





Abstract
The effect of long-term inhaled corticosteroid (ICS) use on myocardial infarction (MI) and cardiovascular (CV) death in chronic obstructive pulmonary disease (COPD) remains uncertain.
We conducted a systematic search of MEDLINE, EMBASE, ISI, regulatory documents and manufacturers' trial registries for long-term (>24 weeks duration) randomised controlled trials (RCTs) or controlled observational studies reporting on CV outcomes or death with ICS use in COPD. A fixed effects model was used to calculate the relative risks (RRs) and 95% CIs.
23 RCTs with 24–160 weeks of follow-up were included. In the RCTs, ICS were not associated with a significantly reduced risk of MI (RR 0.95, 95% CI 0.73–1.23; p = 0.68, I2 = 0%), CV death (RR 1.02; 95% CI 0.81–1.27; p = 0.89, I2 = 0%), or mortality (RR 0.96, 95% CI 0.86–1.07; p = 0.43, I2 = 0%). In the observational studies, ICS use was associated with a significant reduction in CV death (two studies: RR 0.79, 95% CI 0.72–0, 86; p <0.0001, I2 = 44%) and mortality (11 studies: RR 0.78, 95% CI 0.75–0.80; p<0.001, I2 = 33%). Publication bias via funnel plot asymmetry was noted for mortality in the observational studies (Egger test, p = 0.05).
We conclude that while observational studies suggest that ICS may potentially confer CV or mortality benefit, RCTs failed to show any significant effect of ICS therapy on MI or CV death. These conflicting findings need to be clarified through further research.
- Cardiovascular effects
- chronic obstructive pulmonary disease
- inhaled corticosteroids
- meta-analysis
- mortality
Inhaled corticosteroids (ICS) such as fluticasone propionate, budesonide and beclometasone are widely used in chronic obstructive pulmonary disease (COPD) 1. According to the current Global Initiative for Chronic Obstructive Lung Disease guidelines, ICS are indicated in combination with long acting β2-agonists (LABA) in patients with moderate-to-severe COPD to reduce the frequency of exacerbations 2.
ICS may potentially reduce cardiovascular (CV) events by alleviating the systemic inflammation responsible for atherogenesis in patients with COPD 3. CV and mortality benefits with ICS have been reported in observational studies in patients with COPD 4, 5. However, it remains uncertain whether this beneficial effect is seen in randomised controlled trials (RCTs). CV disease is an important cause of morbidity and mortality among patients with COPD 6. The strength of association between ICS use and CV events and mortality and the magnitude of any potential benefit needs critical evaluation.
Our primary objective was to systematically ascertain the risk of myocardial infarction (MI) or CV death associated with long-term use of ICS compared with control therapies in COPD. As a secondary objective, we aimed to ascertain the effects of ICS on overall mortality.
METHODS
Inclusion criteria
Our inclusion criteria for RCTs were as follws: 1) a study design consisting of parallel-group RCTs for any ICS (fluticasone, beclomethasone, budenoside or triamcinolone) of ≥24 weeks duration; 2) study participants with COPD of any severity; 3) an ICS as the intervention drug versus control treatment, in which the comparison groups consisted of ICS versus placebo or ICS in combination with LABA versus LABA alone; and 4) the trials had to explicitly report data (including zero events) on the incidence of MI, CV death or overall mortality.
Controlled observational studies (case control, prospective cohort or retrospective cohort) reporting on MI or mortality with ICS exposure compared to those without ICS exposure in COPD were also evaluated.
Exclusion criteria
We restricted the analysis of RCTs to trials of >24 weeks duration to evaluate the long-term CV effects of ICS use. RCTs in patients with asthma or acute exacerbations of COPD were excluded.
Search strategy
An initial search which yielded 30 long-term RCTs of ICS from 651 citations was originally carried out in May 2008 as part of an earlier systematic review 7, covering PubMed and EMBASE by using the clinical trial filters in conjunction with drug and disease search terms (“fluticasone” or “budesonide” or “beclometasone” or “beclomethasone”) and “chronic” and “obstructive”. Y.K. Loke and C.S. Kwok continued updating the search until April 30, 2009, and added the drug term “triamcinolone” to the above trial search with no language restrictions. A separate search string was used to identify observational studies: “inhaled corticosteroids” AND “cohort OR case–control” AND “mortality OR death OR myocardial OR cardiovascular” AND “chronic obstructive”. Published and unpublished trials were retrieved from the Cochrane Database of systematic reviews, websites of the US Food and Drug Administration, European regulatory authorities, manufacturers' product information sheets and the manufacturers' clinical trials register of fluticasone and beclometasone (GlaxoSmithKline) 8, and budesonide (AstraZeneca) 9. The bibliographies of included studies and the Web of Science Cited References search were used to identify relevant citing articles.
Study selection
Two reviewers (Y.K. Loke and C.S. Kwok) independently and in duplicate scanned all titles and abstracts that indicated the study was an RCT or observational study evaluating the use of ICS in patients with COPD. After obtaining full reports of potentially relevant RCTs and observational studies, the same two reviewers independently assessed eligibility from full text articles. Full consensus regarding eligibility and matching between journal publications and company trial reports was obtained after consultation with a third reviewer (S. Singh).
