





Abstract
We investigated determinants of change in bronchial reactivity in the Swiss Cohort Study on Air Pollution and Lung Diseases in Adults (SAPALDIA), a population-based cohort with wide age range (29–72 yrs at follow-up).
The role of sex, age, atopic status, smoking and body mass index (BMI) on percentage change in bronchial reactivity slope from the baseline value was analysed in 3,005 participants with methacholine tests in 1991 and 2002, and complete covariate data. Slope was defined as percentage decline in forced expiratory volume in 1 s from its maximal value per micromole of methacholine.
Bronchial hyperreactivity prevalence fell from 14.3 to 12.5% during follow-up. Baseline age was nonlinearly associated with change in reactivity slope: participants aged <50 yrs experienced a decline and those above an increase during follow-up. Atopy was not associated with change, but accentuated the age pattern (p-value for interaction = 0.038). Smoking significantly increased slope by 21.2%, as did weight gain (2.7% increase per BMI unit). Compared with persistent smokers, those who ceased smoking before baseline or during follow-up experienced a significant decrease in slope (-27.7 and -23.9%, respectively). Differing, but not statistically different, age relationships and effect sizes for smoking and BMI between sexes were found.
Mean bronchial reactivity increases after 50 yrs of age, possibly due to airway remodelling or ventilation–perfusion disturbances related to cumulative lifetime exposures.
- Adult
- bronchial hyperreactivity
- cohort studies
- epidemiologic determinants
- methacholine chlorine
- population
Although elevated bronchial reactivity plays a major role in asthma 1, the determinants of its change over time have not been extensively researched.
In cross-sectional studies, bronchial reactivity was inversely associated with airway size 2, 3 and positively associated with atopy 4, 5. Smoking has not consistently been shown to increase reactivity 5–8 and a sex difference beyond airway size is debated 3, 8, 9.
Longitudinal change in bronchial reactivity in the general population has only been investigated by a few cohort studies. In the Normative Aging Study, bronchial reactivity at follow-up was positively correlated with baseline blood basophil counts 10. New-onset bronchial hyperreactivity (BHR) was associated with both low and high baseline body mass index (BMI), and linearly with change in BMI 11. In the European Community Respiratory Health Survey (ECRHS), baseline smokers had higher bronchial reactivity at follow-up 12, and an interaction between allergic sensitisation and sex was found: persistent sensitisation was associated with a reactivity decrease in females but not males 12. Baseline allergic rhinitis was associated with incident BHR and increased bronchial reactivity at follow-up 13. Finally, a small study on volunteers from UK general practices showed seasonal patterns, with higher reactivity during summer and winter months 14.
These findings suggest that change in bronchial reactivity might differ between sexes and is influenced by both allergic conditions and inflammatory processes. Still, knowledge on longitudinal determinants is limited: bronchial reactivity is highly variable in repeated assessments 15, and the cited studies had either short follow-up 14, 11 or restricted age range 13 or sex 11. There is, thus, a knowledge gap on longitudinal determinants in older populations including males and females. As major pulmonary diseases, such as chronic obstructive pulmonary disease and asthma, increase either in prevalence 16 or severity 17 with age and exhibit important sex differences 18, 19, investigating the timecourse of bronchial reactivity in aged populations is important.
The Swiss Cohort Study on Air Pollution and Lung Diseases in Adults (SAPALDIA) with its population-based sample aged 29–72 yrs at follow-up, detailed health questionnaire data, allergy testing, standardised spirometry and methacholine testing, provides an opportunity to fill this gap.
Thus, we aimed to assess the longitudinal impact of sex, age, atopic status, smoking and BMI on change in bronchial reactivity over the whole age range of the SAPALDIA population.
