





Abstract
Electrical impedance tomography (EIT) has been used to study regional ventilation distribution in neonatal and paediatric lung disease; however, little information has been obtained in healthy newborns and infants.
Data on regional ventilation distribution and regional filling characteristics were obtained using EIT in the neonatal period, at 3 and 6 months of age, in spontaneously breathing infants during non-rapid eye movement sleep. Regional ventilation distribution was described using regional end-expiratory and end-inspiratory impedance amplitudes, and geometric centre of ventilation. Regional filling characteristics were described with the phase lag or lead of the regional impedance change in comparison to global impedance change.
32 infants were measured in the supine position. Regional impedance amplitudes increased with age but regional ventilation distribution remained unchanged in all infants at any age, with the dependent (posterior) lung always better ventilated. Regional filling characteristics showed that the dependent lung filled during inspiration before the nondependent lung during all follow-up measurements.
Regional ventilation distribution and regional filling characteristics remained unchanged over the first 6 months of life, and the results obtained on regional ventilation distribution are very similar to those in adult subjects.
- Electrical impedance tomography
- healthy reference
- infant
- respiratory mechanics
- sigh
- ventilation distribution
A better understanding of normality is needed for deriving thresholds of clinical significance for disease 1. The rapid lung growth occurring over the first few years of life necessitates repeated measurements to understand the developmental changes of lung growth and physiological behaviour 2. The performance of such measurements has been technically difficult, due to the inability of infants and young children to cooperate with testing and the lack of repeatable noninvasive tests 3. Although there is a sound body of literature describing the respiratory mechanics of neonates and infants in disease 3–5, much knowledge is yet to be obtained in spontaneously breathing healthy infants. In this age group, the traditional methods of measuring respiratory mechanics, in particular regional ventilation distribution, pose some difficulties 6–8. Multiple-breath inert gas washout techniques are commonly used to assess ventilation distribution, but cannot provide information about regional ventilation distribution 5, 8. Other methods, such as computed tomography (CT) and aerosol dispersion, involve exposure to radiation 9, 10.
Electrical impedance tomography (EIT) has emerged as a noninvasive functional imaging modality that can be used to measure regional ventilation distribution 11. EIT can be used repeatedly for extended periods of patient monitoring, without the need for sedation. One of the distinct advantages of EIT measurements is that data can be analysed over a given time period and reported as an EIT image, similarly to a CT scan, or analysed on a breath-by-breath basis, to analyse the time course of regional filling 12, 13. This aspect is important for lung function measurements in infants, where irregular breathing and sighs are a common finding 1. This paper reports the results of follow-up EIT measurements from a small cohort of healthy newborns at 2 weeks, and at 3 and 6 months of life measured in non-rapid eye movement (NREM) sleep. The questions that have been addressed are: 1) does regional ventilation distribution change within the first 6 months of life; 2) does regional filling change; and 3) what is the impact of a sigh on regional ventilation distribution?
MATERIAL AND METHODS
Study design
This study was undertaken as part of a larger prospective healthy reference cohort study from birth to 2 yrs of age, in which healthy term neonates were enrolled following a normal delivery. Regional ventilation distribution with EIT was evaluated during regular quiet breathing in NREM sleep at 2 weeks, and 3 and 6 months of age.
Subjects
EIT measurements were taken in the supine position at 2 weeks, and 3 and 6 months of age in 32 term infants (17 males and 15 females) in the sleep laboratory of the Mater Children’s Hospital, Brisbane, Australia. Inclusion criteria were nonsmoking families without a history of allergies or pulmonary disease and without pre- or perinatal maternal medical history. The study had the approval of the local research ethics committee and written informed consent was obtained. A polysomnography and sleep staging was performed according to recommendations 14.
