA, USA). Animals (donors and recipients) were sedated with ketamine (20 mg·kg body weight−1), diazepam (0.1 mg·kg−1) and atropine (0.02 mg·kg−1). Anaesthesia was induced with intravenous propofol (2 mg·kg−1), midazolam (0.6 mg·kg−1) and fentanyl (5 μg·kg−1). After endotracheal intubation, anaesthesia was maintained with a continuous intravenous infusion of propofol (9 mg·kg−1·h−1), midazolam (0.6 mg·kg−1·h−1), fentanyl (5 μg·kg−1·h−1) and pancuronium bromide (0.4 mg·kg−1·h−1). Volume control ventilation was used with the ventilatory settings: inspiratory oxygen fraction 1.0; inspiratory:expiratory ratio 1:2; tidal volume 10 mL·kg−1; peak airway pressure 12–20 cmH2O; and positive end-expiratory pressure 5 cmH2O. The initial respiratory rate was 12 breaths·min−1 and was adjusted to obtain end-tidal CO2 30–40 mmHg. All animals received humane care in accordance with the Guide for the Care and Use of Laboratory Animals 24.
Transplantation operation and KL4 surfactant treatment
Briefly, sternotomy, thymectomy and anterior pericardectomy were performed in donors. Before preservation, KL4 surfactant (or the same volume of saline in the untreated group) was instilled into the left lung at 37°C at a dose of 25 mg total PL·kg body weight−1 (2.5 mL·kg body weight−1) KL4 surfactant. Then, a retrograde flush of cold (4°C) University of Wisconsin solution (60 mL·kg body weight−1 under a perfusion pressure ≤30 cmH2O) was performed. The lungs were inflated to a pressure of 20 cmH2O, the trachea stapled and the heart–lung block stored at 4°C for 22 h. Recipients underwent a left posterolateral thoracotomy and the left lung was clamped, excised and lavaged ex situ. The recipient left lung was used as the control lung. Subsequently, the donor left lung was implanted. Upon ventilation of the donor lung, reperfusion was started and the time was set to zero. Ventilatory and haemodynamic parameters were measured as in 7 in the basal situation (pre-surgery) and after lung transplantation at 0, 1 and 2 h following reperfusion.
Lung groups and BAL processing
Individual lung lavages were obtained from the left lung removed from recipients (control group), and donor left lung transplanted into the recipients in KL4 surfactant-treated and untreated animals. Cytometric analyses were performed in cells obtained from BAL from each lung, as detailed in the online supplementary material. The volume of the remaining cell-free BAL was recorded and used for: 1) protein quantification by Lowry’s method, modified by adding sodium dodecylsulfate 5; 2) protein oxidation, determined on the basis of their protein carbonyl contents by the dinitrophenylhydrazine spectrophotometric assay 25; 3) tumour necrosis factor (TNF)-α and C-reactive protein (CRP) quantification using porcine TNF-α (Pierce Endogen, Rockford, IL, USA) and CRP (GenWay Biotech Inc., San Diego, CA, USA) ELISA kits; and 4) surfactant isolation.
Isolation and biochemical analysis of pulmonary surfactant fractions
Cell-free BAL was centrifuged at 48,000×g for 1 h at 4°C to obtain pellets of large surfactant aggregates (LA), which are the active form of surfactant, and supernatant, which contains small surfactant PL vesicles and proteins present in the alveolar fluid (SA). Protein content and protein carbonylation were determined in LA and SA fractions. Surfactant apolipoproteins (SP-A, SP-B and SP-C) were measured by Western Blot analysis from LA as described previously 26. Lipid extracts of LA and SA were obtained by chloroform/methanol extraction 5, and used to quantify total PLs in LA and SA by phosphorus analysis 5 and lipid hydroperoxides by the ferric-xylenol orange method 27.
Surface adsorption assay
The ability of the active fraction of surfactant (LA) to adsorb onto and spread at the air–water interface was tested in a Wilhelmy-like high-sensitive surface microbalance as described previously 5, 7.
