





Abstract
We sought to determine the type of pulmonary involvement in microscopic polyangiitis (MPA), primarily focusing on pulmonary fibrosis (PF), its prevalence, temporal relationship with other disease manifestations and outcome.
33 patients (16 males) with biopsy proven perinuclear anti-neutrophilic cytoplasmic antibody-positive MPA (age 63.5 yrs) participated in the study. Pulmonary involvement was assessed using standard methods, including radiographic imaging (chest radiographs and high-resolution computed tomography), pulmonary function testing, bronchoscopy and bronchoalveolar lavage, and, if indicated, lung biopsy. All-cause mortality was analysed by the Kaplan–Meier method and was compared between MPA patients with and without PF.
At the time of diagnosis, renal involvement was detected in all patients, with renal biopsies being consistent with segmental necrotising glomerulonephritis in all patients. The most common respiratory symptom was haemoptysis, which was found in nine (27%) patients. PF was present in 12 (36%) patients at the time of diagnosis, whereas one patient developed PF while on therapy ∼10 yrs after disease diagnosis. In seven patients with PF, respiratory symptoms related to fibrosis preceded other disease manifestations by a median (range) period of 13 (5–120) months. Patients were followed up for a period of 38±30 months. Presence of PF was associated with increased mortality (p = 0.02), with six deaths occurring in the fibrotic group and one in the nonfibrotic group. In the fibrotic group most deaths were related to PF.
PF occurs frequently in MPA, may precede other disease manifestations by a variable length of time and has a poor prognosis.
Microscopic polyangiitis (MPA) is a systemic necrotising vasculitis characterised by the involvement of small blood vessels, the absence of granulomas on histopathological specimen and, usually, no detection of immune deposits.
While the kidney is the most commonly involved organ in MPA, lung involvement may also occur in a significant percentage of patients, ranging from 25% to 30% 1–3. Diffuse alveolar haemorrhage secondary to pulmonary capillaritis is the most frequent manifestation of respiratory involvement, expressed clinically as haemoptysis, dyspnoea and anaemia 2, 3. Recently, case reports or small patient series 4–15 have also described pulmonary fibrosis in MPA and raised the question that pulmonary fibrosis may also be an important clinical manifestation of the disease. However, the precise prevalence of pulmonary fibrosis and its impact on patient survival remain largely unknown.
Therefore, the purpose of our study was to report the clinical characteristics, prevalence and outcome of pulmonary fibrosis in consecutive MPA patients followed up for several years.
METHODS
This study included newly diagnosed MPA patients or MPA patients who were followed up in the outpatient clinics at two tertiary hospitals in Athens, Greece (Laiko University Hospital and General Sismanogleio Hospital), during the period from November 1, 2003 to December 31, 2008. Study approval was obtained by the Institutional Review Board (Laiko University Hospital) which waived the need for informed consent. Inclusion criteria for entry into the study were: 1) presence of rapidly progressive glomerulonephritis and/or alveolar haemorrhage in combination with other systemic manifestations of vasculitis; 2) histological evidence of small vessel vasculitis or pauci immune necrotising glomerulonephritis; and 3) absence of granulomatous inflammation or asthma 16, 17. In our study, alveolar haemorrhage was defined as the presence of pulmonary infiltrates in conjunction with a bloody bronchoalveolar lavage (BAL) or increased percentage of haemosiderin-laden macrophages and the absence of infection or pulmonary oedema 18. Patients with isolated small vessel vasculitis and absence of systemic involvement were not included in the study. Particular attention was paid to excluding patients with Wegener's granulomatosis, malignancy or connective tissue disease associated vasculitides or Churg–Straus syndrome. Thus, patients with evidence of ear, nose, or throat involvement, as well as patients with asthma, lung nodules, cryoglobulinemia, or presence of immunoglobulin A deposits in skin or other biopsy specimen were not included 2.
At the time of diagnosis, pulmonary involvement was assessed with imaging studies (plain chest radiographs and thoracic computed tomography (CT)). Bronchoscopy with BAL was performed for diagnostic purposes when pulmonary involvement was the only or major manifestation of MPA. Patients with pulmonary manifestations at the time of diagnosis were followed up with repeat studies (pulmonary function testing, lung CT) if indicated. Presence of anti-neutrophilic cytoplasmic antibody (ANCA) was tested in all patients using an indirect immunofluorescence assay. Pulmonary function testing was measured following initial therapy and within 6 months from disease diagnosis, when patients were clinically stable. Measurements were made according to standard methods and included spirometry, lung volumes and diffusion capacity of the lung for carbon monoxide.
