





Abstract
The aim of our study was to investigate if hypoglycaemia correlates with outcome in community-acquired pneumonia (CAP).
We performed a prospective, observational study of consecutive patients presenting with a primary diagnosis of CAP in Lothian (UK). Admission plasma glucose was measured and, on this basis, patients were divided into two groups, hypoglycaemic (<4.4 mmol·L−1 or <79.0 mg·dL−1) and nonhypoglycaemic (≥4.4 mmol·L−1 or ≥79.0 mg·dL−1). Outcomes of interest were 30-day mortality, need for mechanical ventilation and inotropic support. Multivariable logistic regression was used to compare these outcomes in hypoglycaemic patients to nonhypoglycaemic patients, adjusting for diabetes mellitus, prior statin use and Pneumonia Severity Index.
In total, 1,050 patients were included in the study with 5.4% classified as hypoglycaemic. Increased rates of 30-day mortality (28.1% versus 7.5%, p<0.0001), need for mechanical ventilation (29.8% versus 6.5%, p<0.0001) and need for inotropic support (21.1% versus 4.8%, p<0.0001) were observed in hypoglycaemic patients compared with nonhypoglycaemic patients. On multivariable analysis, hypoglycaemia was independently associated with increased 30-day mortality (OR 2.25, 95% CI 1.1–4.7; p = 0.03), need for mechanical ventilation (OR 3.8, 95% CI 1.9–7.5; p = 0.0002) and need for inotropic support (OR, 2.9, 95% CI 1.4–6.3; p = 0.0006).
Admission hypoglycaemia is associated with increased 30-day mortality, need for mechanical ventilation and inotropic support in patients presenting with CAP.
There has been increasing interest in the influence of glycaemia on outcome in acutely unwell patients. Hypoglycaemia has previously been shown to be a predictor of adverse outcome in patients with Gram-positive and Gram-negative sepsis 1–3.
Although hyperglycaemia has been shown to be a factor associated with poor outcome in community-acquired pneumonia (CAP) 4–6 and is one of 20 variables used to calculate the Pneumonia Severity Index (PSI) 4, to date no study has investigated the association of hypoglycaemia and outcome in CAP. The aim of this study was to investigate if admission hypoglycaemia is associated with increased risk of mortality, need for mechanical ventilation and need for inotropic support in patients presenting with CAP.
METHODS
The Edinburgh Pneumonia Study is a prospective observational study of adult patients presenting with a diagnosis of CAP between January 2005 and January 2008 to NHS Lothian (UK). This study reports a sub-analysis of this study investigating the effect of hypoglycaemia on outcome. The study was approved by the Lothian Research Ethics Committee (UK).
Patients were included in the study if they presented with a new infiltrate on chest radiography and had three or more of the following symptoms or signs: cough, sputum production, breathlessness, pleuritic chest pain or signs consistent with pneumonia on auscultation.
Exclusion criteria were as follows. 1) Hospital-acquired pneumonia: development of symptoms >48 h following admission or discharge from an acute care facility <2 weeks prior to admission; 2) active thoracic malignancy; 3) immunosuppression: defined as current, >28 day, use of oral prednisolone at any dose or other immunosuppressive drugs (methotrexate, azathioprine, cyclosporin and anti-tumour necrosis factor-α agents), or patients with solid organ transplantation; 4) known adrenal insufficiency; 5) intravenous or subcutaneous insulin therapy on admission prior to measurement of plasma glucose; and 6) pulmonary embolism and patients in whom active treatment was not considered appropriate (palliative care).
Site of care and data collection
At the study sites in NHS Lothian, patients presented either as self-referral to the Emergency Dept or via general practitioner referral to a Medical Assessment Unit. Patients were reviewed by the medical team and the decision of whether to admit or discharge the patient was made.
All patients had baseline observations (pulse, blood pressure, respiratory frequency and temperature) and standard blood tests (full blood count, urea and electrolytes, liver function tests, coagulation profile and C-reactive protein) measured on admission. Blood culture requests were left to the discretion of the attending physician. All observations and blood tests were taken within 4 h of hospital admission.