Study characteristics
A pre-specified protocol was used to record: the location and duration of the RCT (in weeks); the spirometric criteria used to diagnose COPD in participants; the primary outcome measure; the dose and frequency of ICS and control interventions; mean age and sex of participants; the severity of COPD in the participants as mean predicted forced expiratory volume in 1 s (FEV1); previous ICS corticosteroid use; and the proportion of current smokers and patients with pre-existing CV disease or CV risk factors when available. The design and relevant data sources, duration of follow-up, the number of study participants and their selection criteria were recorded for the observational studies.
Risk of bias assessment
Two reviewers independently and in duplicate assessed the reporting of blinding, allocation concealment, withdrawals and the loss to follow-up in RCTs. To determine the strength of adverse event monitoring, the frequency and type of adverse event monitoring during the follow-up period were evaluated based on the recommendations in the Cochrane Handbook for Systematic Reviews of Interventions on assessing adverse effects 10. Information on the selection of participants, the comparability of cases and controls, and methods used in ascertaining exposure and outcomes, and the sources of support were extracted for the observational studies. The risk of publication bias was assessed using funnel plot and Egger's test. Evidence of asymmetry from Egger's test was considered to be a p-value <0.1 11.
Outcome measures
The end-points of incidents of fatal and nonfatal MI and CV death were pre-specified as the co-primary outcome measures. A composite CV mortality end-point comprising of fatal MI, fatal stroke, sudden death, cardiac arrest and fatal arrhythmias was constructed for trials that did not report on the specific end-point of CV death but provided mortality data on individual CV end-points 12. The CV end-points were ascertained through routine serious adverse events (life threatening, require hospitalisation or lead to significant disability or death) reported within each trial and may not have been prospectively defined in a uniform fashion across the trials, because none of the RCTs were prospectively designed to assess the CV risk of ICS use. The end-point of all-cause mortality or overall mortality (inclusive of CV death) was pre-specified as the secondary outcome measure.
Data extraction
Two reviewers independently and separately extracted data (including zero events) on MI, CV death and mortality among trial listings of adverse events or serious adverse events. Data in the clinical trials register and the regulatory documents were reconciled with data in the published journal article when possible, and authors were contacted for data clarification where needed. If there were multiple reports for a particular study, data from the recent versions were extracted. We avoided double counting of trials by cross checking published and unpublished studies. We extracted the crude and adjusted risk ratios for CV events and mortality from the observational studies. Two reviewers (Y.K. Loke and C.S. Kwok.) were independently involved in all stages of study selection, data extraction and risk of bias assessment. Discrepancies were resolved with 100% agreement after rechecking the source papers, further discussion among the reviewers, and consultation with a third reviewer (S. Singh), with full consensus obtained before drafting the article.
Statistical analysis
RevMan (version 5.021; Nordic Cochrane Center, Copenhagen, Denmark) was used to calculate relative risk (RR) and 95% CI for the outcome of MI, CV death and all-cause mortality. Outcome data on trial participants were analysed using a 2×2 format according to the “intention to treat” principle. All reported p-values are two sided with significance set at <0.05. Statistical heterogeneity was assessed using the Cochrane I2 statistic, with I2 >25% indicating moderate statistical heterogeneity and I2 >50% indicating a substantial level of heterogeneity 13. We planned to pool data across studies using the fixed-effects models if substantial statistical heterogeneity was not present. If substantial statistical heterogeneity was present (I2 >50%), we planned to explore sources of heterogeneity and the effect of individual study characteristics and subgroups on the risk estimates.
A predefined sensitivity analyses was performed to explore the influence on effect size of the choice of comparators, statistical models (fixed versus random effects), duration of the trials (limited to the trials >1 yr in duration), and the risk of bias by restricting the analysis to RCTs at low risk of bias (adequate sequence generation, allocation concealment and double-blinding, with clear reporting of loss to follow-up). We evaluated the effect of ICS dose by excluding data from intervention arms where participants were randomised to lower doses of ICS (fluticasone ≤500 μg daily and budesonide ≤400 μg daily).
Risk ratios (RR or hazard ratio, adjusted where available) from the observational studies were pooled separately from the RCTs, using the generic inverse variance method with fixed effects model. We assumed similarity between the risk ratio and OR because CV events and deaths were assumed to be rare events 14.