EIT
A Goe-MF II system (Cardinal Health, Hoechberg, Germany) was used to perform EIT measurements in the supine position for durations of 10 min. The principles of EIT systems have been published elsewhere 11, 12, 15, 16. All EIT measurements were taken with electrodes at nipple level and were sampled at 13 images·s−1 (13 Hz) with a 50 kHz injection current of 5 mA peak-to-peak. EIT data were referenced to a regular tidal breathing period during quiet NREM sleep. Data were analysed offline using a custom-developed EIT Data Analyser program based in MATLAB v7.7 (The Mathworks Inc., Natick, MA, USA).
Image analysis
EIT data were band-pass filtered, inclusive of the first and second harmonics of the respiratory rate 12, 17, 18, and a cut-off mask at 20% of the peak impedance signal applied 19. EIT images were generated using the average end-expiratory to end-inspiratory impedance differences for each individual pixel time-course array to describe the magnitude of the regional tidal volume change among individuals. Six slices from anterior to posterior (A–P axis) and from right to left (R–L axis) were defined as regions of interest (ROI)1–6 for regional impedance amplitude analysis 15. EIT images and regional amplitudes were obtained for ≥10 consecutive breaths during quiet breathing. Additionally, the regional impedance amplitudes were measured prior to, during and after a sigh in NREM sleep. The geometric centre of the EIT image was calculated for the entire image, and for the right and left lung separately 20. The geometric centre, based on the 32×32 matrix, defines the centre of ventilation using a balanced averaging of pixel values from anterior to posterior or from right to left.
Time-course analysis
Regional filling characteristics of the lung can be measured using the time-course of the impedance measurements. An ROI impedance change may show a phase lead or lag in relation to the whole lung. Such phase shifts were described with phase angles 21. If an ROI fills ahead of the rest of the lung, the phase angle is positive. If an ROI fills after the rest of the lung, the phase angle becomes negative. We used a cross-correlation method to calculate the phase angles 12, 22.
Analysis of sighs
The regional impedance amplitudes were calculated for 10 breaths prior to and after a sigh, and also during the sigh itself. The regional volume expansions of the tidal breaths and the sigh were compared to global volume expansion by plotting the impedance change of the anterior or posterior lung against that of the global signal, forming a curve 13. A linear relationship is found if the percentile degree of volume change of an ROI is the same as that of the global lung. If the rate of change in an ROI is initially less but then, towards the end of the inspiratory effort, greater than the global lung, then the curve has a concave shape. If the rate of expansion in a ROI during the initial phase of the inspiration is greater than the global lung but decreases towards the end, then the curve has a convex shape. In order to quantify this physiological behaviour, a curve fit was performed 23 using the formula: 
where I(g) is the impedance change of the ROI, g is the impedance change of the global signal, FI is the filling index of the ROI, and a and c are constants. FI describes the shape of the curve, where a convex curvature is evident when FI < 1 and a concave shape is evident when FI > 1; thus, physiological behaviour observed. To analyse the impact of a sigh on regional filling characteristics, the FIs of the anterior and posterior lung were calculated for 10 breaths prior to, during and 10 breaths after a sigh.
Statistics
Data are presented as mean (95% CI). A one-way ANOVA with a Bonferroni correction was applied for repeated measurements.
A multi-way ANOVA was performed to assess the effect of sex, age and region of interest on regional amplitudes, geometric centre and phase angles. A paired t-test was used for comparison of variables within different lung regions. For statistical analysis, SPSS version 15.0 (SPSS Inc., Chicago, IL, USA) was used.
RESULTS
Feasibility of measurements
All 32 enrolled infants were assessed with EIT during NREM sleep at mean±sd 13.7±3 days; 25 infants were followed up at 3 months (age 97±8 days) and 26 infants at 6 months (age 187±6 days). In each infant, at least one 10-min EIT measurement was obtained at each recording session.
