





Abstract
Identification of work-related allergy, particularly work-related asthma, in a (nationwide) medical surveillance programme among bakery workers requires an effective and efficient strategy.
Bakers at high risk of having work-related allergy were indentified by use of a questionnaire-based prediction model for work-related sensitisation. The questionnaire was applied among 5,325 participating bakers. Sequential diagnostic investigations were performed only in those with an elevated risk. Performance of the model was evaluated in 674 randomly selected bakers who participated in the medical surveillance programme and the validation study. Clinical investigations were evaluated in the first 73 bakers referred at high risk.
Overall 90% of bakers at risk of having asthma could be identified. Individuals at low risk showed 0.3–3.8% work-related respiratory symptoms, medication use or absenteeism. Predicting flour sensitisation by a simple questionnaire and score chart seems more effective at detecting work-related allergy than serology testing followed by clinical investigation in all immunoglobulin E class II-positive individuals.
This prediction based stratification procedure appeared effective in detecting work-related allergy among bakers and can accurately be used for periodic examination, especially in small enterprises where delivery of adequate care is difficult. This approach may contribute to cost reduction.
Exposure to high-molecular-weight flour allergens may result in allergic diseases, such as asthma, allergic rhinitis, conjunctivitis and dermatitis 1, 2. Work-related asthma is the most serious outcome, and accounts for acute morbidity, long-term disability and adverse social and economic impacts 3, 4.
In order to decrease respiratory allergy in bakery workers, the Dutch government, in association with labour and industry organisations, agreed to a covenant in 2001. The main goals of this covenant were dissemination of knowledge among employers and employees concerning reduction of exposure to workplace allergens and health risks, and establishing a health surveillance programme. Studies in the Dutch baking industry, flour mills and baking product industries have shown that exposure is high and needs to be reduced considerably in order to reduce the burden of disease. This cannot be achieved over a short time period without structural changes to the production process, making primary prevention not easily achievable 5.
Besides, a level of no effect for work-related allergy related to flour dust exposure cannot be estimated 6. This implies that even very low exposure levels lead to the development of sensitisation. Therefore, a combination of medical surveillance and exposure reduction in high-risk workers seems to be the most (cost-) effective alternative for intervention. For that reason, a secondary prevention programme was developed that aimed to first identify sensitised workers and then perform sequential medical investigations only in these workers. However, in order to find all sensitised workers, all bakery workers (n = 8,000–10,000) would have to be investigated by skin-prick tests or immunoglobulin (Ig)E serology, which is inefficient and results in high costs, especially as these industries consist of >2,500 traditional bakeries and ∼80 industrial bakeries, flour mills and baking product industries spread all over the country. Of the traditional bakeries, 60% have fewer than five employees, and have poor coverage by occupational healthcare services. Moreover, consultation of a company doctor occurs in only a minority of patients with work-related allergy 7.
Therefore, a questionnaire-based prediction model was developed to estimate the individual probability of the presence of IgE sensitisation to wheat and/or α-amylase allergens. IgE sensitisation to flour allergens was used as an outcome because it is strongly associated with already established allergic (asthmatic) diseases, as well as subclinical illness 8–10. This model enables risk stratification. Clinical evaluation can, therefore, be restricted to workers with an elevated sensitisation risk, leaving a considerable number of workers at low risk, in whom no or less-far-reaching medical investigations are required 11, 12.
The present article describes the results of the application of a prediction model among 5,325 workers exposed to flour dust (from baking, milling and bakery ingredient industries). Performance of the model was evaluated in 674 traditional and industrial bakers who participated in both the health surveillance programme and a validation study among 890 randomly selected bakers. Results of clinical investigations in the first 73 referred bakers at high risk are reported.
METHODS
The prediction model
The individual probability of sensitisation to wheat and/or fungal α-amylase allergens (IgE class II) was estimated using a questionnaire-based prediction model. This model had been developed previously using data from a survey among 390 Dutch bakers 13. For practical application, the model was transformed into a score chart to calculate sum scores:

Each predictor was valued as 1 when present and 0 when absent. Risk groups were calculated using the following cut-off points: 0–1: low score; 1.5–3.0: intermediate score; and ≥3.5: high score. The model development and score chart are described more extensively in the online supplementary material.