METHODS AND MATERIALS
Study design and population
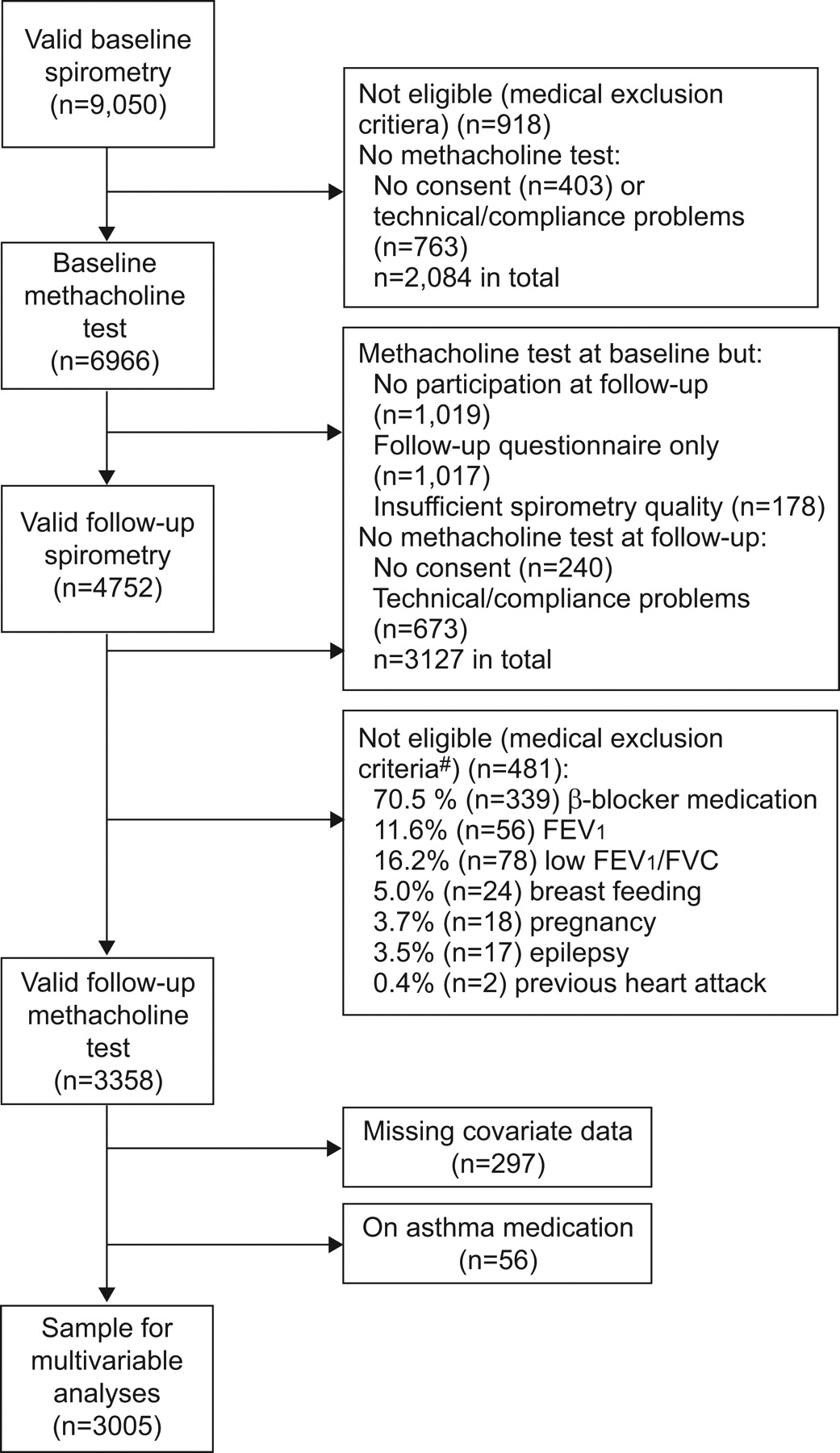
The SAPALDIA study methodology has been published previously 20. Briefly, 6,966 randomly selected, 18–60-yr-old adults from eight areas of Switzerland underwent health interview, spirometry and bronchial reactivity testing with methacholine in 1991. At follow-up in 2002, 3,358 underwent the same assessments (fig. 1). 3,005 participants with complete covariate data and no asthma medication were available for multivariable analysis.

Selection of study participants. FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity. #: numbers do not sum to 100% as some participants met several criteria.
All participants gave written consent, and the study was approved by the Swiss Academy of Medical Sciences and local ethics committees.