Image analysis
Overall, there were significant increases in regional amplitudes with age for all ROIs investigated in the A–P and R–L axes (p<0.001 by multi-way ANOVA) (fig. 1). Inspection of regional differences showed that the measured ROI amplitudes in the gravity (A–P) axis increased, with the greatest change between 2 weeks and 3 months of age for all measured ROIs (p<0.05 by one-way ANOVA with Bonferroni correction), but then only a moderate increase was found between the ages of 3 and 6 months (not significant). The greatest regional amplitude change with growth was found in the posterior (dependent) lung, with an mean amplitude of 0.045 (95% CI 0.006) at 2 weeks, 0.055 (95% CI 0.006) at 3 months and 0.066 (95% CI 0.008) at 6 months of age (p<0.001). In the anterior (nondependent) lung, the mean amplitude increased similarly but to a lesser extent, from 0.039 (95% CI 0.004) at 2 weeks to 0.054 (95% CI 0.004) at 3 months and to 0.060 (95% CI 0.007) at 6 months of age. In the R–L axis, the regional amplitudes increased with age similarly to the A–P axis, with the greatest change between 2 weeks and 3 months, but a lesser change between 3 and 6 months of age. The geometric centre remained, over the entire age range, in the centre of the chest with a slight trend in location toward the anterior lung (fig. 2).
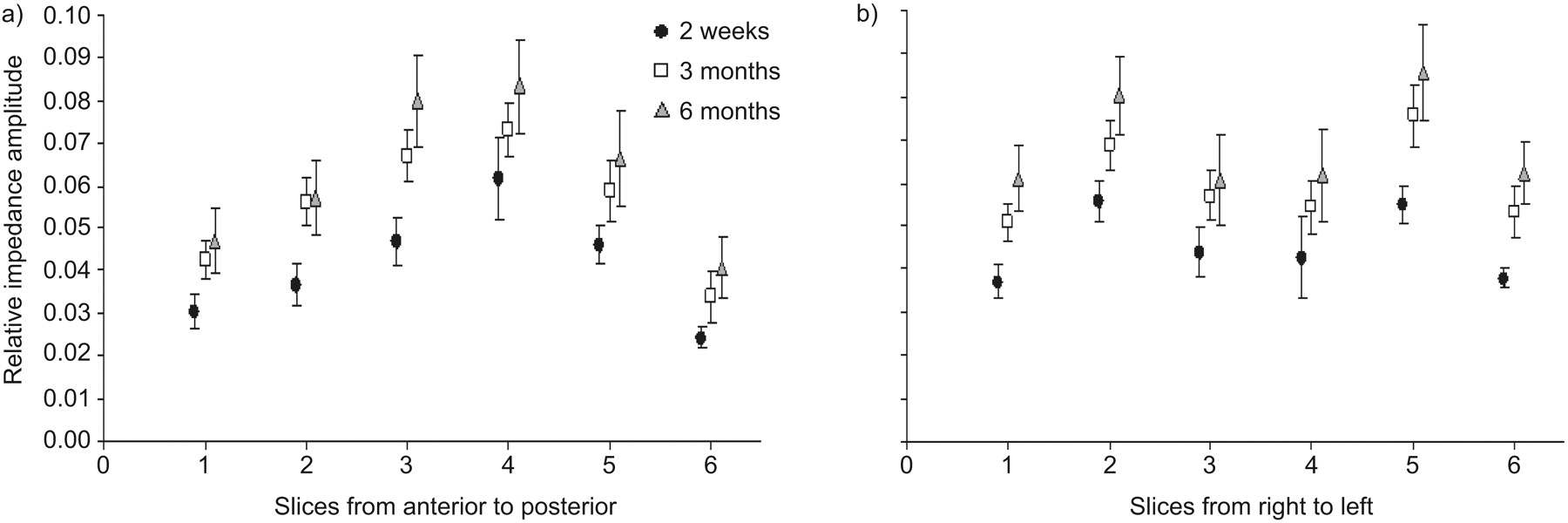
Regional impedance amplitudes increased overall between 2 weeks and 6 months of age (p<0.001), with the greatest increase in regional amplitudes between 2 weeks and 3 months of age. a) Anterior-to-posterior axis. b) Right-to-left axis. Data are presented as mean (95% CI).