Risk stratification
A short questionnaire with 19 questions, containing the four predictors, was distributed to the bakery workers by instructed consultants who visited all of the companies. The workers were asked to complete the questionnaire and return it by regular mail. On the basis of their response, each worker was classified as being of low, intermediate or high risk of being sensitised to wheat and/or fungal α-amylase (fig. 1).

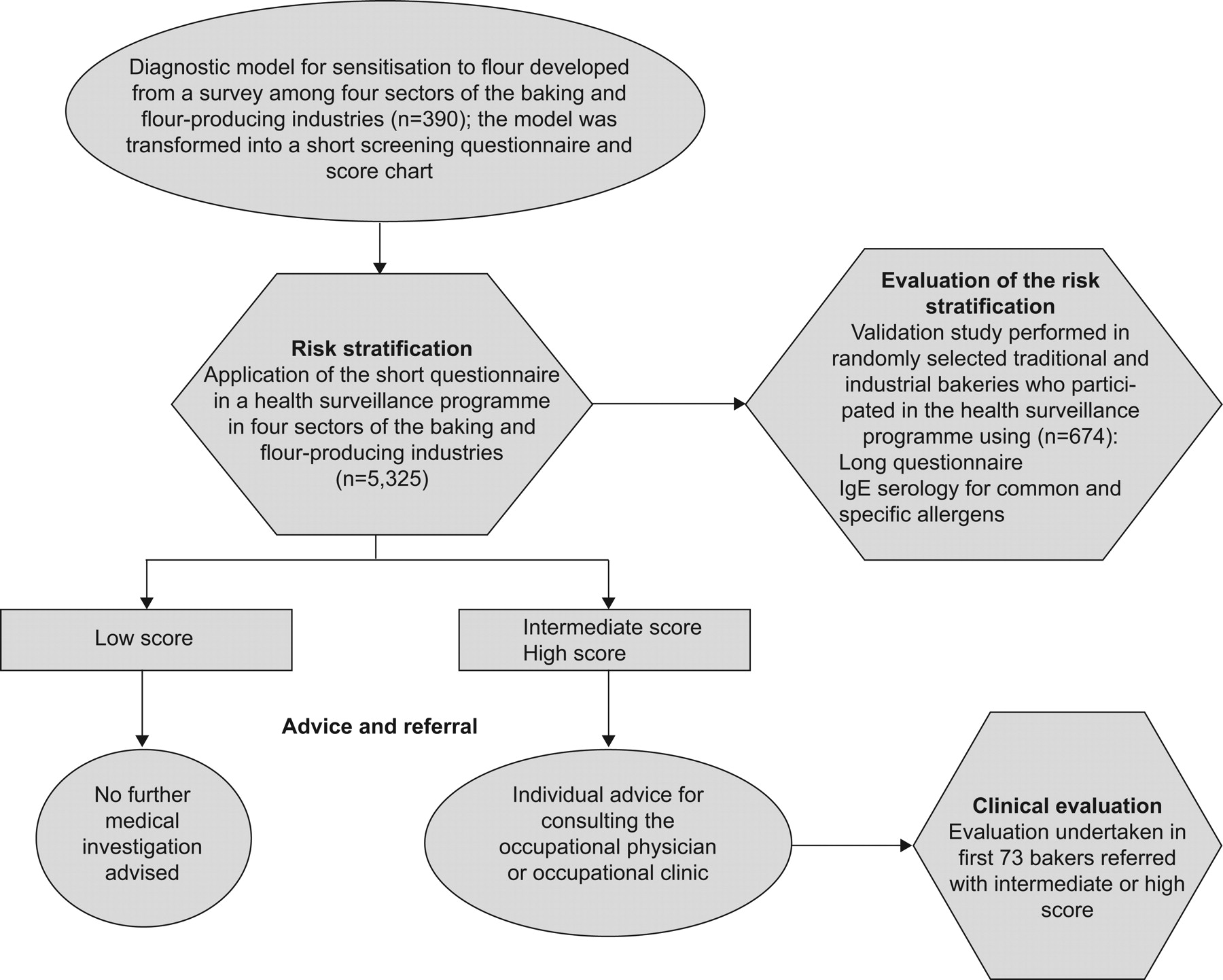{kind=link}
Design and participation in the health surveillance programme and evaluation of the risk stratification in the validation study. IgE: immunoglobulin E.