RESULTS
Trial characteristics
The flow chart of study selection is shown in figure 1⇓. Of the 715 citations retrieved, 23 RCTs fulfilled our inclusion criteria 15–37. Trial characteristics are shown in table 1⇓. These trials enrolled a total of 23,396 participants with COPD, with 12,332 receiving ICS versus 11,064 controls. The duration of the trials ranged from 24 to 160 weeks, with 16 trials being longer than 52 weeks in duration 15–20, 22, 23, 25, 27–29, 32, 33, 36, 37. The sample size was variable and the number of participants in the trials ranged from 186 23 to 6,184 18. Inhaled fluticasone was evaluated in 16 trials 15–18, 20–27, 30, 31, 35, 37, inhaled budesonide in six trials 19, 28, 32–34, 36, and inhaled triamcinolone in only one trial 29. Most trials enrolled participants with severe COPD, as the mean FEV1 of the participants was <50% for the majority of trials, compared to >50% for only a few trials 28, 29, 35. The majority of the participants were males, with proportions of current smokers ranging from 22% 35 to 90% 29. COPD was consistently defined in the RCTs with spirometric criteria and the majority of trials excluded patients with asthma, except the Lung Health Study 29 which had <10% of participants with asthma in both arms. The trial by Paggiaro et al. 31 had some patients with atopy 31, while SCO40041 23 and SCO3002 did not specify these exclusions 25.

Flow chart showing the study selection. RCTs: randomised controlled trials; ICS: inhaled corticosteroids; COPD: chronic obstructive pulmonary disease; CV: cardiovascular.
Characteristics of randomised controlled trials included in the analysis of cardiovascular(CV) events and mortality
The trial quality was variable (table 2⇓). All the RCTs had blinding of participants and personnel 15–37. The loss to follow-up was variable and ranged from no loss to follow-up (0 %) 35–37 to 4.9 % 16. Similarly, the withdrawal rates were variable and ranged from <1% 35 to 52% 16. Nine RCTs provided detailed descriptions regarding blinding, adequate sequence generation, allocation concealment, and clear reporting of loss to follow-up and were at low risk of bias 15–18, 27, 31, 35–37. The remaining 14 RCTs were at unclear risk of bias 19–21, 22–26, 28–30, 32–34. 