Statistical analysis
Data are presented as mean±sd and were normally distributed (Shapiro–Wilk test). For statistical analysis, a two-tailed unpaired t-test was used for comparison of the two groups of recipients (untreated and KL4 surfactant-treated) in the analysis of haemodynamic and gasometric parameters. In studies with different lung groups, differences in means between the three lung types (control, untreated and KL4 surfactant-treated) were evaluated by one-way ANOVA followed by Bonferroni adjustment. An α level ≤5% (p≤0.05) was considered significant.
RESULTS
Physiological responses
Gasometric and haemodynamic parameters were measured in recipients from untreated and KL4 surfactant-treated groups before (basal values) and after lung transplantation. The KL4 surfactant-treated group showed arterial oxygen tension (Pa,O2) values significantly higher than those of the untreated group after 2 h of reperfusion (fig. 1). The preservation of Pa,O2 levels with KL4 surfactant treatment was associated with maintenance of low alveolar–arterial oxygen tension difference (PA–a,O2), indicating protection of the alveolar wall from injury during reperfusion. However, we did not find statistical differences when the haemodynamic parameters of untreated and KL4 surfactant-treated groups were compared (online supplementary table S1).

a) Arterial oxygen tension (Pa,O2) and b) alveolar–arterial oxygen tension difference (PA–a,O2) values in untreated (▪; n = 6) and KL4 surfactant-treated (□; n = 8) recipients over 2 h of reperfusion. Measurements were made in basal situation (pre-surgery), and after lung transplantation at 0, 1, and 2 h of reperfusion. Results are shown for the recipient native right lung after left lung explantation, and the transplanted and native lungs during reperfusion. Data are presented as mean±sd. #: p = 0.01; ¶: p = 0.007.
Changes in lung surfactant
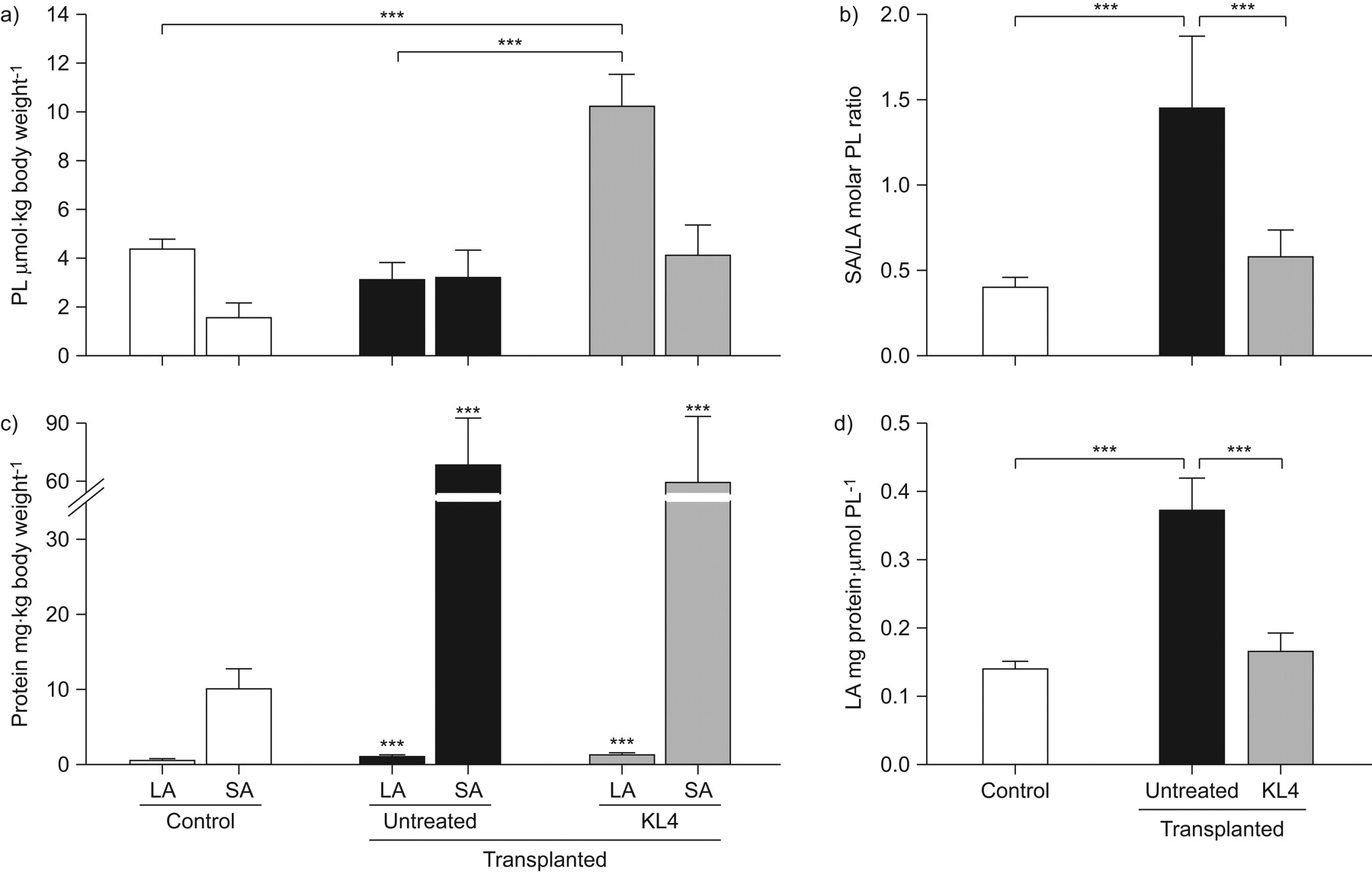
