





Abstract
Bronchodilator response (BDR) is assessed to estimate the reversibility of airflow obstruction. Bronchial hyperresponsiveness (BHR) is a characteristic feature of asthma and is usually measured by means of bronchial challenges using direct or indirect stimuli. The aim of the present study was to compare BHR to methacholine (direct) and that to adenosine 5’-monophosphate (AMP) (indirect) with regard to their relationships to BDR in asthmatic children.
Methacholine and AMP challenge tests were performed on 138 children with mild-to-moderate asthma, and the provocative concentration causing a 20% decline in forced expiratory volume in 1 s (FEV1) (PC20) was determined for each challenge. BDR was calculated as the change in FEV1, expressed as a percentage of the initial value, after inhalation of 400 μg salbutamol.
Methacholine PC20 correlated significantly but weakly with BDR (r = -0.254; p = 0.003). However, there was a significant and strong correlation between AMP PC20 and BDR (r = -0.489; p = 0.000). For AMP PC20, the relationship was closer than for methacholine PC20 (p = 0.024 for comparison between correlation coefficients). The same figures were observed when BDR was expressed as a percentage of the predicted value.
A stronger correlation of BDR with AMP PC20 than with methacholine PC20 suggests that BDR may be better reflected by BHR as assessed by AMP challenge than by methacholine challenge.
Measurement of bronchodilator response (BDR) is widely applied to assessment of the acutely reversible component of airways obstruction 1. Asthma is traditionally defined as reversible airflow obstruction, although clinicians have long recognised that the obstruction is sometimes not completely reversible 2. In children and adults with asthma, BDR is often used to indicate the degree of reversibility, aid confirmation of the diagnosis, assess the severity of the disease and help make therapeutic decisions 3.
Bronchial hyperresponsiveness (BHR), defined as an exaggerated bronchoconstrictive response of the airways to a variety of stimuli, is considered to be a hallmark of asthma. BHR is most commonly evaluated using methacholine or histamine, which acts directly at the level of bronchial smooth muscle. However, BHR can also be assessed using indirect stimuli, such as adenosine 5’-monophosphate (AMP), which causes bronchoconstriction by stimulating or enhancing the release of mediators from mast cells 4. There is increasing interest in the role of indirect bronchial challenges because symptoms and bronchoconstriction occur in clinical asthma by means of indirect mechanisms 5.
It has been suggested that the assessment of BDR might be a useful guide to the presence of BHR 6. Indeed, provocation challenges, when contraindicated for reason of severe airway obstruction, have been replaced by bronchodilator tests. However, studies on the relationship between BHR to histamine or methacholine and BDR have yielded conflicting results; some found a significant correlation 7–9, whereas others did not 10, 11. Conversely, there is no information as to whether BDR correlates with BHR to indirect stimuli, such as AMP.
In the present study, methacholine and AMP challenge tests and bronchodilator testing were performed, and the degree of BHR to methacholine and to AMP compared with regard to their relationships to BDR in children with asthma.
MATERIAL AND METHODS
Children with mild-to-moderate asthma, aged 7–18 yrs, were enrolled in the present study. They were attending the allergy clinic at Seoul National University Children's Hospital (Seoul, Korea). All subjects had physician-diagnosed asthma and a history of episodic wheezing and/or dyspnoea during the previous year, which was resolved after using bronchodilators. They had been medicated with inhaled short-acting β2-agonists on demand in order to relieve symptoms, with or without controller medications (i.e. inhaled corticosteroids or leukotriene receptor antagonists). Children were excluded if they had a history of near-fatal asthma, major exacerbations necessitating the use of systemic corticosteroids or other respiratory diseases other than asthma.