23 RCTs reported on overall mortality 15–37, of which 20 trials reported on MI 15–18, 20–28, 30–32, 34–37 and 20 trials reported on CV death 15–18, 20–31, 34–37. Data on MI, CV death and overall mortality in the RCTs are shown in table 3⇓.
Risk of bias assessment of included randomised controlled trials of inhaled corticosteroids in chronic obstructive pulmonary disease(COPD)#
Cardiovascular(CV) events and all-cause mortality in randomised controlled trials of inhaled corticosteroids in chronic obstructive pulmonary disease
Main findings
ICS use was not associated with a significant effect on the risk of MI (105 (1.0%) out of 10,222 versus 107 (1.2%) out of 8,951 for control; RR 0.95 (95% CI 0.73–1.23); p = 0.68) (fig. 2⇓). There was no evidence of statistical heterogeneity among the included trials (I2 = 0%) 15–18, 20–28, 30–32, 34–37.
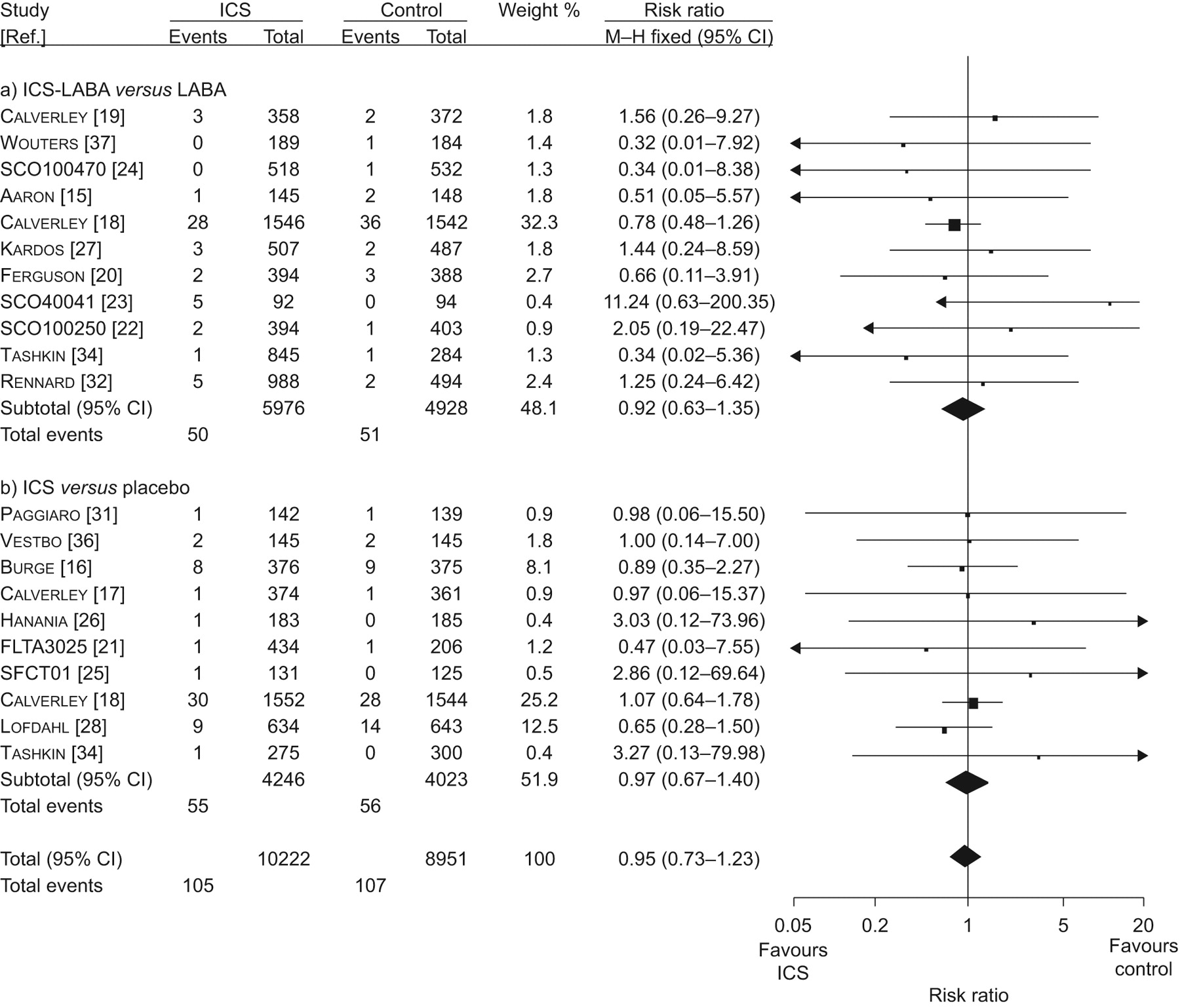
Meta-analysis of randomised controlled trials of inhaled corticosteroids (ICS) versus controls for myocardial infarction. a) ICS-long acting β2-agonists (LABA) versus LABA and b) ICS versus placebo. a) Chi-squared = 6.16; degrees of freedom (df) = 10 (p = 0.80); I2 = 0%. Test for overall effect: z = 0.43 (p<0.67). b) Chi-squared = 2.79; df = 9 (p = 0.97); I2 = 0%. Test for overall effect: z = 0.16 (p<0.87). Overall: Chi-squared = 9.06; df = 20 (p = 0.98); I2 = 0%. Test for overall effect: z = 0.41 (p<0.68). M–H: Mantel–Haenszel.
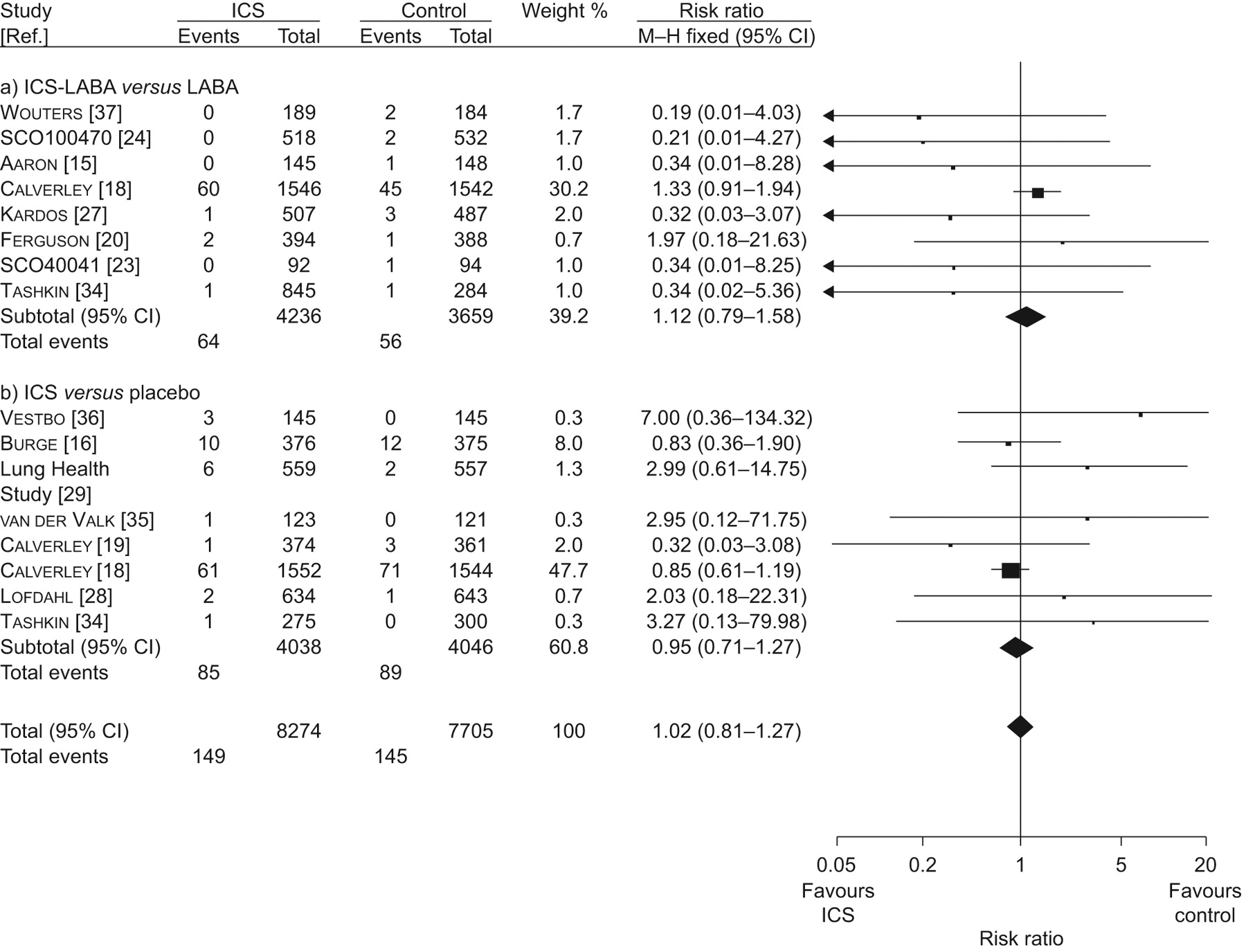
ICS use was not associated with a significant effect on the risk of CV death (149 (1.8%) out of 8,274 versus 145 (1.9%) out of 7,705 for control; RR 1.02 (95% CI 0.81–1.27); p = 0.89) (fig. 3⇓). There was no evidence of statistical heterogeneity among the included trials (I2 = 0%) 15–18, 20–31, 34–37.