Figure 2 shows the PL and protein content of LA and SA isolated from control and transplanted lungs in both KL4 surfactant-treated and untreated groups. LA represents freshly secreted surfactant membranes from type II cells, whereas SA represents metabolic products of LA formed within the airspace together with proteins present in the alveolar fluid. Figure 2a illustrates that KL4 surfactant-treated lungs showed a significant increase in PL content in LA, but not in SA, with respect to control and untreated transplanted lungs. This indicates that instilled KL4 surfactant reached the alveolus and was efficiently incorporated in LA. The PL SA to LA ratio was significantly higher in lavage material from untreated transplanted lungs as compared to KL4 surfactant-treated and control lungs (fig. 2b). An uneven distribution of surfactant subtypes is a marker of lung injury, and usually occurs by accelerated LA to SA conversion in the inflamed lung due to the presence of proteases and/or oxygen radicals 19. With respect to protein levels in SA and LA fractions, we found that protein levels in SA from transplanted lungs were significantly higher than those of control lungs, regardless of the group considered (KL4 surfactant-treated or untreated) (fig. 2c). Increased levels of proteins recovered in SA indicate leakage of serum proteins into the alveoli. Protein levels in LA of transplanted lungs (either KL4 surfactant-treated or untreated) slightly increased with respect to control lungs (fig. 2c) due to coisolation of some serum proteins with surfactant membranes. Given that serum proteins are potent inhibitors of surfactant biophysical function 19, we used the protein/PL ratio in LA as a marker of surfactant injury. Figure 2d shows that the protein/PL ratio significantly increased in LA of untreated transplanted lungs compared with control and KL4 surfactant-treated transplanted lungs.

a) Phospholipid (PL) content in large (LA) and small surfactant aggregates (SA) from control (n = 10) and transplanted groups, with (n = 8) and without (n = 6) KL4 surfactant treatment. b) Average SA/LA PL ratio in transplanted and control lungs. c) Protein content in LA and SA of control and transplanted lungs. d) Protein/PL ratio in LA from control and transplanted lungs. Data are presented as mean±sd. ***: p<0.001.