The present study consisted of a 1-week observational period, followed by methacholine and AMP bronchial challenges during the second week and bronchodilator testing in the third week (fig. 1). At the start of the observational period, the patients were asked to discontinue their controller medications, if used, and to use only inhaled β2-agonists on demand during the entire study period. During the second week, each subject was evaluated using a battery of tests, including blood eosinophil counts, total serum immunoglobulin E measurements and skin-prick tests. Atopy was defined as the presence of at least one positive skin reaction (weal major diameter of >3 mm) to a battery of 12 common airborne allergens. On each of the 2 days (≥3 but ≤6 days apart) during the second week, either a methacholine or an AMP challenge test was performed. The sequence of these challenges was randomised in order to preclude any bias related to potential carry-over effects. In order to be eligible for the present study, the subjects had to be able to undergo pulmonary function tests in a reproducible way (i.e. the two largest forced expiratory volumes in 1 s (FEV1) were within 5% of each other after three acceptable spirograms had been obtained) and were required to have an FEV1 of ≥60% of the predicted value 12. During the third week, bronchodilator testing was performed. Subjects were excluded from the study if an exacerbation of asthma or a respiratory tract infection had occurred within 4 weeks prior to the tests, or if they showed an unstable FEV1 (difference in baseline FEV1 of ≥10% pred between methacholine and AMP challenge).

Schematic flow chart showing study design. The first week was an observational period. The order of the methacholine (□) and adenosine 5’-monophosphate (▓) challenge tests was randomised. ▪: bronchodilator test. Vertical arrow indicates discontinuation of controller medication.
Methacholine and AMP challenge tests
Methacholine inhalation tests were carried out using a modification of the method described by Chai et al. 13, and AMP challenge tests were performed using a modification of the European Respiratory Society (ERS) method 14. Inhaled short-acting β2-agonists were withheld for ≥8 h and other medications for 3 days before each challenge. Fresh solutions of methacholine and AMP were prepared in buffered saline solution at various concentrations of methacholine (0.075, 0.150, 0.3125, 0.625, 1.25, 2.50, 5.00, 10.0, 25.0 and 50.0 mg·mL−1) and AMP (3.125, 6.25, 12.5, 25.0, 50.0, 100, 200 and 400 mg·mL−1). Lung function was measured using a computerised spirometer (Microspiro-HI 298; Chest, Tokyo, Japan), and the largest value of triplicate FEV1 on each occasion was used for analysis. A Rosenthal–French dosimeter (Laboratory for Applied Immunology; Baltimore, MD, USA), triggered by a solenoid valve set to remain open for 0.6 s, was used to generate an aerosol from a DeVilbiss 646 nebuliser (DeVilbiss Health Care; Somerset, PA, USA), with air pressurised at 20 psi. Each subject inhaled five inspiratory capacity breaths of buffered saline solution and increasing concentrations of methacholine or AMP, respectively, at 5-min intervals. This gave a mean±sd output of 0.009±0.0014 mL per inhalation. FEV1 was measured 90 s after inhalation at each concentration. The procedure was terminated when the FEV1 had decreased by >20% of its post-saline value or when the highest methacholine (50.0 mg·mL−1) or AMP (400 mg·mL−1) concentration was reached. The percentage decline in FEV1 from the post-saline value was plotted against the logarithmic concentration of inhaled methacholine or AMP. The provocative concentration causing a 20% fall in FEV1 (PC20) for methacholine and AMP were calculated by interpolating between two adjacent data points when the FEV1 decreased by >20%. Censored values of 100 mg·mL−1 for methacholine PC20 and 800 mg·mL−1 for AMP PC20 were given to those who did not show a 20% decline in FEV1 after inhalation of the maximal concentration of methacholine (50.0 mg·mL−1) or AMP (400 mg·mL−1).
Bronchodilator testing
Bronchodilator testing was performed as indicated by the ERS Task Force team 15. Lung function was measured before and 15 min after inhalation of 400 μg salbutamol aerosol (Ventolin Evohaler; GlaxoSmithKline, London, UK), which was administered as four separate doses of 100 μg via a spacer (AeroChamber Plus; Trudell Medical International, London, ON, Canada). BDR was assessed in two ways: 1) change (δ) in FEV1 as a percentage of the initial value (post-bronchodilator FEV1 minus pre-bronchodilator FEV1, expressed as percentage increase over pre-bronchodilator FEV1); and 2) δFEV1 as a percentage of the predicted value (post-bronchodilator FEV1 minus pre-bronchodilator FEV1, expressed as a percentage of the predicted value).
Parents gave written informed consent for their children to participate in the study. The study protocol was approved by the Institutional Review Board of Seoul National University Hospital.