Advice and referral
The results of the scores were communicated by letter to every worker individually and to the occupational physician. Workers with a low sum score were informed about a low sensitisation risk and that no action was indicated. Workers with intermediate scores were invited for diagnostic work-up by their occupational physician. Workers with a high sum score were directly referred to the specialised clinic for occupational respiratory diseases.
Evaluation of the risk stratification
The accuracy and impact of the risk stratification were evaluated in data from randomly selected traditional and industrial bakeries. This so-called validation study was based on a random sample of 674 exposed bakers who participated in the health surveillance programme 14.
Clinical evaluation
Results of advanced medical investigations were described in the first 73 referred bakers. All of the bakers visiting the clinic underwent clinical history-taking, physical examination, serology tests, spirometry and measurement of nonspecific bronchial hyperresponsiveness to histamine. Peak expiratory flow (PEF) and nonspecific bronchial hyperresponsiveness were measured after a continuous period of ≥2 weeks both at and off work. Workers with an established diagnosis were referred back to their occupational physician.
Statistical analyses
All statistical analyses were performed using SPSS 15.0 for Windows (Statistical Product and Service Solutions, Inc, Chicago, IL, USA). Prevalence rates were compared using the Chi-squared test. Differences between means were compared using ANOVA. Discrimination was assessed by calculating the area under the receiver operating characteristic curve. The diagnostic model was developed using methods described by Harrell et al. 15. Statistical significance was defined as a p-value of <0.05 (two-tailed).
RESULTS
Between November 2004 and November 2006, 6,714 workers from 1,637 traditional bakeries and 1,760 workers from 74 industrial bakeries were registered for participation in the programme (table 1). They covered almost all of the industrial and half of the traditional enterprises throughout the Netherlands. Of 1,637 registered traditional bakeries, 1,189 (72.7%) participated in the programme, whereas all of the registered industrial bakeries participated. A short questionnaire, specifically developed for the present purpose, was handed out to 8,396 bakery workers and received back from 5,325 (63.4%). A total of 60% of workers in the traditional and 80% of workers in the industrial bakeries sent back the short questionnaire. In the flour milling (n = 10) and baking products companies (n = 13), almost 60% of workers joined the programme. The highest rate (60%) of workers with low scores was found in traditional bakers, and the highest rate (21%) of high scores in industrial bakers participating in the programme (table 2). A small nonparticipation study among 86 bakers showed that two-thirds of them either did not receive the questionnaire or forgot to send it back to the institute. The proportion of workers worried that the results could be used in an unfavourable way by their employer was 3%.
Table 3 outlines the predicted and observed sensitisation rates across different scores in workers participating in the validation study. The predicted mean probability of sensitisation to wheat and/or fungal α-amylase in these workers was lower (18.7%) than the observed sensitisation rate (20.1%). The predicted sensitisation rate to wheat and/or fungal α-amylase in the high-score group was somewhat higher (42.7%) than the observed rate (41.5%), and lower in the low-score group (9.3 compared to 12.9%). Wheat sensitisation was 5.9 times higher (46 out of 135; 34.1%) in workers with high scores compared to those with low scores, and showed 16.3% (22 out of 135) α-amylase sensitization (2.0 times higher than individuals with low scores). Workers sensitised to wheat allergens reported 75.3% (64 out of 85) intermediate and high scores, leaving 24.7% (21 out of 85) reporting low scores. Table 4 shows the distribution of asthma-related symptoms, work-related symptoms, absenteeism and inhalation medication across different scores. Workers with low scores were significantly older (mean 41.6 yrs) than workers with intermediate and high scores. On average, they had also worked longer (16.3 yrs) in their current job than bakers with intermediate and high scores. Approximately 70% of workers reporting asthma attacks in the last 12 months and ∼60% reporting inhalation medication (corticosteroids plus long-acting β2-mimetics or short acting β2-mimetics) had high scores. Only 9.1% of bakers reporting wheezing had low scores. No low scores were identified in workers reporting asthma attacks during or following work, a finding understandably attributed to the fact that one of the questions was a predictor of the diagnostic rule.