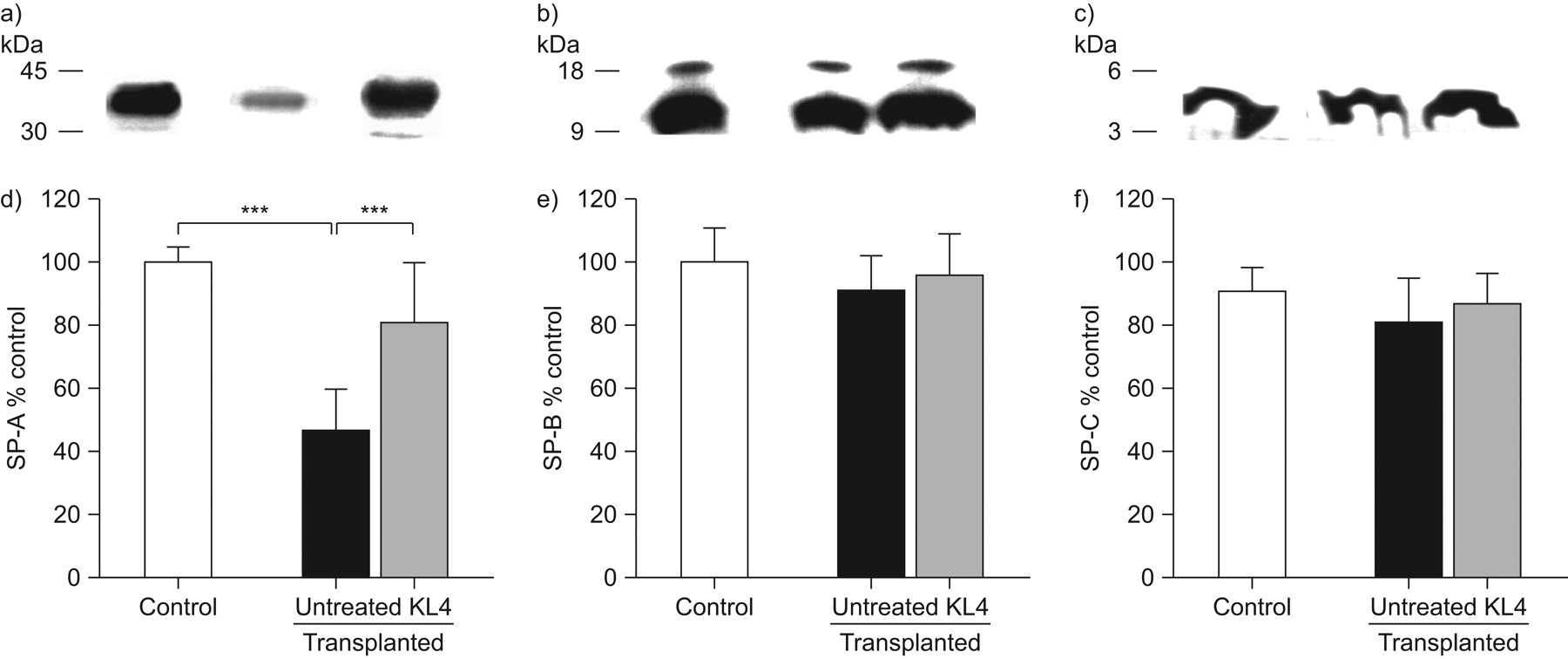
Figure 3 shows that surfactant lipid and protein components were oxidised after lung transplantation, as demonstrated by significant increases in lipid peroxides and protein carbonyls in LA of untreated transplanted lungs. Protein and lipid oxidation was also found in SA of these lungs (data not shown). Remarkably, KL4 surfactant treatment of the donor left lung protected surfactant lipids and associated proteins from oxidative damage (fig. 3). Figure 4 shows the surfactant apolipoprotein content of LA (SP-A, SP-B and SP-C) in control and transplanted lungs. While the amount of both SP-B and SP-C in LA did not change after lung transplantation, the content of SP-A decreased by 54±10% in surfactant from untreated transplanted lungs. KL4 surfactant treatment of the donor left lung returned the content of SP-A to normal (fig. 4).