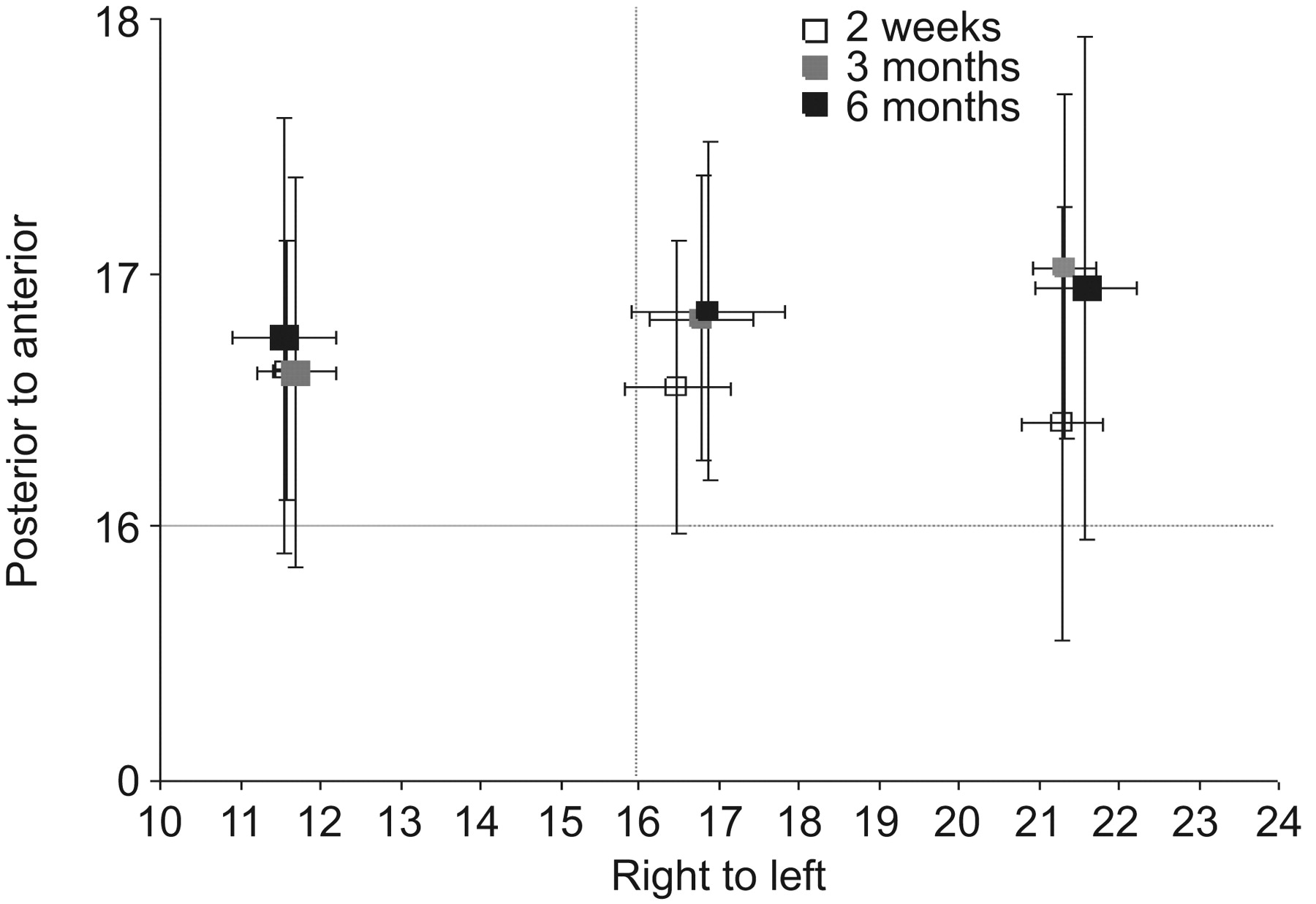
Global, and left- and right-lung geometric centres. The geometric centre remained centrally located at 2 weeks, and 3 and 6 months of age. Data are presented as mean (95% CI).