Statistical analysis
Data are presented as mean±sd or geometric mean and 1-sd range. FEV1 are expressed as a percentage of the predicted value. Subjects were considered to show BHR to methacholine or AMP when their methacholine PC20 was <16 mg·mL−1 16 or when their AMP PC20 was <200 mg·mL−1 17. PC20 were logarithmically transformed before statistical analysis. Correlations between PC20 and BDR or blood eosinophil counts were calculated using Spearman's rank-order method. Correlation coefficients were compared using Fisher's z-transformation and a two-tailed z-test 18. A p-value of ≤0.05 was considered significant. All analyses were performed using the statistical software SPSS version 17.0 (SPSS, Inc., Chicago, IL, USA).
RESULTS
A total of 169 children with mild-to-moderate asthma were enrolled in the present study. Of these children, 31 were subsequently excluded because of the occurrence of asthma exacerbations or respiratory tract infections (n = 11), unstable or low FEV1 (n = 6), failure to undergo methacholine or AMP challenges according to the schedule (n = 8), failure to undergo bronchodilator testing (n = 4) or incomplete data due to other causes (n = 2).
The characteristics of the 138 patients whose data were complete are presented in table 1. There was no significant difference in baseline FEV1 before the methacholine and AMP challenges (90.2±13.1 versus 91.0±12.7% pred). The geometric mean (95% confidence interval) of methacholine PC20 was 1.99 (1.57–2.52) mg·mL−1, and that of AMP PC20 was 37.6 (27.6–51.2) mg·mL−1. A total of 128 (92.8%) patients had a methacholine PC20 of <16 mg·mL−1, the cut-off point for BHR to methacholine. Conversely, 116 (84.1%) subjects exhibited BHR to AMP (PC20 of <200 mg·mL−1). The pre-bronchodilator FEV1 (88.9±11.9% pred) were not significantly different from the baseline FEV1 before methacholine and AMP challenge; 105 (76.1%) subjects had a pre-bronchodilator FEV1 of ≥80% pred. The post-bronchodilator FEV1 was 96.2±11.6% pred; the majority (n = 127; 92.0%) exhibited a value of ≥80% pred. The overall increase in FEV1 following inhalation of salbutamol, expressed as a percentage of the initial value and of the predicted value, was 8.44±5.13% initial and 7.29±3.92% pred, respectively.
The relationship between methacholine PC20 and δFEV1 (% initial or % pred) is shown in figure 2. Both δFEV1 (% initial) (fig. 2a) and δFEV1 (% pred) (fig. 2b) correlated significantly with methacholine PC20 (r = -0.254; p = 0.003 and r = -0.212; p = 0.013, respectively).
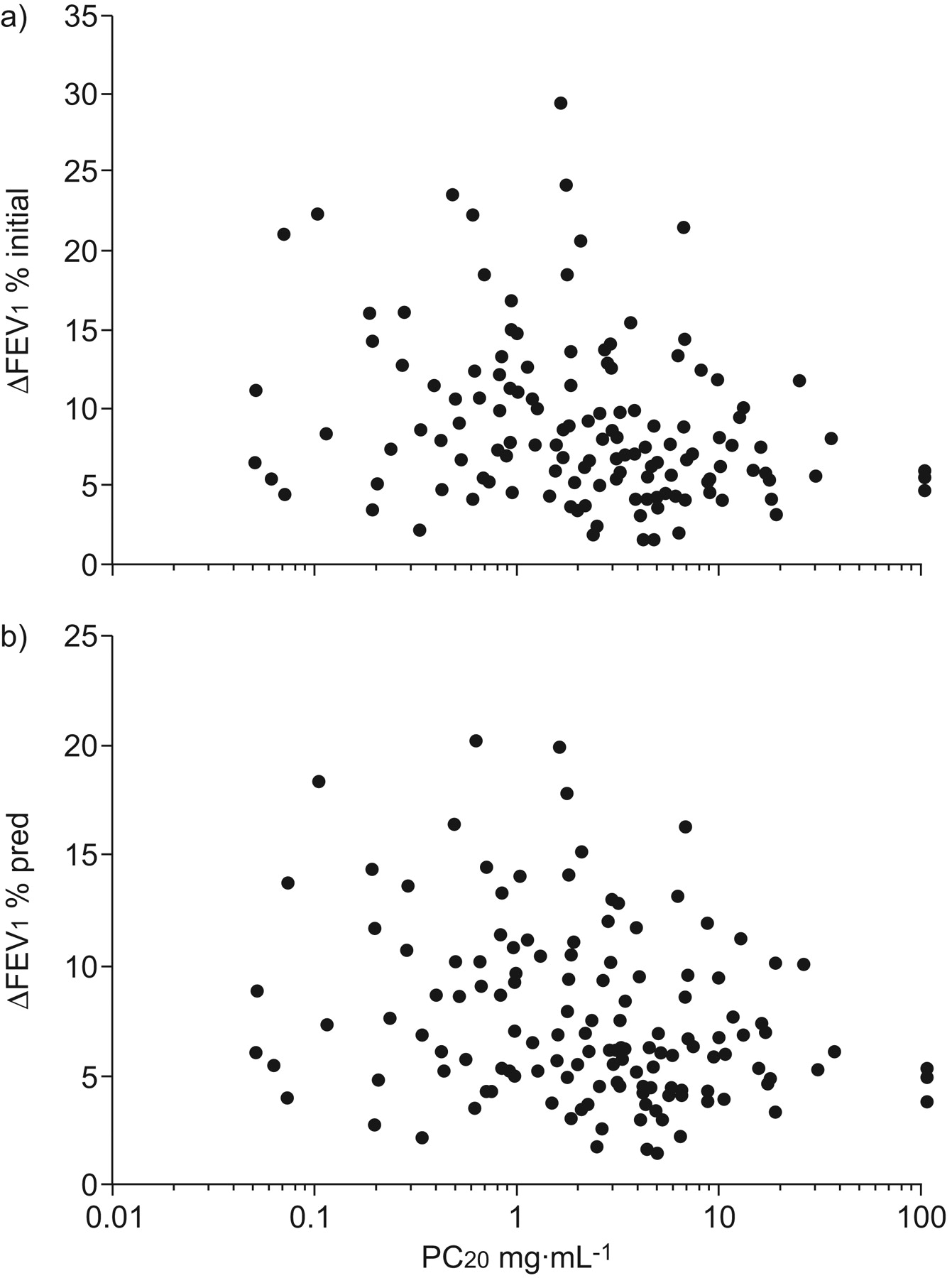
Scatter plots showing the change in (δ) forced expiratory volume in 1 s (FEV1) against the provocative concentration of methacholine causing a 20% fall in FEV1 (PC20), with FEV1 expressed as: a) the percentage increase over the initial value (r = -0.254; p = 0.003); and b) percentage increase over the predicted value (r = -0.212; p = 0.013).
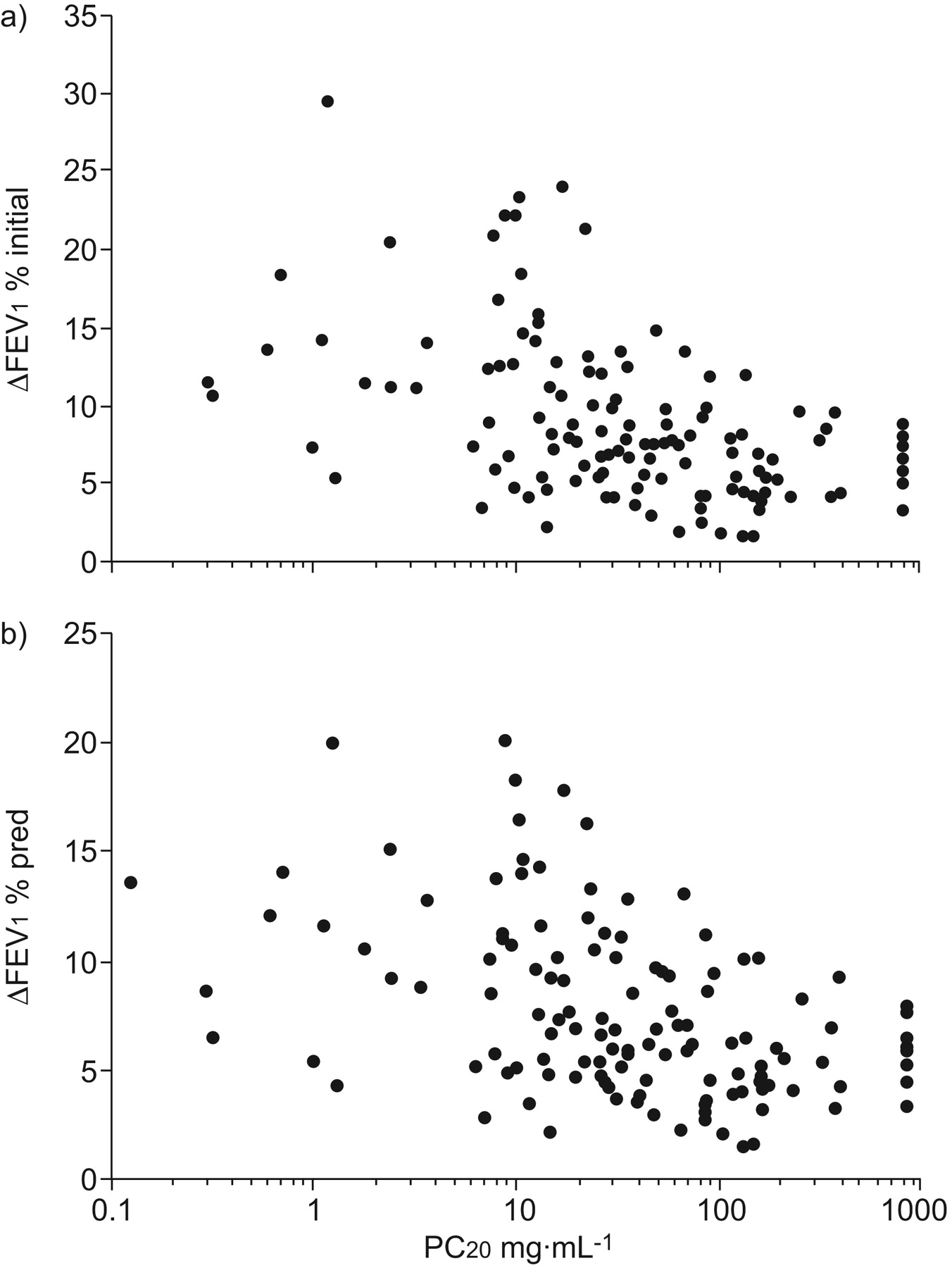
The relationship between AMP PC20 and δFEV1 (% initial or % pred) is shown in figure 3. Both δFEV1 (% initial) (fig. 3a) and δFEV1 (% pred) (fig. 3b) correlated significantly with AMP PC20 (r = -0.489; p = 0.000 and r = -0.448; p = 0.000, respectively).