Oxidation of a) lipids and b) proteins in large surfactant aggregates from control (n = 10) and transplanted lungs (KL4-treated, n = 8; untreated, n = 6). The final concentration of PLs in lipid peroxidation experiments and proteins in carbonylation experiments were similar for all surfactant samples. Data are presented as mean±sd. DNPH: dinitrophenylhydrazine. *: p<0.05.

Levels of immunoreactive a, d) surfactant protein (SP)-A, b, e) SP-B and c, f) SP-C in large surfactant aggregates isolated from control and transplanted lungs with and without KL4 surfactant treatment. 2 μg protein from LA of control (n = 10) and transplanted lungs (KL4, n = 8; untreated, n = 6) were separated by a) 12%, b) 16% and c) 18% sodium dodecylsulfate–polyacrylamide gel electrophoresis, transferred to nitrocellulose and blotted with polyclonal antibodies against a) SP-A, b) SP-B or c) SP-C. d–f) Quantitation of surfactant apolipoproteins was achieved by densitometric evaluation of the immunoreactive bands. Data are presented as mean±sd. ***: p<0.001.
Surfactant function was determined by measuring the ability of LA to adsorb onto and spread at an air–water interface using a Wilhelmy dipping plate attached to an electrobalance suitable for monitoring changes in surface pressure 19. The amount of surfactant PLs injected into the hypophase was the same for all samples from the control and transplanted groups. Interfacial adsorption is performed through 1) the transport of the material injected through the bulk liquid to accumulate at the air–liquid interface and 2) the spread of the material along the surface, producing the surface pressure we measured. The results indicate that the surface adsorption rate of surfactant from untreated transplanted lungs decreased significantly compared with surfactant isolated from control lungs (fig. 5). KL4 surfactant treatment resulted in complete normalisation of surfactant interfacial adsorption activity.

Interfacial adsorption kinetics of large surfactant aggregates from control (○) and transplanted lungs with (•) and without (▪) KL4 surfactant treatment. The final concentration of phospholipids in the hypophase was 83 nmol·mL−1 for all surfactant preparations obtained from control (n=10) and transplanted lungs (KL4, n = 8; untreated, n = 6). Data are presented as mean±sd. π: surface pressure. ***: p<0.001.
To investigate the contribution of ischaemia to the alterations observed in surfactant composition and function after I/R injury, we performed biophysical and biochemical studies in LA and SA isolated from preserved lungs (i.e. the right lung of the donor). We found no differences in PL and protein content in LA and SA, SP-A content or surfactant surface adsorption between samples isolated from control and preserved lungs (online supplementary fig. S1). Furthermore, normal surfactant function and composition were found in the right lung of recipients (native lung) (data not shown), indicating that surfactant alterations are restricted to the transplanted lung as a result of I/R injury.
Other injury variables in BAL
Increased levels of proteins were recovered in cell-free BAL of transplanted lungs regardless of the treatment group (KL4 surfactant-treated or untreated), as a consequence of the oedema (online supplementary fig. S2). We determined the concentration of protein carbonyls in cell-free BAL as an indicator of oxidative stress. Figure 6a shows that protein oxidation greatly increased after transplantation and KL4 surfactant treatment of the donor left lung protected against oxidative damage.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Inflammatory markers in bronchoalveolar lavage isolated from control (n = 10) and transplanted lungs (KL4, n = 8; untreated, n = 6). a) Protein carbonyls per milligram of protein, b) levels of immunoreactive C-reactive protein (CRP) and c) tumour necrosis factor (TNF)-α, and d) percentage of neutrophils. Data are presented as mean±sd. DNPH: dinitrophenylhydrazine. *: p<0.05.