Meta-analysis of randomised controlled trials of inhaled corticosteroids (ICS) versus controls for cardiovascular death. a) ICS-long acting β2-agonists (LABA) versus LABA and b) ICS versus placebo. a) Chi-squared = 6.46; degrees of freedom (df) = 7 (p = 0.49); I2 = 0%. Test for overall effect: z = 0.62 (p<0.53). b) Chi-squared = 6.55; df = 7 (p = 0.48); I2 = 0%. Test for overall effect: z = 0.33 (p<0.74). Overall: Chi-squared = 13.85; df = 15 (p = 0.54); I2 = 0%. Test for overall effect: z = 0.14 (p<0.89). M–H: Mantel–Haenszel.
ICS use was not associated with a significant effect on the risk of mortality (580 (5.2%) out of 11,241 versus 596 (5.8%) out of 10,211 for control; RR 0.96 (95% CI 0.86–1.07); p = 0.43) 15–37. There was no evidence of statistical heterogeneity among the included trials (I2 = 0%).
Sensitivity analysis
These estimates were robust to the choice of comparators in subgroup analysis. ICS use was not associated with a significant effect on the risk of MI when combined ICS+LABA was compared to LABA alone (RR 0.92 (95% CI 0.63–1.35), p = 0.67; I2 = 0%) or when ICS was evaluated against placebo (RR 0.97 (95% CI 0.67–1.40), p = 0.87; I2 = 0%). Similarly, ICS use was not associated with a significant effect on the risk of CV death when combined ICS+LABA was compared to LABA alone (RR 1.12 (95% CI 0.79–1.58), p = 0.53; I2 = 0%) or when ICS was evaluated against placebo (RR 0.95 (95% CI 0.71–1.27), p = 0.74; I2 = 0) Combined ICS and LABA use did not significantly reduce MI (RR 1.09 (95% CI 0.68–1.75), p = 0.71; I2 = 0%) or CV death (RR 0.81 (95% CI 0.58–1.12), p = 0.20; I2 = 0%) against placebo. The random effects analysis on MI (RR 0.92 (95% CI 0.70–1.20), p = 0.52; I2 = 0%) and CV death (RR 1.01 (95% CI 0.81–1.27), p = 0.90; I2 = 0%) associated with ICS use yielded effect sizes similar in magnitude and direction to those from the fixed-effects analysis.
The sensitivity analysis on MI (RR 0.95 (95% CI 0.72–1.24), p = 0.70; I2 = 0%) and CV death (RR 1.02 (95% CI 0.82–1.28), p = 0.84; I2 = 2%) associated with ICS use in trials of ≥52 weeks duration [15–20, 22, 23,25 27–29, 32, 33, 36, 37] was similar in magnitude and direction to the overall estimates. The sensitivity analysis on MI (RR 0.91 (95% CI 0.67–1.24), p = 0. 56; I2 = 0%) and CV death (RR 1.00 (95% 0.79–1.25), p = 0.97; I2 = 9%) associated with ICS use in RCTs at low risk of bias 15–18, 27, 31, 35–37 was similar in magnitude and direction to the overall estimates. The exclusion of trial arms with lower doses of ICS use did not change the direction or magnitude of the estimates for MI (RR 0.88 (95% CI 0.66–1.16), p = 0.36; I2 = 0%) and CV death (RR 1.03 (95% CI 0.81–1.28), p = 0.82; I2 = 5%).