{kind=link}
{kind=link}
{kind=link}
Scatter plots showing the change in (δ) forced expiratory volume in 1 s (FEV1) against the provocative concentration of adenosine 5’-monophosphate causing a 20% fall in FEV1 (PC20), with FEV1 expressed as: a) the percentage increase over the initial value (r = -0.489; p = 0.000); and b) percentage increase over the predicted value (r = -0.448; p = 0.000).
The correlation between AMP PC20 and δFEV1 (% initial) was significantly stronger than that between methacholine PC20 and δFEV1 (% initial) (p = 0.024 for the comparison of correlation coefficients of -0.489 and -0.254). The correlation between AMP PC20 and δFEV1 (% pred) was also significantly higher than that between methacholine PC20 and δFEV1 (% pred) (p = 0.029 for the comparison of correlation coefficients of -0.448 and -0.212).
When the analysis was confined to 109 subjects who were steroid-naive, both methacholine PC20 and AMP PC20 correlated significantly with δFEV1 (% initial) (r = -0.279; p = 0.003 and r = -0.543; p = 0.000, respectively). They also correlated significantly with δFEV1 (% pred) (r = -0.242; p = 0.011 for methacholine PC20; r = -0.501; p = 0.000 for AMP PC20). The relationships of δFEV1 (% initial and %pred) with AMP PC20 were significantly closer than those with methacholine PC20, respectively (p = 0.021 for the comparison of correlation coefficients of -0.543 and -0.279, and p = 0.028 for the comparison of correlation coefficients of -0.501 and -0.242; data not shown).