Subsequently, patients spent 12–24 h in the Medical Assessment Unit, from where they were discharged or moved to a specialist ward. Critically ill patients could be admitted at any time to the intensive care unit (ICU) for invasive ventilation and/or inotropic support or to the high dependency unit (HDU), which provides intensive monitoring as well as noninvasive ventilation (bilevel or continuous positive airway pressure ventilation), and/or inotropic support. All patients received standard antibiotic therapy in accordance with British Thoracic Society (BTS) guidelines 7.
Glucose measurement
All patients had plasma glucose measured on admission (all readings were taken within 4 h, prior to any corrective treatment). The study cohort was divided into two groups on the basis of admission plasma glucose level: 1) hypoglycaemic (glucose <4.4 mmol·L−1 or <79.0 mg·dL−1), as previously defined 8; and 2) nonhypoglycaemic (glucose ≥4.4 mmol·L−1 or ≥79.0 mg·dL−1).
The hypoglycaemic group was then subdivided further into the following groups: mild hypoglycaemia (3.9–4.39 mmol·L−1 or 70–78.9 mg·dL−1); moderate hypoglycaemia (3.4–3.89 mmol·L−1 or 61–69.9 mg·dL−1); and severe hypoglycaemia (<3.4 mmol·L−1 or <61 mg·dL−1).
Severity assessment scores on admission
The following severity scores were analysed for all patients on admission.
PSI
The PSI 4 is a well-validated prediction scale for 30-day mortality in CAP composed of the following 20 characteristics: age, sex, nursing home residence, neoplastic disease, cerebrovascular disease, congestive cardiac failure, chronic renal disease, chronic liver disease, altered mental status, respiratory frequency ≥30 breath·min−1, systolic blood pressure <90 mmHg, temperature <35°C or >40°C, cardiac frequency >125 beats·min−1, pH <7.35, blood urea >10.7 mmol·L−1, sodium <130 mEq·L−1, glucose >13.9 mmol·L−1, haematocrit <30%, arterial oxygen tension <60 mmHg, and pleural effusion.
With use of these data, patients were classified into five risk classes (1–5) according the criteria created by Fine et al. 4. In the original Pneumonia Patient Outcome Research Team cohort study, 30-day mortality ranged from 0.1% for patients with a class 1 rating to 27% for patients with a class 5 rating.
CURB65
CURB65 is a validated method of predicting in-patient mortality associated with CAP recommended by the BTS 7, 9. It consists of new onset mental confusion, urea >7 mmol·L−1, respiratory frequency ≥30 breaths·min−1, systolic blood pressure <90 mmHg or diastolic blood pressure ≤60 mmHg, and age ≥65 yrs.
BTS guidelines suggest that patients with a CURB65 score of 0–1 be considered for outpatient treatment, patients with a CURB65 score of 2 be considered for a short in-patient hospital stay, and that patients with a CURB65 score ≥3 have severe pneumonia requiring in-patient management, and ICU or HDU care should be considered, particularly for patients with a CURB65 score ≥4 7.
Systemic inflammatory response syndrome
Systemic inflammatory response syndrome (SIRS) is a well-recognised criteria of the sepsis syndrome 10. It is defined as two of the following variables: temperature >38°C or <36°C, cardiac frequency >90 beats·min−1, respiratory frequency ≥20 breaths·min−1 or arterial carbon dioxide tension <4.3 kPa (32 mmHg), and white blood cell count >12,000 cells·mm−3 or <4,000 cells·mm−3.
Severe sepsis is defined as SIRS with failure of one or more organs, in the context of suspected or proven infection. Septic shock refers to SIRS with hypotension not responsive to adequate fluid resuscitation, also in the context of suspected or proven infection 10.
Outcomes
The outcomes of interest were 30-day mortality, need for mechanical ventilation and need for inotropic support. The indications for mechanical ventilation and inotropic support were left to the discretion of the attending physician.
Statistical analysis
All data were analysed using SPSS (version 13; SPSS Inc., Chicago, IL, USA). Descriptive statistics of demographic and clinical variables are presented as median (interquartile range) unless otherwise stated. The Chi–squared test was used to compare categorical data between groups. The Mann–Whitney U-test was used for the comparison of two groups of continuous data and the Kruskal–Wallis test was used for comparison of more than two groups of continuous data. Kaplan–Meier analysis was used for comparison of survival between hypoglycaemic and nonhypoglycaemic groups and between subdivisions of the hypoglycaemic group. The statistical significance was evaluated using the log-rank test.