Bakers with work-related eye or nasal symptoms showed high scores in 69 or 61%, respectively, leaving only 5 or 10%, respectively, of these symptoms in the low-score group. Absenteeism was only detected in high- and intermediate-score bakers. A change in job or task due to work-related allergy had occurred in seven of the eight cases found in bakers with high scores. Results in the low-score group (low predicted probability of IgE sensitisation to flour allergens) were analysed in order to evaluate the extent of misclassification of flour sensitisation and the impact on detection of respiratory allergy. Table 5 shows the distribution of wheezing symptoms, work-related eye and nasal symptoms, and medication use for bronchial asthma across sensitisation to flour allergens in workers with low scores. In the low-score group 12.9% (47 out of 365) bakers were sensitised to wheat and/or α-amylase allergens. Of these 47 bakers, 29 (61.7%) were sensitised to α-amylase and 21 (44.1%) to wheat. Only six (1.6%) bakers with low scores used inhalation medication (corticosteroids plus long acting β2-mimetics and/or short acting β2-mimetics). Symptoms reported during daily work, and which improved if not working, including wheeze, conjunctivitis or rhinitis, were not reported in sensitised bakers with low scores.
Clinical evaluation was completed in the first 73 (69 traditional and four industrial bakers) referred individuals (table 6). Bakers with high scores, as calculated from the screening questionnaire, were advised to contact the clinic directly. Bakers with intermediate scores were first evaluated by their occupational physician and referred to the clinic if necessary. Two bakers with low scores visited the clinic on their own initiative. Of 73, 39.7% were wheat- and 9.6% α-amylase-sensitised. Rye serology was only assessed in workers reporting symptoms related to rye exposure (n = 14). Eight out of 14 (57.1%) bakers were sensitised. Of these eight workers, 75% (six) were also sensitised to wheat allergens. Rhinitis and conjunctivitis, either alone or in combination, were diagnosed in 69.9% (51 out of 73) of the individuals, of whom 58.8% (30 out of 51) reported their rhinitis to be associated with their work. Bronchial asthma (general and work-related) was diagnosed in 25 (34.3%) bakers attending the clinic, 10 (13.7%) bakers had occupational asthma and three (4.1%) cases could be assigned as having work-exacerbated asthma. Most (80%) of the asthma cases were detected in the high-score group. The prevalence of work-related rhinoconjunctivitis in bakers with work-related asthma was 83% (10 out of 12), and 31% (four out of 13) in bakers with asthma diagnosed as not work-related (data not shown). In eight (11%) bakers, no clinical disease could be diagnosed. Five of them presented themselves with an intermediate score, whereas none of them were sensitised to specific, as well as common, allergens. In three bakers, chronic obstructive pulmonary disease (COPD), hypertension and hyperventilation were diagnosed.
DISCUSSION
Prediction models for various outcomes have been developed for clinical diagnosis in a comprehensive and scientific way since the late 1980s. The essence of diagnosis concerns the level of probability with which the outcome (illness) is known to be present or absent in a particular person at a particular time 16, 17. The development of diagnostic prevalence/probability functions for a given outcome, in a given domain, makes it possible to find a small number of predictors to constitute the best possible knowledge base for diagnosis. However, few prediction models have been developed for occupational respiratory medicine purposes or found an application in surveillance programmes 18–20. This is surprising since, with the use of prediction models, risk groups may be identified easily in occupational health practice or medical surveillance programmes specifically aimed at secondary prevention. The present study demonstrates that, with a simple short questionnaire, developed to predict flour sensitisation, work-related allergy can accurately be identified.
In this medical surveillance programme among all eligible bakers in the Netherlands, a diagnostic rule was applied to predict the presence of wheat and/or fungal α-amylase sensitisation. Bakers were stratified into risk groups in order to inform them about the probability of having an allergic disease and to assist in clinical referral. Risk stratification resulted in a high-score group for clinical investigation, an intermediate-score group for medical follow-up by occupational physicians and a low-score group comprising ∼57% of the workforce, in which medical investigations were supposed not to be indicated. Allergic diseases were diagnosed more specifically in an outpatient clinic specialising in occupational respiratory disorders.