The δFEV1 (% initial) was calculated according to the presence/absence of BHR to methacholine and BHR to AMP, respectively, and the number of subjects with a positive and negative BDR, with a cut-off of 9% 19, in each category are presented in table 2. The δFEV1 (% initial) was significantly higher in subjects with BHR to methacholine than those without (p = 0.032). The same figures were observed between subjects with BHR to AMP and those without (p = 0.043). A positive BDR was associated with BHR to methacholine with a high positive predictive value (98%), but a negative BDR does not exclude it (negative predictive value of 10%). Likewise, the positive and negative predictive value of BDR testing for BHR to AMP was 96 and 22%, respectively.
There was an inverse correlation between AMP PC20 and blood eosinophil count (r = -0.237; p = 0.005), but not between methacholine PC20 and blood eosinophil count (r = -0.059; p = 0.488) (data not shown).
DISCUSSION
In the present study, the relationship between BDR and bronchial responsiveness, assessed by methacholine and AMP challenge, was investigated. Although both methacholine PC20 and AMP PC20 correlated significantly with BDR, the correlation was stronger for AMP PC20 than for methacholine PC20. To the best of our knowledge, this is the first study to compare methacholine and AMP responsiveness with regard to their relationships to BDR in children with asthma.
BDR is usually measured by changes in airflow before and after administration of β2-agonists. Most commonly, it is expressed as the percentage increase in FEV1 over the initial value. The BDR of the present asthmatic subjects, expressed in this manner, averaged 8.44%, which was comparable to that of other studies. Tantisira et al. 20 reported a mean BDR of 10.07% among the 1,041 participants in the Childhood Asthma Management Program. Galant et al. 21 observed various mean BDRs according to clinical severity, ranging from 7.3 (mild intermittent group) to 10.1% (severe persistent group). There is no clear consensus as to what constitutes significant reversibility in subjects with airflow obstruction. A recent report suggested that a ≥9% BDR cut-off point best distinguishes children with asthma from those without 19. According to this criterion, it was found that 47 (34.1%) of 138 children with asthma exhibited a positive BDR. This is in line with previous reports that a large proportion of patients with asthma do not show a positive BDR, which strengthens the suggestion that BDR provides only modest sensitivity in confirming the diagnosis of asthma 21.
In the present study, methacholine and AMP challenge tests were performed during the second week in randomised order. The low-dose inhaled corticosteroids administered to most of the subjects requiring controller therapy are reported to have short-lived (within 1 week) effects on methacholine and AMP reactivity after treatment is stopped 22, 23. Conversely, the time course of changes in BDR following inhaled corticosteroid withdrawal has not been studied. Therefore, bronchodilator testing was set to be performed during the third week in order to minimise any effect of corticosteroids.
It has been suggested that BDR is the physiological opposite of bronchoconstrictor responsiveness 6, 9, and, therefore, that bronchial challenge tests can be replaced by bronchodilator tests in subjects with airway obstruction. Several studies have shown that BDR is associated with histamine or methacholine responsiveness in both children and adults with asthma 7–9. Similarly, we found a significant, albeit weak, correlation between BDR and methacholine PC20. On the contrary, there are other reports that BDR is not related to methacholine responsiveness 10, 11. The reasons for these conflicting data are unclear, but they are presumably due to confounding factors such as airway remodelling. It is hypothesised that airway wall thickening results in disproportionately severe airway narrowing and thus leads to exaggerated BHR 24. This hypothesis is supported by studies showing a significant relationship between BHR to methacholine and the degree of airway wall thickening 25. Conversely, airway remodelling may be an important mechanism that leads to fixed airflow obstruction in asthma 26.