Time-course analysis
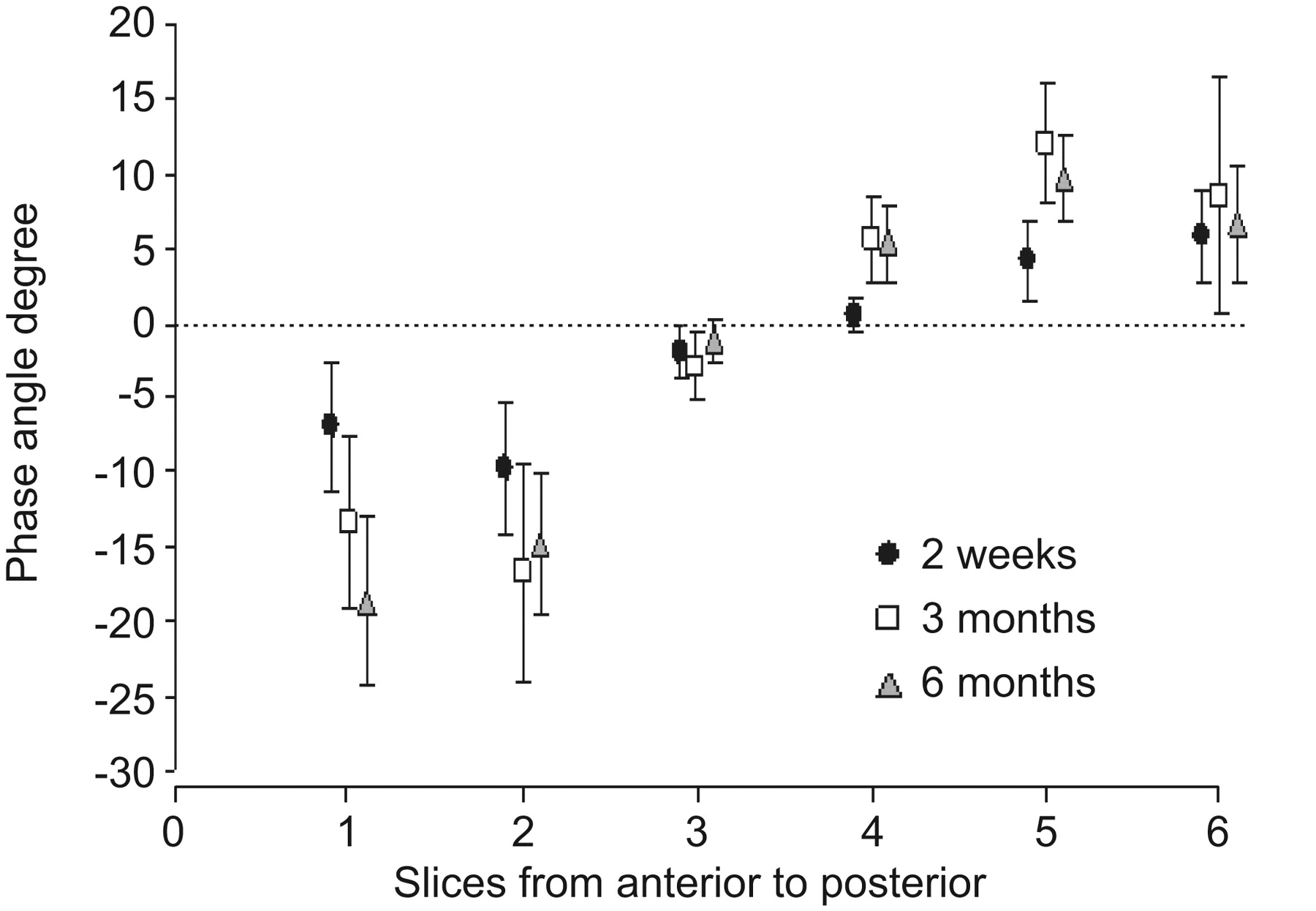
The phase angles for the anterior (nondependent) lung were predominately negative and those for the posterior (dependent) lung were positive, indicating that, during spontaneous breathing, the dependent lung filled before the nondependent lung (p<0.05) (fig. 3). A similar filling pattern was found at 3 and 6 months of age (p<0.05). The comparison of the filling pattern between right and left showed that the right lung filled before the left lung in all age groups (p<0.05).