Given the large number of bakeries distributed throughout the Netherlands, the questionnaire was presented to the individual baker by trained consultants (contacted by the Dutch Grains Seeds and Pulses Product Board (The Hague)) visiting the bakery. Using this approach, a rather satisfactory overall response rate of ∼63% was attained, with the highest rate (79%) in industrial bakers. This is comparable to other sector-wide surveillance programmes, which, for instance, exist in the construction industry (personal communication). Surprisingly, only 3% of the nonresponding bakers were worried that the results could be used in an unfavourable way by their employer.
In general, most prediction models show reduced accuracy when applied in new populations 12. This so-called external validation of the present model was not assessed. However, the model was validated internally. Differences in sensitisation rate may still be expected for the total population (predicted 18.7 versus observed 20.1%), as well across different scores (table 3). Furthermore, the present study also showed that the model discriminated wheat sensitisation more accurately than sensitisation to α-amylase allergens. In bakers with a high score, 34.1% wheat sensitisation was found compared to 16.3% α-amylase.
Stratification and misclassification
The choice of cut-off points for classification of workers into the high-, intermediate- or low-risk (probability) groups is crucial and determines referral policy and misclassification rate. A balance must be sought between an acceptable proportion of missed cases and unnecessary referrals. Although the model used was developed with the best available knowledge, derived from a well-designed appropriate study, failures and difficulties can be expected for various reasons. It might be wondered whether or not it is acceptable to miss 35.6% (47 out of 132) flour-sensitised individuals at the gain of minimising the number of individuals (56%) to be evaluated by occupational physicians and clinical pulmonologists.
Misclassification of workers wrongly assigned as sensitised into the high-score group is less dramatic because they present with respiratory health complaints that need to be evaluated further, as presented in the clinical evaluation. However, on the basis of the present validation sample, we estimated that 12.9% of the workers with a low calculated sensitisation probability were wrongly assigned as nonsensitised to flour allergens. This is a serious problem because no further medical investigation was advised. These workers may be asymptomatic, or deny symptoms due to poor perception. When bakers were reinvestigated as part of the present validation study, the low-score group showed very low prevalences of reported wheezing (2.7%), work-related wheezing (0.3%), work-related conjunctivitis (1.0%) and work-related rhinitis (3.8%). Although asthma attacks were not reported in the low-score group, the nondetection of current asthmatics is a serious problem, especially in sensitised workers. However, six (1.6%) bakers treated with inhalation medication (corticosteroids plus long-acting β2-mimetics and/or short-acting β2-mimetics), which may indicate respiratory problems, were found in the low-score group. Three of them were sensitised to flour allergens. None of the sensitised bakers reported work-related asthma attacks, work-related wheezing or work-related upper respiratory symptoms. Therefore, it seems rational to conclude that they belong to a group of sensitised workers, with their respiratory disorder (asthma or COPD) well treated (no respiratory symptoms) and/or their exposures optimally controlled. If these findings are extrapolated to all of the investigated traditional and industrial bakers, 0.9% (1.6%×55.2%) individuals with possible bronchial asthma or COPD are not detected because of having low scores, comprising 41 (0.9×4,612) individuals.
Ideally, it would be desirable to have information about the clinical evaluation of bakers with a low score, which would give more accurate evidence regarding the existence of occupational allergic diseases, such as work-related asthma etc. However, the present approach of analysing the responses of 365 bakers with low scores provides sufficient indication that the number of false negatives is acceptable. Only six (1.6%) bakers were found to be using some kind of inhalation medication that could be attributed to having asthma or COPD (or no disease), and not a single worker indicated having (work-related) asthma. We, therefore, think that the prediction model used to evaluate occupational allergic diseases in the low-score group showed accurate discrimination. Besides, a clinical investigation of workers already informed to have a low probability and advised that no medical investigations were needed, would undoubtedly lead to substantially biased results. We, therefore, think that our approach of calculating the expected prevalence of a proxy for asthma/COPD (use of inhalation medication) provides an acceptable and sufficiently accurate result given the size of the group of bakers.