Assessment procedures
Health questionnaire
Study participants underwent a health interview on respiratory symptoms, pre-existing pulmonary diseases, smoking behaviour, environmental tobacco smoke (ETS) exposure at home or work, medication use and socioeconomic factors.
Never-smokers had smoked <20 packs of cigarettes or <360 g of tobacco during their lifetime 21. Ex-smokers had quit smoking at least 30 days before the interview, and current smokers reported active smoking 21. We defined six categories of longitudinal smoking behaviour: persistent never-smokers, ex-smokers and smokers for those with unchanged exposure, quitters for baseline smokers becoming ex-smokers at follow-up, uptakers for baseline never-smokers becoming current or ex-smokers at follow-up, and intermittent smokers for the rest.
Asthma was defined as an affirmative answer to both questions “Have you ever had asthma?” and “Was this confirmed by a doctor?”. Asthma medication was defined by current intake of inhalers, aerosols or tablets for asthma. Chronic cough was defined as cough during the day or in the morning for ≥3 months·yr−1 in the previous 2 yrs. Wheezing was present if occurring unrelated to a cold in the 12 months prior to examination.
Spirometry
Following the ECRHS protocol 22, participants underwent three to eight forced expiratory lung function manoeuvres to achieve a minimum of two measurements complying with American Thoracic Society criteria 23.
Bronchial reactivity testing
After a starting inhalation of physiological saline solution, methacholine was administered by MEFAR® aerosol dosimeters using progressive four-fold solutions of 0.39, 1.56, 6.25 and 25 mg·mL−1. Starting from functional residual capacity, participants inhaled to the total lung capacity and held their breath for 4 s. Two forced expiratory manoeuvres were performed 1 and 2 min after inhalation, and the larger forced expiratory volume in 1 s (FEV1) measurement was recorded. If FEV1 fell >10% from the post-saline level, intermediate, two-fold concentrations were applied. No testing was done if FEV1 after saline inhalation fell below 90% of the maximum spirometry value. The test was stopped if FEV1 fell by ≥20% from post-saline measurement, or if a cumulative methacholine dose of 2 mg was reached.
Bronchial reactivity was defined by dose–response slope, similarly to the method employed by O'Connor et al. 24: percentage decline in FEV1 (relative to the maximal test value) divided by the cumulative methacholine dose in micromoles. BHR was defined as FEV1 decline of ≥20% from the post-saline measurement up to 2 mg of methacholine.
Test exclusion criteria were myocardial infarction within the last 3 months, severe cardiac failure, β-blocker medication (including eye drops), epilepsy, pregnancy, lactation, FEV1/forced vital capacity (FVC) ratio <80% and FEV1 <70% predicted.
Allergic sensitisation
In both examinations, atopic sensitisation was assessed by Phadiatop® tests (Phadia, Uppsala, Sweden), radioimmune assays detecting serum immunoglobulin E antibodies to common inhalatory antigens, such as pollen, household dust mite and animal epithelia 25. Positive tests had activity levels ≥0.35 kU·L−1 (for any allergen) and defined atopy.
Statistical analysis
After adding a small constant (0.01) to each, bronchial reactivity slopes were naturally logarithmised to achieve a more symmetrical distribution 3.The difference between follow-up minus baseline logarithm was used as outcome measure and corresponds to the logarithmised follow-up over baseline slope ratio, as shown below:
Exponentiation of regression estimates thus yields geometric means and confidence limits of slope ratios. For clearer interpretation, exponentiated coefficients were expressed as percentage changes from baseline slope (e.g. an exponentiated coefficient of 1.03 as 3% increase).
To study the effect of selection processes at different stages, characteristics of participants with follow-up methacholine testing, complete covariate data and no asthma medication were compared to those assessed only at baseline, either solely by spirometry (n = 2,084) or including methacholine test (n = 3,127), using Chi-square, Wilcoxon rank sum and unpaired t-tests.
BHR prevalence and median reactivity slopes at both examinations were described.