Radiological assessment
High-resolution CTs (HRCTs) were obtained using various scanners. An experienced CT radiologist who was blinded to the clinical data reviewed the CT scans. Pulmonary fibrosis was defined as the presence of reticular pattern, intralobular lines, traction bronchiectasis or honeycombing which persisted on repeat CT examination. The degree of fibrosis was assessed semiquantitatively by recording as involving <10%, 10–40% or >40% of the lung parenchyma 19. The CTs were also assessed for the presence of additional radiological abnormalities, such as ground-glass opacities, consolidation or pleural thickening.
Analysis
Data are presented as mean±sd, unless otherwise stated. The differences between groups were analysed with an unpaired t-test or Fischer's exact test where applicable. Kaplan–Meier analysis was used to study differences in survival between MPA patients with and without pulmonary fibrosis. All statistical analyses were carried out with commercially available statistical software (MedCalc Software, Mariakerke, Belgium).
RESULTS
33 patients with a diagnosis of MPA met our criteria and were included in the study. 26 of these patients were newly diagnosed whereas seven patients had been diagnosed with MPA prior to the study period and were followed up in the outpatient clinic. In these seven patients, data related to disease presentation and pulmonary involvements were retrieved from their records. All patients were followed up for a period of 38±30 months.
On the basis of the presence of pulmonary fibrosis, patients were divided into two subgroups: fibrotic and non-fibrotic. Table 1 shows the clinical characteristics for the two subgroups. Constitutional symptoms such as fever, fatigue or weight loss were present in the majority of patients (table 1). The most common respiratory symptom was haemoptysis, which was reported in five out of the 13 patients with pulmonary fibrosis and in four out of the 20 patients without fibrosis. Dyspnoea and chronic cough were present in four and three patients with pulmonary fibrosis, respectively. ANCA was present in 32 (97%) out of 33 patients: 31 patients had a perinuclear staining pattern (p-ANCA) and one patient had a mixed p-ANCA and cytoplasmic-ANCA. ANCA specificity with ELISA was tested in seven patients, all of whom showed myeloperoxidase (MPO) type of antibodies. Routine testing for anti-MPO was not performed as the diagnosis of MPA was based on histological evidence of pauci-immune glomerulonephritis or small vessel vasculitis.
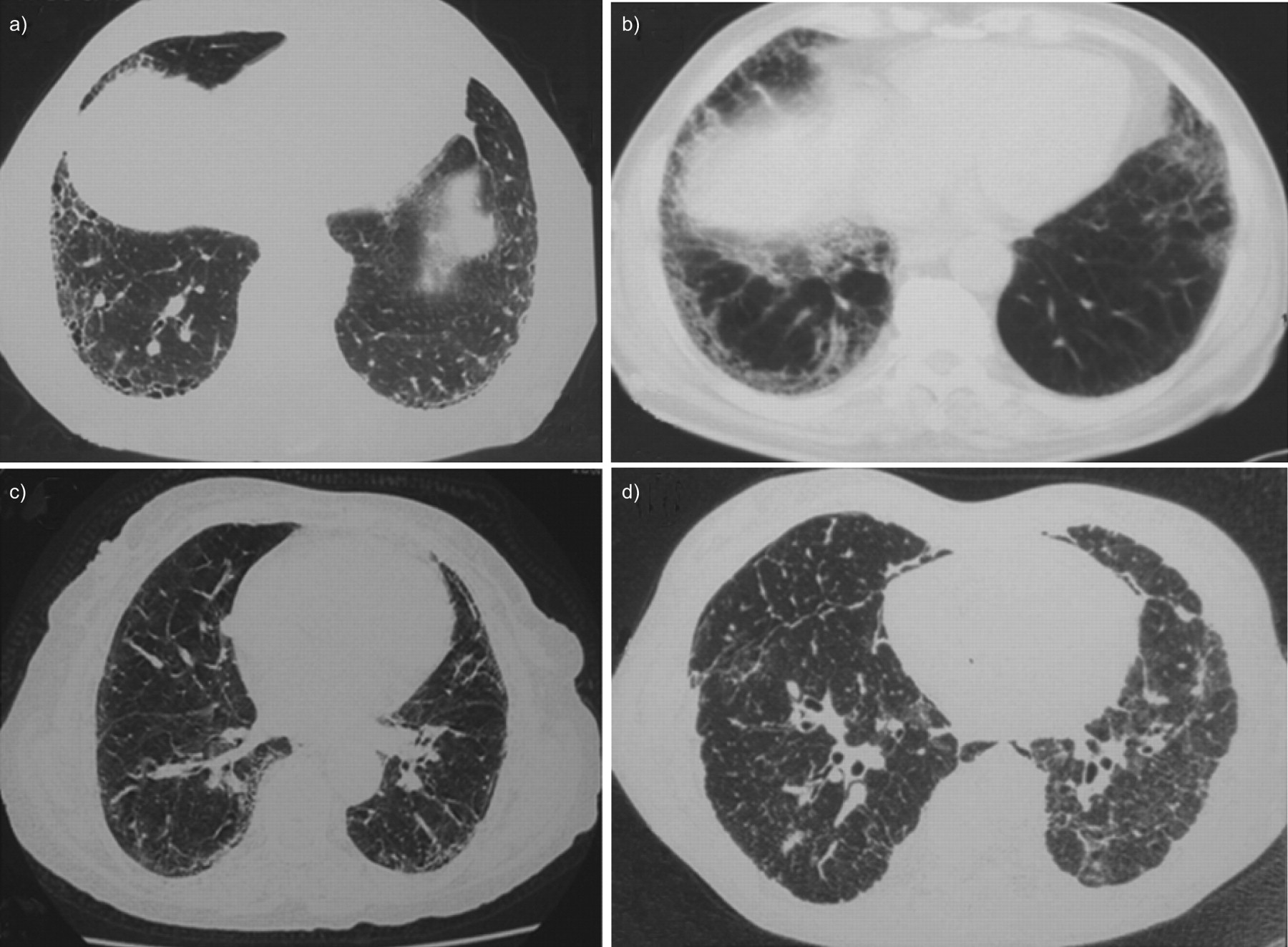
HRCT images were available in 32 patients at the time of MPA diagnosis. One patient with no respiratory symptoms and a normal chest radiograph did not undergo a HRCT. The differences in the HRCT findings between the fibrotic and non-fibrotic subgroups are shown in table 1. Semiquantitative assessment of the extent of fibrosis at time of diagnosis showed that eight patients had >40% of lung involvement, four patients 10–40% of lung involvement, and one patient <10% of lung involvement. Representative HRCT images of patients with pulmonary fibrosis are shown in figure 1. Pulmonary fibrosis was present in 12 (36%) patients at time of diagnosis. An additional patient developed pulmonary fibrosis while on therapy, ∼10 yrs after disease diagnosis. Four patients with pulmonary fibrosis also had haemoptysis at the time of MPA diagnosis. In seven patients with pulmonary fibrosis, the fibrosis preceded other disease manifestations by a median (range) period of 13 (5–120) months. In one patient who underwent open lung biopsy the histological type of fibrosis was usual interstitial pneumonia (UIP). In the patients with pulmonary fibrosis, the radiological HRCT pattern of fibrosis was consistent with UIP in seven patients, and with nonspecific interstitial pneumonia pattern in four patients. On repeat HRCTs, pulmonary fibrosis progressed in five patients and remained unchanged in the remaining eight patients. Pulmonary function data for the patients with and without pulmonary fibrosis are shown in table 2. The total lung capacity was significantly lower in patients with pulmonary fibrosis than in those without fibrosis (p<0.05).

Representative high-resolution computed tomography in four patients with microscopic polyangiitis (MPA) and pulmonary fibrosis. a–c) Pulmonary fibrosis preceded other manifestations of MPA, whereas in d) fibrosis developed several years after diagnosis of MPA.
During the follow-up period, there were six all-cause deaths in the fibrotic group and one death in the non-fibrotic group. Survival analysis using the Kaplan–Meier method showed a significantly greater all-cause mortality among MPA patients with pulmonary fibrosis (p = 0.02). The median survival of MPA patients with pulmonary fibrosis was 72 months; the median survival of MPA patients without fibrosis could not be calculated as > 85% of patients were still alive at the last follow-up (December 31, 2008) (fig. 2). Of the six deaths in the fibrotic group, four were directly related to fibrosis (all with extensive fibrosis involving >40% of parenchyma at the time of diagnosis) and respiratory failure, one death was due to lung cancer and one was due to sepsis. In the non-fibrotic group, the single death was due to small cell lung cancer in a patient with history of smoking and chronic obstructive lung disease. At the last follow-up (December 2008), two additional patients in the fibrotic group were on home oxygen for end-stage respiratory failure.

{kind=link}
{kind=link}
Kaplan–Meier survival graph comparing microscopic polyangiitis patients with (––––) and without (- - - -) pulmonary fibrosis.
DISCUSSION
Our study demonstrates that pulmonary fibrosis is a frequent manifestation and a significant cause of death in patients with MPA. Pulmonary fibrosis may predate other manifestations of MPA by a variable period of time or may manifest at time of disease diagnosis.
Our study included a homogenous population of MPA patients who all had histological evidence of pauci-immune glomerulonephritis on renal biopsy. We excluded patients who had cavitary lung lesions at the time of diagnosis or history suggestive of upper airway symptoms that could be due to Wegener's granulomatosis, or patients with Churg–Straus syndrome according to the American College of Rheumatology diagnostic criteria 20, 21.