The alternative to not missing sensitised workers is to investigate all bakers (n = 4,612) using serological tests and refer only workers with positive IgE class II results for clinical evaluation. This approach would not only lead to high costs but also result in undetected symptomatic bakers nonsensitised to flour allergens. Again, if cases reporting inhalation medication for their asthma were scrutinised, 5.5% (28 out of 508) symptomatic bakers not sensitised to wheat and/or α-amylase allergens would be missed and excluded from advanced medical follow-up (data not shown). Thus opting for the alternative and investigating all bakers serologically would lead to a 6-fold (5.5 versus 0.9%) higher number of nondetected possible asthma cases compared to the present method using a prediction model for flour sensitisation.
Clinical evaluation
Among the 73 referred bakers with intermediate and high scores, a third had bronchial asthma. Of these asthmatics, 80% reported high scores. Occupational asthma was diagnosed in 10 (40%) cases and work-exacerbated asthma in three (12%), leaving 12 cases diagnosed as having general asthma (for definitions, see online supplementary material). Three general asthma cases were sensitised to wheat allergens. All three bakers reported work-related upper respiratory symptoms and use of respiratory medication. However, they were regarded as having general asthma as diagnostic tests (e.g. positive serial PEFs or significant improvements in histamine response (at the end of a working period compared with a period away from work)) could not be assessed appropriately. Nine general asthma cases were not sensitised to any of the workplace allergens (wheat, α-amylase, soya or rye). Unfortunately, serial PEFs and work-related histamine response could not be assessed in all of them because of constraints put in place by the employer. Thus it seems plausible that some cases may be more correctly classified as occupational asthma or work-exacerbated asthma and not as general asthma. These results point towards the well-known difficulties in establishing a proper diagnosis of asthma in the workplace. Especially occupational asthma and work-exacerbated asthma, where an improvement in symptoms during times away from work and worsening on days with regular exposures, must be objectively assessed.
Work-related asthma may be accompanied or preceded by symptoms of rhinitis or conjunctivitis. These symptoms were shown to be present in 70% of these asthmatics. A clear association with their work could be established in ∼40%. In bakers with occupational asthma or work-exacerbated asthma, work-related rhinitis and/or conjunctivitis were reported in the majority (85%) of cases, whereas, in general asthma, these symptoms were found in 25% of patients. Besides, ∼50% (14 out of 30) patients with work-related rhinitis and/or conjunctivitis were found to have coexisting asthma. These findings stress the importance of work-related rhinitis and/or conjunctivitis associated with work-related asthma, which are, however, difficult to test objectively.
The present surveillance programme and its evaluation demonstrate that, by applying a simple questionnaire model to predict the probability of flour sensitisation, work-related allergy can accurately be detected in bakers with an elevated risk. Of bakery workers with asthma, 90% could effectively be identified in this way. The model discriminated wheat sensitisation more accurately than sensitisation to α-amylase allergens. Workers with a low sensitisation probability showed very low rates (0.3–3.8%) of work-related respiratory symptoms or other indicators of disease (medication use or absenteeism). Prediction of flour sensitisation by means of a simple questionnaire and a score chart is probably more effective at detecting work-related allergy than serology testing followed-up by clinical investigation in all IgE class II-positive individuals. Therefore, this model can fairly and straightforwardly be incorporated into the already existing and statutorily regulated periodic occupational health examinations among bakery workers, especially in small enterprises, where delivery of adequate care is difficult. This approach is expected to contribute to cost reductions.
Footnotes
This article has supplementary material accessible from www.erj.ersjournals.com
Support Statement
This study was supported by the Netherlands Ministry of Social Affairs and Employment (The Hague), the Dutch Grains Seeds and Pulses Product Board (The Hague) and the Aladdin programme for occupational health research (the Netherlands Ministry of Social Affairs and Employment).
Statement of Interest
None declared.
- Received October 29, 2009.
- Accepted January 31, 2010.
- ©2010 ERS