Determinants of the logarithmised follow-up over baseline slope ratio were investigated by multivariable mixed linear models including sex, age, allergic sensitisation, BMI, change in BMI, current and ex-smoking, exposure to passive smoke, adjustment for concurrent colds at either examination, sinus and cosinus terms modelling seasonal cyclicity, and random effects for study areas. Continuous covariates, such as age, BMI and pack-years, were also modelled using natural cubic splines specifying five knots positioned as recommended by Harrell 26. Pack-yrs smoked in smokers, ex-smokers or both were entered instead of smoking variables. Changes in smoking behaviour were assessed by replacing baseline smoking variables with the categories persistent never-smokers (n = 1,349), ex-smokers (n = 606), uptakers (n = 99), quitters (n = 250) and intermittent smokers (n = 100) in a model relating to persistent smokers (n = 601) as reference. Effects of airway calibre and lung size were not of primary interest, but models were controlled for baseline FEV1, FVC and forced expiratory flow at 25–75% (FEF25–75%) (the latter pre-adjusted for sex and FEV1). Participants reporting asthma medication at either examination were expected to influence the observed associations significantly and were thus excluded (n = 56).
Robust standard errors were computed to account for heteroscedasticity in residuals. Two-sided significance levels were chosen at α = 0.05 for main effects and α = 0.1 for interactions.
Several sensitivity analyses were conducted. In order to assess to what extent effects of study covariates were mediated by lung function and its change, we applied different adjustments to the models, including change in FEV1, FVC and FEF25–75%, calculated as follow-up minus baseline value, to the baseline variables, replacing lung function variables by % pred values for FEV1 and FVC 27, and their corresponding change, and leaving out all lung function variables. We checked whether covariate coefficients and p-values were unaltered by the adjustments.
To study the impact of selection processes, we re-ran multivariable analyses, giving more weight to under-represented study participants. Weights consisted of the inverse probability of having methacholine testing at both examinations, as calculated by regressing participation on the same baseline covariates as in the multivariable analyses plus doctor-diagnosed asthma and baseline BHR. Finally, regression analyses were re-run after excluding doctor-diagnosed asthma at either examination.
All statistical analyses were performed using STATA version 9.2 (StataCorp, College Station, TX, USA) and SAS Software version 9.1 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Characteristics of the study populations
Briefly, 49.1% of our study participants with complete data on covariates and no asthma medication (n = 3,005) were female, 28.3% were current smokers, 29.4% atopic, 12.9% hyperreactive and 3.7% asthmatic (see online supplementary table O1). Subjects in this sample were significantly less smoking-exposed, asthmatic and hyperreactive, had better lung function values, and less wheezing and chronic cough than participants with only baseline spirometry or methacholine test. Main reasons for missing baseline methacholine tests were medical exclusions (n = 918) and technical/performance problems (n = 763), while at follow-up, missing data were largely due to complete nonparticipation (n = 1,019) or questionnaire assessment only (n = 1,017). 481 follow-up participants met exclusion criteria for methacholine testing (fig. 1). As would be expected, they fared worse regarding smoking, asthma prevalence, hyperreactivity, lung function and respiratory symptoms than our multivariable analysis sample (data not shown).
Prevalence of BHR and bronchial reactivity slope at either examination
3,358 participants with methacholine testing at both examinations, but not necessarily complete data on covariates, were analysed descriptively (online supplementary table O2). BHR prevalence fell significantly by -1.8% from 14.3 to 12.5% (McNemar p = 0.0054). Only 46.8% of the 479 BHR cases at baseline persisted to follow-up. 6.8% of 2,879 previously normoreactive participants became hyperreactive (n = 195).
The median bronchial reactivity slope fell from 1.00 to 0.93% FEV1 decline·μmol methacholine−1.
Determinants of change in bronchial reactivity slope
Analyses were based on 3,005 participants with follow-up methacholine testing, complete covariate data and no asthma medication.
Main effects of determinants
No significant association between sex and change in reactivity slope presented after controlling for baseline lung function (table 1). When modelled with spline functions, age was nonlinearly associated with the change in reactivity slope: subjects aged <50 yrs at baseline experienced a decline over the subsequent 11 yrs of follow-up (fig. 2a). The decline was largest around 30 yrs, diminished continuously afterwards and at 50 yrs, a change in direction occurred, with an observable increase thereafter. In participants aged ≥30 yrs, the reactivity slope increased significantly by 1.5% (95% CI 0.7–2.3%) per year. BMI increase, but not its baseline value, was associated with an increase in reactivity slope of 2.7% (95% CI 0.3–5.2%) per BMI unit. Current baseline smokers experienced a 21.2% (95% CI 7.5–36.7) increase in reactivity slope compared to never-smokers, corresponding to a 3.6% (95%CI 1.6–5.6%) increase per 5 pack-yrs. There were no associations between exposure to ETS or atopy at baseline and change in reactivity slope.