Observational studies
12 observational studies were included 4, 5, 38–47. Details of the included studies and the risk of bias are shown in table 4⇓. Confounding was potentially present in several studies, with differences in baseline characteristics between the study groups 5, 40, 43, 44, 46. ICS exposure was estimated from dispensing records and dosages were usually extrapolated from the amounts dispensed 39, 43. It was uncertain if patients with concomitant asthma were reliably excluded (misclassification bias) 40. Immortal time bias, when patients exposed to ICS had an inappropriate interval of immortality compared with patients exposed to controls that did not have this interval, was a potential bias in certain studies 4, 40, 42–45. Some studies were funded by manufacturers of ICS 41, 44, 45, 47.
Characteristics of observational studies of inhaled corticosteroids(ICS) and cardiovascular (CV) events or mortality
ICS were not associated with a significantly reduced risk of MI (RR 0.83, 95% CI 0.63–1.08) in one observational study reporting on MI 39. Two observational studies reported a significant association between ICS exposure and reduction in CV death, but did not specify details on the causes of death 4, 5. Pooled analysis of these two studies yielded an RR of 0.79 (95% CI 0.72–0.86, p<0.0001) for CV death, with moderate statistical heterogeneity (I2 = 44%) (fig. 4a⇓). 11 observational studies reported on overall mortality 4, 5, 38, 40–47. ICS use was associated with a significantly reduced risk of death in a meta-analysis of these 11 observational studies (RR 0.78, 95% CI 0.75–0.80; p<0.0001) (fig. 4b⇓) 4, 5, 38, 40–47. However, there was evidence of moderate statistical heterogeneity among the included studies (I2 = 33%).
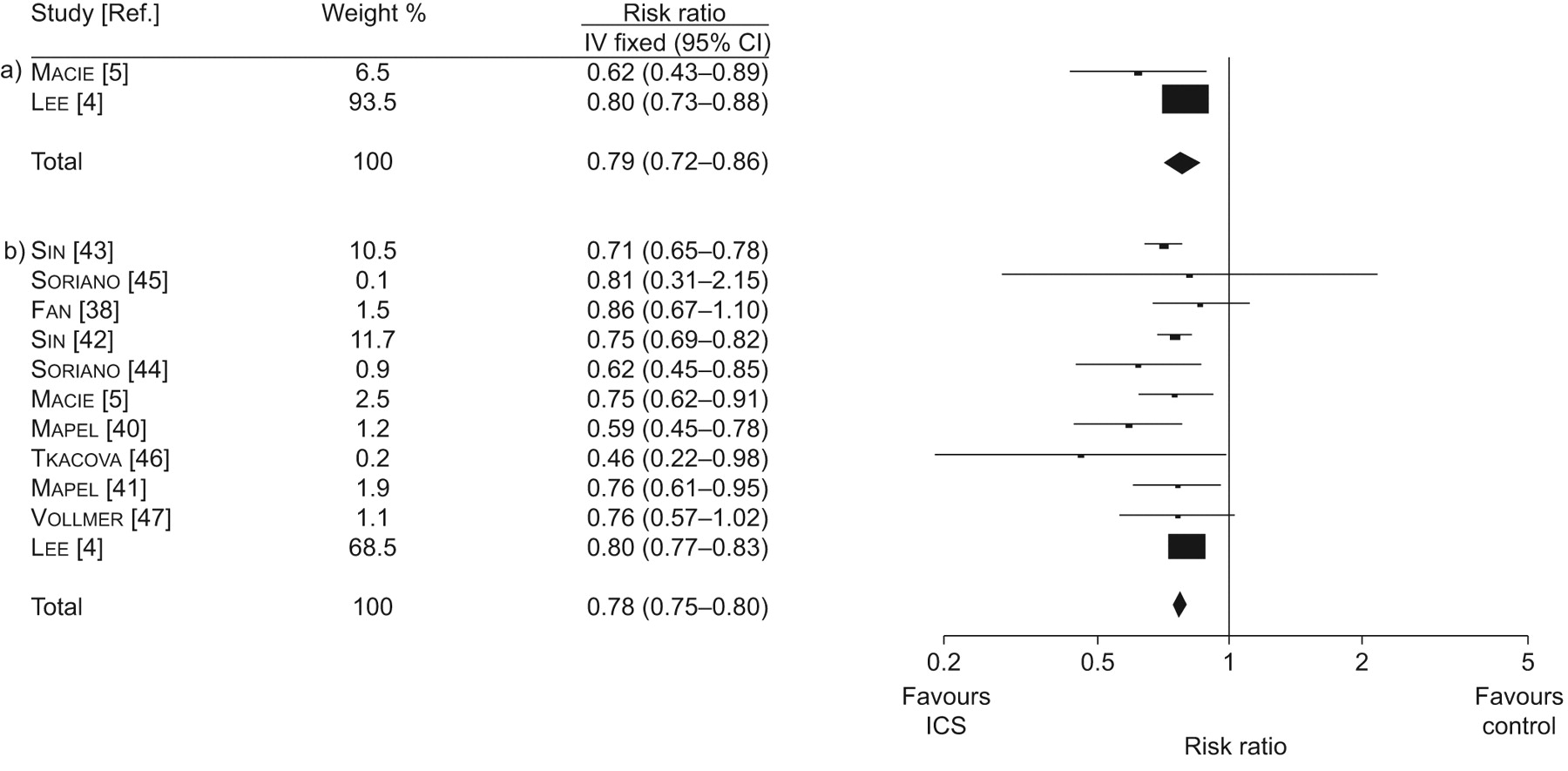
Meta-analysis of inhaled corticosteroids (ICS) versus controls for a) cardiovascular death and b) overall mortality in observational studies. a) Chi-squared = 1.79; degrees of freedom (df) = 1 (p = 0.18); I2 = 44%. Test for overall effect: z = 5.10 (p<0.00001). b) Chi-squared = 14.95; df = 10 (p = 0.13); I2 = 33%. Test for overall effect: z = 16.22 (p<0.00001). IV: inverse variance.