We found a relatively high prevalence of pulmonary fibrosis in patients with MPA. Symptomatic pulmonary fibrosis preceded other clinical manifestations of MPA in seven (21%) patients in our cohort whereas in an additional five (15%) patients there was radiographic evidence of pulmonary fibrosis at the time of diagnosis. Overall, evidence of fibrosis by HRCT at the time of disease diagnosis was more common than haemoptysis (36% versus 27%) in our patient cohort. In two patients, pulmonary fibrosis predated other MPA manifestations by ∼10 yrs. An equally long interval was also reported in previous reports 8, 9, 11. Foulon et al. 9 described six MPA patients in whom pulmonary fibrosis predated other features of MPA by a mean time of 36.2±50 months (range 2–137 months).
In our study, clinically overt pulmonary fibrosis was essentially restricted to those patients in whom fibrosis preceded other disease manifestations. As in previous reports, these patients were frequently diagnosed as having idiopathic pulmonary fibrosis and were treated as such. There was only one patient who developed fibrosis and subsequently died, ∼10 yrs after disease diagnosis. In five patients with only radiological evidence of fibrosis but no symptoms at the time of diagnosis, the fibrosis essentially remained asymptomatic for a period of several years. It is very likely that in this particular subset of patients with asymptomatic pulmonary fibrosis their disease would have gone undetected if detailed pulmonary assessment with CT was not performed. The exact percentage of MPA patients with only radiographic evidence of pulmonary fibrosis at the time of MPA diagnosis that will develop respiratory failure requires further study.
The pathogenesis of pulmonary fibrosis in MPA remains poorly understood. Recurrent occult alveolar haemorrhage has been suggested as a putative mechanism leading to fibrosis, in a manner similar to that described for pulmonary fibrosis in patients with idiopathic haemosiderosis and haemoptysis 6, 22. Subclinical alveolar haemorrhage is frequently detected in patients with ANCA-associated vasculitides and pulmonary disease 23. Alternatively, fibrosis may be related to a direct fibrogenicity of ANCA antibodies and, in particular, to MPO-ANCA antibodies. Although early histopathological studies 24 did not detect marked differences in the degree of lung fibrosis among the various types of vasculitides, studies have suggested that MPO antibodies may cause generalised pulmonary tissue injury through the release of products of activated neutrophils 25. In this setting, fibrosis could represent a reparative response to the underlying chronic lung injury 6, 25.
To the extent that pulmonary fibrosis was clinically manifest at the time of diagnosis in the majority of patients in this study and in previous studies 8, 9, 12, the possibility of idiopathic pulmonary fibrosis inducing MPA cannot be entirely excluded. In a recent retrospective study on 17 patients with idiopathic pulmonary fibrosis and positive ANCA testing, Foulon et al. 9 reported that 40% of these patients developed MPA after a variable period of time ranging from 0 months to 137 months. Considering the short survival of patients with idiopathic pulmonary fibrosis, this figure is relatively high. Ultimately, the cause and effect relationship between pulmonary fibrosis and MPA will require larger prospective studies of patients with both pulmonary fibrosis and MPA.
The limitations of our study should be acknowledged. A limitation of our study was the lack of lung biopsies to fully characterise the histological features of fibrosis in this disease. Lung biopsy is not usually indicated in patients with MPA when specific diagnosis can be established reliably by other organ biopsies and serum assay for ANCA 26. Furthermore, in patients presenting with pulmonary fibrosis, the diagnosis of interstitial fibrosis can also be reliably made on the basis of the characteristic CT findings, such as peripheral honeycombing and traction bronchiectasis 27. All patients were screened for other diseases causing pulmonary fibrosis including collagen vascular diseases or occupational exposure, drugs or family history 28. Finally, the prevalence of pulmonary fibrosis found in our study may not accurately reflect the true prevalence of fibrosis in these patients due to selection bias. Our patient cohort consisted of patients who were treated primarily in a general medicine or renal disease ward and may not be representative of the entire MPA patient population. Larger studies including patients with various manifestations will be required to assess the precise prevalence of fibrosis in these patients.
A practical corollary of our findings applies to the diagnostic approach of patients presenting with pulmonary fibrosis. In these patients, screening for an occult MPA is not typically recommended 29. The high prevalence of fibrosis in MPA in our study and other data suggest that these patients should be screened with ANCA to test for the possibility of MPA.
In summary, we have demonstrated a relatively high prevalence of lung fibrosis in patients with MPA. The fibrosis may precede other disease manifestations by a variable length of time or become manifest at time of diagnosis. This subset of MPA patients has an extremely poor prognosis.
Footnotes
Statement of Interest
None declared.
- Received July 14, 2009.
- Accepted October 28, 2009.
- ©ERS 2010
REFERENCES