CRP is one of the most characteristic acute-phase proteins displaying rapid and pronounced increase in BAL in response to inflammation 5, 28, 29. Figure 6b shows that the concentration of CRP significantly increased in cell-free BAL of untreated transplanted lungs. KL4 surfactant treatment decreased CRP content in BAL.
TNF-α is an early-response cytokine, produced primarily by alveolar macrophages, which promotes the cascade of events that leads to pulmonary inflammation 2. Figure 6c shows that TNF-α levels greatly increased in transplanted lungs regardless of the treatment group considered (KL4 surfactant-treated or untreated). Likewise, neutrophil entry was observed in transplanted lungs. KL4 surfactant treatment did not influence neutrophil influx into the grafts, which is consistent with previous studies using animal-derived surfactant 12.
DISCUSSION
Severe I/R injury leading to primary graft dysfunction occurs in 15–25% of lung transplant recipients, and contributes to significant morbidity and mortality 1. We found that transplantation and reperfusion of porcine lungs that had been stored for 22 h at 4°C resulted in severe I/R injury characterised by: 1) significant decrease in Pa,O2 and increase in PA–a,O2; 2) increase in plasma protein leakage and neutrophil influx into the alveolar space of transplanted lungs; 3) increase in injury markers, such as TNF-α, CRP, lipid peroxidation and protein carbonyls in alveolar fluid of transplanted lungs; and 4) inactivation of surfactant biophysical activity. Surfactant disturbances largely contributed to impairment of gas exchange under these conditions, as KL4 surfactant treatment of the donor left lung, prior to explantation, recovered Pa,O2 and maintained normal PA–a,O2.
Surfactant inhibition or inactivation refers to processes that decrease or abolish normal PL adsorption to form a functional surfactant monolayer at the air–liquid interface film and/or prevent the film from reaching low surface tension upon compression 19. The significant decrease of surface adsorption rate of surfactant isolated from untreated transplanted lungs can be explained by the following. 1) Significant increase in lipid peroxides and protein carbonyls in the active surfactant fraction or LA: reactive oxygen species released by activated alveolar macrophages and neutrophils may be involved in surfactant oxidation, which results in structural alterations that lead to poor surface activity 30. 2) High SA/LA PL ratio, which suggests accelerated LA to SA conversion, probably as a consequence of structural alterations in oxidised LA. 3) Reduction of SP-A content in LA, which directly affects both surfactant surface adsorption and rate of LA to SA conversion 19. 4) Significant increase of CRP and other serum proteins in alveolar fluid, which are potent inhibitors of the biophysical activity of surfactant 5, 28, 29. The reduction of SP-A levels enhances susceptibility of surfactant to inactivation by CRP, as SP-A binds to CRP and blocks CRP inhibitory effects on surfactant membranes 29. In summary, we conclude that oxidation of lipids and proteins in surfactant, decreased levels of SP-A, and the presence of CRP and other surfactant protein inhibitors may render the lung susceptible to atelectasis caused by a loss of surfactant function.
Instillation of KL4 surfactant in donor left lungs prior to explantation significantly improved Pa,O2 of recipients, probably as a consequence of surfactant protection from oxidative damage, and recovery of surfactant composition and biophysical activity. KL4 surfactant treatment contributed new and fresh tensoactive material that increased the amount of PLs in LA, and normalised the SA/LA PL ratio and the interfacial adsorption rate of surfactant. In addition, KL4 surfactant treatment prevented production of both lipid peroxides and protein carbonyls in the alveolar compartment, decreased CRP levels and normalised SP-A. In contrast, KL4 surfactant treatment did not prevent or reduce plasma protein leakage and neutrophil influx into the alveolar space of the graft, as previously reported in other studies showing potential benefits of exogenous surfactant treatment in I/R injury after lung transplantation 11, 12. Interestingly, these lung injury sequelae (i.e. high alveolar protein concentration and percentage of neutrophils in BAL) were absent 1 week after transplantation in animals treated with surfactant before reperfusion, but were not observed in untreated rats 9.