Publication bias
The funnel plot for mortality appeared to be symmetrical for the RCTs (fig. 5a⇓) and showed asymmetry for the observational studies (fig. 5b⇓). The Egger's test for publication bias was nonsignificant for RCTs (p = 0.23), with evidence of significant publication bias in the observational studies (Egger's test p = 0.05).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plots of risk ratios for overall mortality in the a) trials and b) observational studies. ▪: inhaled corticosteroid (ICS) long acting β2-agonists (LABA) versus LABA; •: ICS versus placebo.
DISCUSSION
Our meta-analysis has found conflicting evidence on the effects of ICS therapy on cardiovascular events and mortality in patients with COPD. We were unable to demonstrate a significant beneficial effect of ICS therapy on MI or CV death in RCTs. In contrast, our meta-analysis showed significant relative reductions (magnitude of ∼20%) in the risk of CV and all-cause mortality with ICS-exposed patients in the observational studies.
Methodological issues
Publication or outcome reporting bias in the observational studies may partly account for the differences in results between the observational studies and RCTs. The meta-analysis of observational studies was limited to available published studies, and journal publications may favour manuscripts with positive results 48. In contrast, our meta-analysis of RCTs included unpublished data from manufacturers' trial registries thus minimising the risk of publication bias.
The presence of immortal time bias may partly account for some of the mortality reduction seen in observational studies, but is not the only explanation for these divergent findings. A time-dependent analysis accounting for the period of ICS exposure versus control exposure (OR 1.00, 95% CI 0.79–1.26) negated the significant beneficial effect seen using a fixed time analysis (OR 0.69, 95% CI 0.55–0.86) in a study that measured 90-day mortality 49. A significant beneficial association, albeit lower in magnitude, was seen with ICS exposure in another study that minimised the risk of immortal time bias 41. Potential confounders, such as smoking status and lung function, and unknown residual confounding factors, such as co-existing asthma, along with the differential use of home oxygen in patients may have contributed to the perceived effect on mortality in the observational studies.
The apparent lack of CV benefit in the trials which typically exclude patients with serious comorbidities cannot conclusively rule out the potential for a CV benefit in patients with COPD seen in the observational studies. The rates of concomitant smoking in the observational studies may have been lower than that of RCTs where nearly 50% of COPD participants had 10 pack-yrs of smoking history. Factors other than smoking, such as biomass, air pollution and poor nutrition, may contribute to the burden of COPD in community patients. Certain subgroups of patients in the observational studies, especially those with severe comorbidities and a higher risk of CV events, may potentially derive a CV benefit from ICS use.
Comparisons with previous analysis
The finding of a lack of CV effect in our intention-to-treat meta-analysis of 23 published and unpublished trials involving 23,396 patients should be distinguished from other meta-analysis of ICS use limited to the published trials. Our meta-analysis had a greater ability to detect any significant difference on mortality with more precise estimates of treatment effect as shown by our relatively narrow 95% CI (0.86–1.07) for the RR of overall mortality. An earlier pooled analysis (seven published trials, n = 5,085, mean duration of follow-up = 26 months) reported a reduction in mortality with ICS use (adjusted hazards ratio 0.73, 95% CI 0.55–0.96) but had less than one quarter the number of patients than our analysis 50. The effect was more pronounced in females and former smokers, and the benefits were driven by reduction in cancer deaths 50. A subsequent Cochrane systematic review which pooled data from nine trials 51, and another recent meta-analysis of five trials found no evidence of a mortality benefit with ICS use 52.
Our failure to detect a significant effect on MI and CV death with ICS (fluticasone, budesonide and triamcinolone) use should be distinguished from a post hoc subgroup analysis of inhaled budesonide versus placebo on ischaemic cardiac events (angina pectoris, coronary artery disorder and MI) in the European Respiratory Society's study on Chronic Obstructive Pulmonary Disease (EUROSCOP) 28. Their analysis included 1,175 participants, approximately one fifth of the number of participants in our analysis, with mild COPD (average age 52.5 yrs) and reported a significantly lower risk of ischaemic cardiac events with inhaled budesonide (RR 0.58, 95% 0.35–0.98; p = 0.043). The contrasting findings could be partly explained by the inclusion by EUROSCOP of different end-points of angina, ischaemia and coronary artery disorder in patients with milder COPD. However, applying the end-points of ischaemic cardiac events of EUROSCOP to the similar 3 yr Towards a Revolution in COPD Health (TORCH) trial 18, shows no significant difference in the rate of ischaemic cardiac events in inhaled fluticasone (56 (36.%) out of 1,552) when compared to placebo (50 (3.2%) out of 1,544). We did not detect any intraclass differences in the risk of CV events between inhaled fluticasone and inhaled budesonide in our meta-analysis.