Mean change in bronchial reactivity slope over 11 yrs of follow-up according to age at baseline in a) the whole study sample, b) males and c) females. Bronchial reactivity slope is defined as percentage decline in forced expiratory volume in 1 s per micromole of methacholine. –—: mean; –---: 95% CI.
Interactions between determinants
Sex
Plotting covariate-adjusted age estimates using spline functions suggested different time courses of change in reactivity slope between males and females (fig. 2b and c). Smoking at baseline appeared to increase slope more in females than males (25.0 versus 16.7%, respectively), while for BMI increase, the opposite was observed (5.4% increase in males versus 0.9% in females) (table 2). However, none of these sex differences were statistically significant.
Atopy
Atopic sensitisation showed a significant interaction with age (table 3): the nonlinear age relationship detected in the whole study sample was more pronounced in atopic, but weaker in nonatopic, subjects. When modelling age with polynomial functions, a significant interaction between atopy and the quadratic age term was observed (p = 0.038). This model was significantly better than assuming no interaction (p = 0.027).
Smoking at baseline was associated with a large and significant increase of 39.1% (95% CI 12.2–72.6%) in atopic persons only. However, the interaction with atopy became significant only when analysing pack-yrs (p-value for interaction (pinteraction) = 0.044).
Smoking
The nonlinear relationship between age and change in reactivity slope was most pronounced in nonsmokers (fig. 3), and appeared different in ever-smokers (pinteraction = 0.073). In current and ex-smokers, the turning point to increasing slope occurred earlier, around age 40 yrs, and no linear increase in slope was observed thereafter. Effect estimates for the other covariates remained unaffected by smoking status.

{kind=link}
{kind=link}
{kind=link}
Mean change in bronchial reactivity slope over 11 yrs of follow-up according to baseline smoking status. Bronchial reactivity slope is defined as the percentage decline in forced expiratory volume in 1 s per micromole of methacholine. ○: ever-smokers; •: never-smokers.
Compared with persistent smokers, participants quitting smoking before the first examination or during follow-up experienced a 27.7% (95% CI 15.9–37.9%) and 23.9% (95% CI 6.8–37.8%) decline in bronchial reactivity slope respectively (table 4), which was comparable to persistent never-smokers (-24.6% decline, 95% CI 14.5–33.5%).
BMI
No significant interactions were found for BMI at baseline or its change.
Sensitivity analyses
Effect estimates and strengths of associations for age, smoking, change in BMI and atopy were unaffected by the method of adjustment for change in lung function (online supplementary table O3). However, when using % pred values and corresponding change for FEV1 and FVC, female sex was significantly associated with a decrease in reactivity slope by 13.8% (95% CI 4.2–22.4%). As the only lung function variable significantly associated with change in reactivity slope, decline in FEV1 % pred increased slope by 1.2% (95% CI 0.3–2.1) for each percent decline.
Repeating regression analyses with weights for each observation inverse to the probability of participation yielded the same results.
Exclusion of participants with doctor-diagnosed asthma resulted in similar smoking effect estimates for males and females, but no significant alterations of other estimates (data not shown).
DISCUSSION
In our general population sample of 29–72-yr-old adults, we found a 1.8% decrease in BHR prevalence and a 7% decrease in median reactivity slope over the course of 11 yrs. We observed a significant negative association of female sex with change in reactivity slope only after controlling for lung function using % pred values. These reflect the sex-specific deviation in lung function from an age- and height-dependent expected value, and preclude the assumption of equal effects of a given absolute lung volume or change in both sexes. But they do not take account of smaller absolute airway sizes in females, which might importantly influence the concentration of the stimulus at the airway walls. In accordance with other studies 12, we have found no sex effect once baseline lung function values were controlled for. The observed sex-specific age relationships of reactivity suggest different age-courses of bronchial reactivity between sexes, maybe due to a higher level of reactivity as a consequence of smaller airway size in females. Additionally, the apparent stronger smoking effect suggests higher susceptibility to environmental exposures in females.