The fact that KL4 surfactant prevented oxidation of lipids and proteins present in the alveolar compartment suggests that KL4 surfactant might downregulate alveolar cell respiratory burst. This is supported by the fact that neutrophil respiratory burst oxidase activity is inhibited in vitro by KL4 surfactant 31 and DPPC, the major lipid component of both KL4 surfactant and animal-derived surfactants, plays an important role in downregulating monocyte respiratory burst 32. Oxidative stress and innate immunity have been recently identified as key lung injury pathways that control the severity of acute lung injury 33. Intratracheal administration of synthetically oxidised surfactant PLs can trigger acute lung injury in vivo, acting through Toll-like receptor 4, and oxidised PL production is a general feature of lethal lung injury in humans and other species 33. These data support the relevance of KL4 surfactant as a therapy in lung transplantation, given its protective effect from oxidative damage.
The decrease of CRP in BAL of KL4 surfactant-treated grafts suggests local CRP generation in lung tissue after transplantation, since protein leakage into the alveolar space was not prevented by KL4 surfactant treatment and plasma CRP levels were not elevated after reperfusion (data not shown). Thus, increased CRP levels in BAL of untreated transplanted lungs might be produced locally by alveolar macrophages 34 and/or epithelial cells 35, 36, as production of CRP by these cells is upregulated by proinflammatory stimuli 34–36. The fact that KL4 surfactant reduced CRP levels, and lipid and protein oxidation in the alveolar compartment suggests that KL4 surfactant might modulate the activation of alveolar cells and inflammation, as has been previously demonstrated in human airway epithelial cells exposed to hyperoxia 37.
The observation that KL4 surfactant treatment normalised SP-A levels was unexpected, as it does not contain SP-A. One possible explanation is that leukocyte proteases are more damaging to oxidised proteins, and KL4 surfactant prevented protein oxidation in LA. Alternatively, this preservative effect of KL4 surfactant may be attributed to the strong binding of SP-A to KL4 surfactant membranes 38, which might protect SP-A from degradation.
The therapeutic dose we used for intratracheal administration of KL4 surfactant (25 mg·kg body weight−1) to donor lungs is ∼15% of the dose recommended for surfactant instillation in neonatal RDS (175 mg/kg bw), and much lower than that used for the treatment of patients with ARDS (100–300 mg·kg body weight−1) 19 and that previously used in experimental lung transplantation (50–200 mg·kg body weight−1) 8–13. We found that a higher dose of KL4 surfactant (65 mg·kg body weight−1 (2.5 mL·kg body weight−1) did not increase the beneficial effect of this synthetic surfactant (data not shown). It is important to point out that recent studies reporting the beneficial effect of surfactant in clinical lung transplantation were performed with low doses of commercially available animal-derived surfactant (∼20–45 mg·kg body weight−1) 14, 17, 18, and our data indicated that instilled KL4 surfactant at low doses in the donor left lung was effective in I/R injury after lung transplantation.
In summary, we conclude that KL4 surfactant treatment in the donor at low doses protects against oxidative damage, recovers the composition and biophysical activity of surfactant, and causes a parallel improvement of arterial oxygenation, minimising the damage triggered by I/R after lung transplantation.
Acknowledgments
We acknowledge C. Cochrane (Scripps Research Institute, La Jolla CA, USA) for his useful suggestions on a critical reading of the manuscript and Discovery Laboratories Inc. (Warrington, PA, USA) for providing KL4 surfactant.
Footnotes
This article has supplementary material available from www.erj.ersjournals.com
Support Statement
This research was supported by Ministerio de Educación y Ciencia (SAF2006-04434 and SAF2009-07810), Instituto de Salud Carlos III (CIBERES) and Fundación Médica MM.
Statement of Interest
A statement of interest for R. Segal can be found at www.erj.ersjournals.com/site/misc/statements.xhtml
- Received February 7, 2010.
- Accepted July 2, 2010.
- ©ERS 2011
REFERENCES