Regional filling characteristics described by phase angles. A positive value indicates that a region of interest (ROI) fills ahead of the rest of the lung, while a negative value indicates that an ROI fills after the rest of the lung. Data are presented as mean (95% CI).
Analysis of sighs
For each infant, at least two sighs were considered for analysis at each age. The measured regional impedance amplitudes of tidal breaths before and after a sigh were not different (not significant) for all age groups (fig. 4). The regional impedance amplitude of the sigh was significantly greater than that of the tidal breaths, but showed a similar regional distribution to the posterior lung showing the greatest impedance amplitudes. The FIs of the posterior and anterior lung showed a very characteristic behaviour in all investigated infants prior to and after a sigh. The FIs of the posterior lung were significantly less than 1.0, indicating that the rate of volume change in the dependent lung is greater at the beginning of the inspiration compared with the rest of the lung. The FIs of the anterior lung before and after the sigh were greater than 1.0, showing a reduced initial rate of volume change in the nondependent lung. The FI of the sigh itself showed the opposite value to the tidal breaths before and after the sigh. This pattern was similar for all age groups (table 1).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Filling indices averaged for all newborns (2 weeks of age) calculated for the anterior and posterior lung for the 10 breaths prior to the sigh, the sigh iself and 10 breaths after the sigh. Data are presented as mean (95% CI). *: p<0.05 for the sigh itself compared with before and after.
DISCUSSION
EIT has emerged as a new noninvasive lung function monitoring tool, but its role in assessing the progression of lung disease remains unclear and is a topic of many recent studies 11. Most published studies present data obtained in mechanically ventilated subjects or patients with lung disease. Few reports document EIT measurements in healthy subjects and none yet exist for follow up studies. We investigated healthy newborn infants and followed them up with EIT measurements to provide normal data.
EIT
Image analysis
The investigation of the change in regional ventilation over the first 6 months of age along the gravity (A–P) axis showed that the posterior (dependent) lung was slightly better ventilated than the anterior (non-dependent) lung, irrespective of age. Figure 1 shows that the greatest increase in ventilation between 2 weeks and 3 months of age occurred in the posterior lung. In the R–L axis, a similar increase in regional ventilation could be observed, with both lungs contributing a similar amount. Two aspects of these findings need to be discussed. First, age-specific normal values for the magnitude of regional ventilation were found, with the dependent lung preferentially better ventilated in all age groups. Brown et al. 24 described similar maturational changes in absolute lung resistivity with serial EIT measurements and showed that resistivity increases with age. Secondly, there is a proportionally larger increase in the magnitude of regional ventilation in the posterior (dependent) than in the anterior (nondependent) lung with growth. These findings contradict conventional wisdom on neonatal ventilation distribution, which states that the nondependent lung is preferentially ventilated. Heaf et al. 25 investigated a small cohort of infants and children with lung disease using a radiolabelled tracer gas (krypton-81m) method, and found that infants and children had the reverse ventilation pattern to adults 25. Frerichs et al. 15 were the first to challenge these findings and were able to demonstrate, with EIT measurements, that ventilation in infants is more centrally located. We have previously described a similar ventilation distribution in a small cohort of newborn infants 18. EIT and krypton-81m ventilation scanning have some distinct differences in the way they measure lung volume and regional ventilation. In healthy subjects, the alveolar lung volume remains almost constant during tidal breathing and most of the volume changes (convection) during tidal breathing occur in the central and peripheral airways, and alveolar ducts 26. EIT measurements are based on tidal volume change. Since the alveolar volume in healthy subjects is hardly changing, EIT can not identify these regions unless alveolar recruitment occurs during tidal breathing. Krypton-81m ventilation scanning investigates steady-state ventilation images based on the inhalation of the tracer gas. Hence, images obtained with krypton-81m scanning are both convection- and diffusion-dependent. Infants tend to breathe near the closing volume of the lung, and regional differences in the distribution of the closing volume exist causing partial atelectasis of the dependent lung in spontaneously breathing and sedated infants 2, 27. In the study by Heaf et al. 25, the investigated subjects were sedated and had lung disease. Therefore, their findings of preferential ventilation of the nondependent lung may not apply to healthy nonsedated infants. The differences in regional amplitudes between the anterior and posterior compartments can be further explained by the artificial division of the chest into two compartments. The anterior chest compartment contains the heart as a “nonlung” structure. In the supine position, gravity causes the heart to be suspended from the sternum, occupying a larger space in the anterior compartment, whereas in the prone position, the heart is resting on the sternum, allowing more anterior lung expansion. Our EIT data set will provide a valuable comparison for future studies in subjects with lung disease or during mechanical ventilation, where alveolar recruitment and derecruitment during tidal breathing can occur 26, 28–30.