Our findings relating to the nonlinear association of change in bronchial reactivity slope with age are new and not described by previous longitudinal studies. These mostly focused on other determinants 11–13 and differed regarding age distribution. An age-associated increase in bronchial reactivity has been described in cross-sectional studies 28. At the time of our own cross-sectional analysis 3, participants were 11 yrs younger and the switch occurring in older age was not detectable. Based on the limited literature on bronchial reactivity in older populations, we can only speculate about possible mechanisms. Airway remodelling or ventilation–perfusion disturbances, which increase bronchial reactivity 29, 30, might be induced by cumulative, lifetime exposures to different noxious substances. Furthermore, loss of tissue elasticity in the ageing lung might cause a tendency for airway closure and air trapping with increased residual volume. It is likely that these mechanisms are not adequately captured in our models, even those including change in lung function.
In accordance with other studies 10, 12, we did not observe a direct effect of atopy on change in reactivity slope. But atopy accentuated the relationship with age and enhanced smoking effects. We found a strong, positive relationship between smoking and change in reactivity slope, a finding inconsistently described 10, 12, possibly due to shorter follow-up times. Profitting from the large sample size of our study, we could also show that quitting smoking has a profound beneficial effect on change in reactivity. Power to assess effects of taking up smoking was, however, limited.
Finally, we observed that change in BMI, but not its baseline value, was positively associated with change in reactivity slope. These effects could be mediated by increased levels of subclinical inflammation from adipose tissue. Our study benefitted from a relatively large sample size, wide age distribution for both sexes, standardised spirometry and methacholine testing, and detailed health interviews. However, it also had limitations: the substantial loss to follow-up over 11 years caused by nonparticipation or only partial participation, technical problems, health-related exclusions or refusal, and associated with smoking, lower lung function values and higher bronchial reactivity slope, leads us to expect bias. Our sensitivity analyses giving more weight to underrepresented groups within the study sample yielded the same results, though. Effect estimates for age, smoking, BMI increase and atopy also remained stable after exclusion of known asthmatics or adjustment for lung function in different ways. Loss to follow-up is, thus, unlikely to invalidate our findings, but due to the stringent selection processes, their generalisability is limited to relatively healthy participants with no or only mild-to-moderate asthmatic disease, or mild lung function impairment. Thus, our results mostly represent the natural course of bronchial reactivity in a general population sample of healthy adults.
In conclusion, in its natural course, bronchial reactivity slope tends to increase in middle- to old-aged persons after showing a favourable attenuation during young adulthood, a pattern more pronounced in atopic individuals, but less evident in smokers. Airway remodelling, ventilation–perfusion disturbances and airway closure associated with the ageing lung possibly underlie the increase in older age. Females might present a different age-course in airway reactivity due to their smaller lung and airway size or greater susceptibility to environmental exposures.