It has not previously been studied whether BDR is related to BHR assessed by indirect challenge tests. Given that indirect challenges more closely reflect the mechanisms via which clinical asthma manifests itself 5, it is surprising that little information is available regarding this relationship. In the present study, BDR correlated significantly with AMP PC20. Furthermore, BDR correlated more strongly with AMP PC20 than with methacholine PC20 (p = 0.024 for comparison of correlation coefficients). The results of the present study suggest that airway reversibility is more closely associated with bronchial responsiveness assessed by AMP than by methacholine in asthma. To the best of our knowledge, this is the first study to have compared methacholine and AMP responsiveness with regard to their relationships to BDR.
When BDR is expressed as the percentage increase in FEV1 over the initial value, small absolute δFEV1 may be exaggerated to be larger in patients with a reduced baseline FEV1. It has been suggested that relating the δFEV1 to the predicted value may be more appropriate 27, because it eliminates the influence of not only the initial value but also sex, age and height. In the present study, however, a closer relationship of BDR with AMP PC20 than with methacholine PC20 persisted (p = 0.029 for comparison of correlation coefficients), even when δFEV1 was evaluated based on the predicted value instead of the initial value.
It is possible that inhaled corticosteroids used as a controller medication may have confounded the results, although they were discontinued ≥1 week before the study. However, when the analysis was restricted to steroid-naive subjects, the same figures were observed.
It is expected that individuals who are maximally bronchodilated at baseline will exhibit minimal BDR, and vice versa. Thus, BDR, even expressed as percentage predicted, is dependent upon the pre-bronchodilator value 28. Conversely, for bronchial challenge tests, a given stimulus provokes a larger bronchoconstrictor response in a subject with more severe obstruction than in a subject with less severe obstruction, resulting in a lower PC20 16. As a result, the severity of both methacholine PC20 and AMP PC20 would be affected by baseline airway calibre. One may argue that the present finding, i.e. a stronger association of BDR with AMP PC20 than with methacholine PC20 may be due to a differential influence of baseline airway calibre on AMP PC20 and methacholine PC20. However, this seems unlikely because methacholine responsiveness is more strongly related to diminished airway calibre than is AMP responsiveness 29.
The reason why BDR is more linked to AMP responsiveness than to methacholine responsiveness is not clear but speculative. Clinical studies in asthmatics have shown that BHR to AMP reflects the underlying bronchial inflammation more accurately than BHR to methacholine 30. This hypothesis is supported by the present observation of a significant correlation between blood eosinophil counts and AMP PC20 but not methacholine PC20. Several authors have investigated the association of BDR with biomarkers of inflammation, including exhaled nitric oxide and bronchial eosinophilia. Covar et al. 31 reported that the level of exhaled nitric oxide was significantly higher in children who showed ≥12% BDR than that in those who did not. Faul et al. 32 reported that the changes in eosinophils in bronchial biopsy specimens correlated with those in BDR 8 weeks after corticosteroid therapy in atopic children with asthma. Thus a higher BDR would be associated with increased inflammatory events in the airways, the extent of which may be more specifically reflected by AMP responsiveness than by methacholine responsiveness.
The correlations between both AMP and methacholine responsiveness and BDR were, albeit significant, not strong. It should be taken into account that bronchodilator testing and the two challenge tests use different stimuli to elicit the response. Another factor that should be considered is the different nature of the tests. Bronchodilator testing is a one-shot test, which is more analogous to exercise challenge, whereas the two challenge tests use a progressive dose–response method.
A positive BDR, defined as a δFEV1 of ≥9% initial, was suggestive of BHR to methacholine or BHR to AMP, with a high predictive value. However, because many patients with BHR to methacholine or BHR to AMP gave a negative BDR result, the predictive value of BDR testing for BHR to methacholine or AMP is quite limited.
In summary, it was found that BDR correlated significantly with not only methacholine responsiveness but also AMP responsiveness. The comparison of correlation coefficients revealed that BDR was more linked to AMP responsiveness than to methacholine responsiveness. The results of the present study suggest that BDR may be better reflected by bronchial responsiveness as assessed by AMP challenge than by methacholine challenge.
Footnotes
Support Statement
This study was supported, in part, by grant No. 04-2009-048-0 from the Seoul National University Hospital (Seoul, Korea) Research Fund.
Statement of InterestNone declared.
- Received August 28, 2010.
- Accepted November 1, 2010.
- ©2011 ERS
REFERENCES