Time-course analysis
40 yrs ago, regional filling characteristics of the lung were first described in healthy adults using radiolabelled isotopes 10. Theoretically, if lung regions fill homogeneously, the degree of expansion will be consistent throughout the entire lung. It was found that, in an upright position, the change in lung volume (expressed as a percentage of total lung capacity) observed during an inspiratory vital capacity (VC) manoeuvre was greater in the lower regions than in the upper lung regions, and that the right lung filled earlier during a deep inhalation. Asynchrony in regional lung filling was found by Koler et al. 31 using differential bronchospirometers in animal experiments, confirming that lung regions may not fill synchronously. EIT allows the measurement of the asynchronous filling and emptying of different lung regions 12. In the present study, we demonstrated that the dependent lung filled before the nondependent lung, which is consistent with the lung model proposed by Milic-Emili et al. 10 that models the lung as a suspended spring in gravity, with the dependent parts of the spring showing easier expansion. Milic-Emili et al. 10 showed that, during the initial phase of a VC manoeuvre, the rate of volume change was greatest in the nondependent lung, whereas during the end-phase of the inspiration the greatest volume change was found in the dependent lung. In our cohort of infants, we found a similar regional rate of impedance change for all analysed sighs. During tidal breathing, the opposite behaviour was found, with the greatest rate of impedance change during the initial phase of the inspiration in the posterior lung and the greatest rate of impedance change during the end-phase of the inspiration in the anterior lung. To explain these differences, one must consider the mechanism of lung expansion during a VC manoeuvre and the contribution of the diaphragm during tidal breathing. In infants, most of the tidal volume during spontaneous breathing is generated by diaphragm excursion 32 and, to a lesser degree, by the chest wall 33. During tidal breathing, the posterior part of the diaphragm shows the greatest shortening of muscle fibres and, hence, the rate of change in lung volume in these regions will be greater than in the anterior parts of the lung 34. During a sigh, the contribution of the chest wall will proportionally increase to generate the large inspiratory effort 35. The posterior part of the chest will experience proportionally less excursion than the anterior, as the posterior chest wall is splinted by the surface the infant is lying on in supine position 36. The greater change of the anterior lung volume at the beginning of a sigh is caused by chest wall geometry and compliance in the supine position.
Limitations
The observed changes in impedance, both during tidal breathing and as an effect of growth, may not be only contributed by change in air volume, but also by change in blood volume and lung tissue characteristics. The separation of several tissue impedance characteristics can only be obtained with a multifrequency EIT equipment, which currently is not yet available for clinical use. In theory, with a multifrequency EIT, the tissue to air ratio of the lung could be separated and lung growth documented.
Conclusion
Regional ventilation distribution measurements using EIT at 2 weeks, and 3 and 6 months of age showed that the dependent lung is preferentially ventilated and fills ahead of the rest of the lung, a breathing pattern that is similar to adults.
Footnotes
Support Statement
The study was supported by the Golden Casket and Preston James Funds.
Statement of Interest
None declared.
- Received March 4, 2010.
- Accepted June 29, 2010.
- ©ERS 2011
REFERENCES