Acknowledgments
The members of the Swiss Cohort Study on Air Pollution and Lung Diseases in Adults (SAPALDIA) team are as follows. Study directorate: T. Rochat (pneumology; University Hospital, Geneva, Switzerland), U. Ackermann-Liebrich (epidemiology; University of Basel, Basel, Switzerland), J.M. Gaspoz (cardiology; University Hospital, Geneva, Switzerland), N Künzli (epidemiology/exposure; SwissTPH, Basel, Switzerland), L.J.S. Liu (exposure; SwissTPH), N.M. Probst Hensch (epidemiology/genetic and molecular biology; SwissTPH) and C. Schindler (statistics; SwissTPH). Scientific team: J.C. Barthélémy (cardiology; University Hospital, St. Etienne, France), W. Berger (genetic and molecular biology; University of Zürich, Zürich, Switzerland), R. Bettschart (pneumology; Hirslanden Klinik, Aarau, Switzerland), A. Bircher (allergology; University Hospital, Basel, Switzerland), G. Bolognini (pneumology; Regional Hospital, Mendrisio, Switzerland), O. Brändli (pneumology; Höhenklinik, Wald, Switzerland), M. Brutsche (pneumology; Cantonal Hospital, St Gallen, Switzerland), L. Burdet (pneumology; Regional Hospital, Payerne, Switzerland), M. Frey (pneumology; Klinik Barmelweid, Aarau), M.W. Gerbase (pneumology; University Hospital, Geneva, Switzerland), D. Gold (epidemiology/cardiology/pneumology; Harvard School of Public Health, Boston, MA, USA), W. Karrer (pneumology; Luzerner Höhenklinik, Crans Montana, Switzerland), R. Keller (pneumology; Aarau, Switzerland), B. Knöpfli (pneumology; Davos, Switzerland), U Neu (exposure; ProClim, Bern, Switzerland), L. Nicod (pneumology; University Hospital, Lausanne, Switzerland), M. Pons (pneumology; Regional Hospital, Lugano, Switzerland), E. Russi (pneumology; University Hospital, Zürich), P. Schmid-Grendelmeyer (allergology; University Hospital, Zürich), J. Schwartz (epidemiology; Harvard School of Public Health), P. Straehl (exposure; BAFU, Bern, Switzerland), J.M. Tschopp (pneumology; Centre Valaisan de Pneumologie, Crans Montana), A. von Eckardstein (clinical chemistry; University Hospital, Zürich), J.P. Zellweger (pneumology; CHUV, Lausanne) and E. Zemp Stutz (epidemiology; SwissTPH). Scientific team at coordinating centers: P.O. Bridevaux (pneumology; University Hospital, Geneva), I. Curjuric (epidemiology; SwissTPH), J. Dratva (epidemiology; SwissTPH), D. Felber Dietrich (cardiology; SwissTPH), D. Keidel (statistics; SwissTPH), M. Imboden (genetic and molecular biology; SwissTPH), H. Phuleria (exposure; SwissTPH), E. Schaffner (statistics; SwissTPH), G.A. Thun (genetic and molecular biology; SwissTPH), A. Ineichen (exposure; SwissTPH) and M. Ritter (exposure; University of Basel).
The study could not have been done without the help of the study participants, technical and administrative support and the medical teams and field workers at the local study sites.
Local fieldworkers: M. Broglie, M. Bünter and D. Gashi (Aarau); R. Armbruster, T. Damm, U. Egermann, M. Gut, L. Maier, A. Vögelin and L. Walter (Basel); D. Jud and N. Lutz (Davos); M. Ares, M. Bennour, B. Galobardes and E. Namer (Geneva); B. Baumberger, S. Boccia Soldati, E. Gehrig-Van Essen, S. Ronchetto (Lugano); C. Bonvin and C. Burrus (Montana); S. Blanc, A.V. Ebinger, M.L. Fragnière and J. Jordan (Payerne); R. Gimmi, N. Kourkoulos and U. Schafroth (Wald).
Administrative staff: N. Bauer (SwissTPH), D. Baehler, C. Gabriel (both University Hospital, Geneva, Switzerland), R. Nilly and F Meier (both SwissTPH).
Footnotes
This article has supplementary material available from www.erj.ersjournals.com
Earn CME accreditation by answering questions about this article. You will find these at the back of the printed copy of this issue or online at www.erj.ersjournals.com/site/misc/cmeinfo.xhtml
Support Statement
This work was supported by the Swiss National Science Foundation (grant numbers 33CSCO-108796, 3247BO-104283, 3247BO-104288, 3247BO-104284, 3247-065896, 3100-059302, 3200-052720, 3200-042532 and 4026-028099), the Federal Office for Forest, Environment and Landscape, the Federal Office of Public Health, the Federal Office of Roads and Transport, the canton governments of Aargau, Basel-Stadt, Basel-Land, Geneva, Luzern, Ticino and Zurich, the Swiss Lung League, the canton’s Lung League of Basel Stadt/Basel Landschaft, Geneva, Ticino and Zurich.
Statement of Interest
None declared.
- Received November 26, 2009.
- Accepted May 28, 2010.
- ©ERS 2011
REFERENCES