Univariate analyses were performed for the outcomes of interest in hypoglycaemic patients, nonhypoglycaemic patients and the subgroup of patients without prior diagnosis of diabetes mellitus. We also performed separate univariate analyses comparing the outcomes of interest between mild, moderate and severely hypoglycaemic patients.
We used multivariable logistic regression to compare the outcomes of interest in patients with hypoglycaemia (plasma glucose <4.4 mmol·L−1 or <79.0 mg·dL−1) compared to nonhypoglycaemic patients. We included prior diagnosis of diabetes mellitus, and nonsevere PSI (≤3) versus severe PSI (≥4) to the baseline model. We also adjusted for prior statin use, as previous analysis had found a significant association between statin use and reduced 30-day mortality in patients with CAP 11. A two-tailed p-value <0.05 was considered statistically significant.
RESULTS
In total, 1,269 patients were considered for inclusion into the study. Of these, 1,050 patients met the criteria and were included in the study. A flow chart of patient enrolment into the study is shown in figure 1⇓. Baseline demographic characteristics of the study population and sub-groups are outlined in table 1⇓.
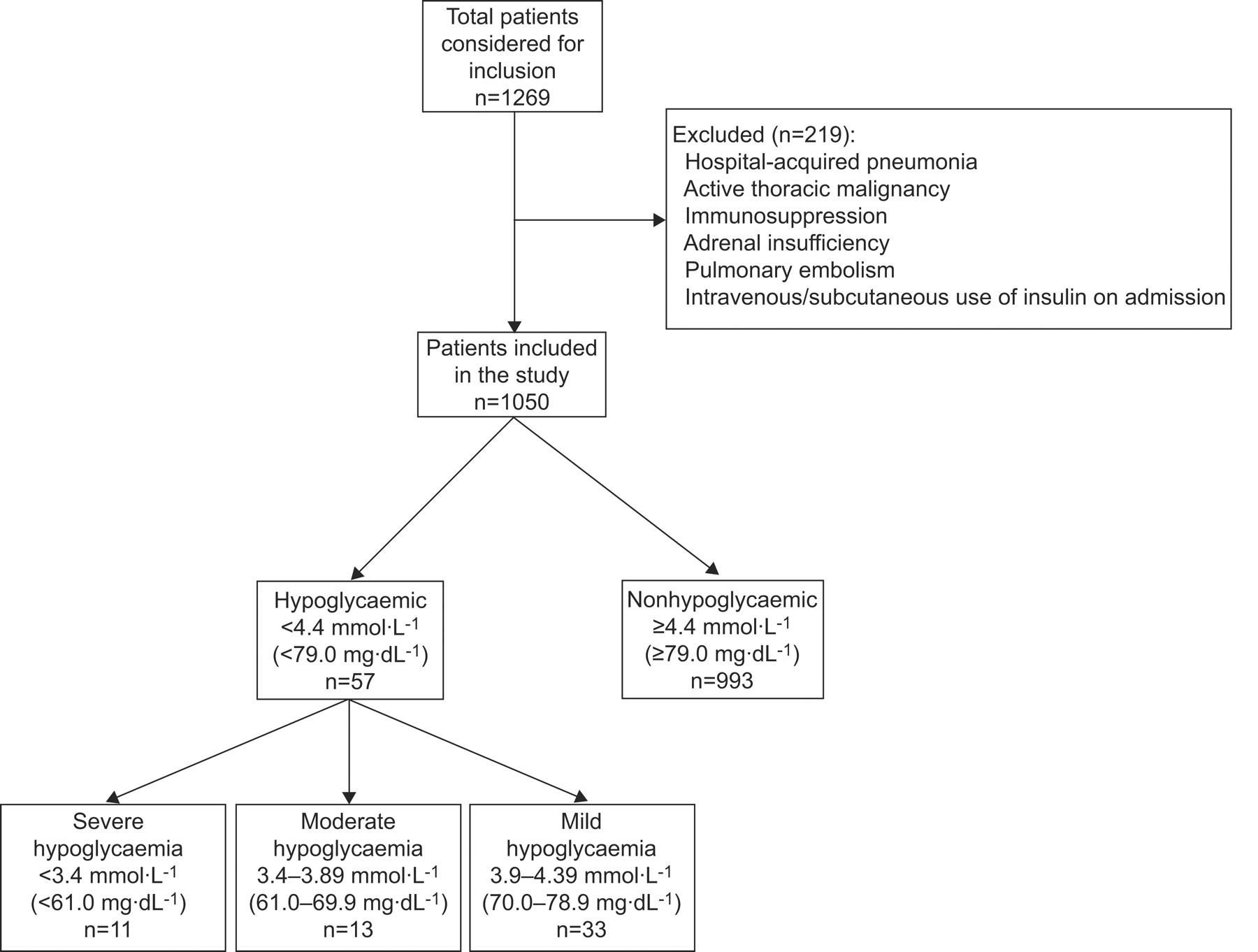
Flow chart of the patients enrolled in the study.