The potential mechanisms by which ICS modulate CV outcomes remain uncertain. ICS could potentially ameliorate CV disease by reducing exacerbations because acute exacerbation in COPD may precipitate CV disease 53. The pathology of COPD includes inflammation and/or alterations in repair mechanisms. The “spill-over” of inflammatory mediators into the systemic circulation in COPD is linked to the development of CV disease 54. However, ICS use may have limited CV benefit because ICS use does not reduce markers of systemic inflammation (serum CRP or interleukin-6 levels), with little impact on neutrophilic inflammation or matrix remodelling relevant to CV disease in COPD 54, 55.
Limitations
Our meta-analysis has several limitations, which mainly stem from the quality of reported data. The RCTs did not use specific definitions of MI or CV death, and inconsistent adverse events reporting may account for some missing outcome data. Our estimates for MI and CV death are relatively imprecise with wide CIs due to the low CV event rates in the trials. Thus, we cannot rule out the possibility of a relative reduction of 27% for MI and 20% for CV death with ICS. 14 trials in the analysis were at unclear risk of bias. The high withdrawal rates in certain trials may also mask any differences in treatment effect. There was potential clinical heterogeneity among the included trials and we cannot completely discount the possibility of statistical heterogeneity because the heterogeneity tests may be underpowered due to low event rates.
We excluded trials shorter than 6 months, but it is unlikely that a substantial CV effect would be discernible in trials of shorter duration. In the absence of patient-level data, we could not determine ICS dose–response relationships 42. However, the exclusion of lower dose intervention arms did not change the direction or magnitude of the estimates for MI and CV death. We could not evaluate the influence of age, severity of COPD, and pre-existing CV risk factors or concomitant statin 56, or angiotensin inhibitor use on CV events associated with ICS use.
Despite these limitations, the apparent absence of improvements in CV and mortality outcomes with ICS use in the trials should be seen in the context of the potential benefit of ICS use on exacerbations, and improved quality of life in recent meta-analyses 51, 57. Our comprehensive meta-analysis informs the recent debate on the role of ICS in COPD 58, 59. RCTs that have reported beneficial effects on exacerbations, but only after a LABA were added to the ICS, were limited by the discontinuation of existing treatment and the absence of the fundamental “intention-to-treat analysis“ 60. Two recent trials 15, 18, designed for a proper intention-to-treat analysis of the primary outcomes, both found no benefit of ICS in COPD 60. ICS do not reduce the decline in FEV1 in COPD 2, 51. The beneficial effect of a LABA-ICS combination may possibly be attributed to the LABA component, without any additional benefit from the addition of an ICS 60.
Future research
Appropriate factorial analyses evaluating the effect of each component of the LABA-ICS combination inhaler, and re-analysis of patient level data by pre-existing ICS use in trials may clarify the optimal role of ICS use in COPD 61. A large-scale pragmatic trial in community patients may also help to clarify the CV effects of ICS use.
The benefits of ICS in reducing exacerbations and improving symptoms should be weighed against the potential for harm, such as an increased risk of pneumonia which appears to be limited to inhaled fluticasone 7, but are uncertain for budesonide 62, 63. Recent data suggest that fluticasone has no significant impact on bone demineralisation 64.
Clinicians will need to carefully evaluate the strengths and limitations of the current evidence concerning the effects of ICS therapy on cardiovascular events when making a treatment decision. Further research to clarify these divergent findings is clearly needed.
Support statement
The design and conduct of the study; the collection, management, analysis and interpretation of the data; and the preparation, review or approval of the manuscript was independent of any sources of funding. There were no sources of funding for this work. No specific financial interests and relationships and affiliations relevant to the subject of their manuscript were reported by Y.K. Loke, C.S. Kwok and S. Singh. S. Singh is supported by the Johns Hopkins Clinical Research Scholars Program (Baltimore, MD, USA). Funding for this study was provided by grant number 1KL2RR025006-03 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. The contents of the study are solely the responsibility of the authors and do not necessarily represent the official view of NCRR or NIH.
Statement of interest
None declared.
Acknowledgments
We would like to thank J. Vestbo (North West Lung Centre, University of Manchester, Manchester, UK) and S. Aaron (University of Ottawa, ON, Canada) for providing data related to the subject of the manuscript.
Footnotes
-
For editorial comments see page 949.
- Received June 17, 2009.
- Accepted November 6, 2009.
- © ERS Journals Ltd
References