Baseline characteristics of study population
Admission glucose level and outcome
Overall 30-day mortality rate was 8.6%. Mechanical ventilation was required in 7.8% of patients and inotropic support was required in 5.7%; 181 (17.2%) patients were discharged within 24 h. Hypoglycaemic patients had increased risk of 30-day mortality, need for mechanical ventilation and inotropic support compared to nonhypoglycaemic patients (table 2⇓). With increasing severity of hypoglycaemia, there was increased 30-day mortality. There were similar trends for mechanical ventilation and inotropic support, but this failed to reach statistical significance (table 2⇓).
Admission glucose level and outcome
Survival analysis in hypoglycaemic and nonhypoglycaemic patients
Figure 2⇓ shows the survival analysis in hypoglycaemic and nonhypoglycaemic patients and in subdivisions of the hypoglycaemic group, for 30 days after admission. In the hypoglycaemic patient group, mortality occurred earlier in comparison to nonhypoglycaemic patients (log rank = 15.1 on 1 degree of freedom; p<0.0001). Survival analysis in sub-divisions of the hypoglycaemic group is also shown in figure 2⇓ (log rank = 12.7 on 2 degrees of freedom; p = 0.0018).

{kind=link}
{kind=link}
Kaplan–Meier survival analysis in a) hypoglycaemic (▪) and nonhypoglycaemic patients (•), and b) subdivisions of the hypoglycaemic group. ▵: glucose 3.9–4.39 mmol·L−1; □: glucose 3.4–3.89 mmol·L−1; ○: glucose <3.4 mmol·L−1.
Admission glucose level and correlation with severity scores
A greater proportion of patients in PSI class IV or V was observed in the hypoglycaemic group compared with the nonhypoglycaemic group (64.9% versus 43.5%; p = 0.002). Similar trends were seen with regards to the proportion of patients in CURB65 class 3–5 (52.6% versus 30.8%; p = 0.001) (table 1⇑).
Analysis of outcome in hypoglycaemic and nonhypoglycaemic patients stratified by PSI risk class
The rates of 30-day mortality, need for mechanical ventilation and need for inotropic support in hypoglycaemic and nonhypoglycaemic patients, stratified according to PSI class, are shown in table 3⇓. In nonhypoglycaemic patients, there were increasing rates of mortality, need for mechanical ventilation and inotropic support with increasing PSI class (table 3⇓). Trends towards increasing rates of mortality, need for mechanical ventilation and inotropic support were observed with increasing PSI class in hypoglycaemic patients, although this failed to reach statistical significance (table 3⇓).
Stratified outcome of hypoglycaemic and nonhypoglycaemic patients according to Pneumonia Severity Index(PSI) class
Comparison of hypoglycaemic and nonhypoglycaemic groups revealed significantly increased rates of mechanical ventilation in hypoglycaemic patients for PSI classes III and IV and significantly increased rates of inotropic support for PSI class IV. Otherwise, no significant differences were observed between the two groups when stratified according to PSI risk class (table 3⇑).
Association of hypoglycaemia with sepsis
The proportion of patients with severe sepsis or septic shock on admission (as defined by SIRS criteria) and proportion of positive blood cultures in each group is shown in table 4⇓. A greater proportion of patients with severe sepsis or septic shock on admission was observed in the hypoglycaemic group compared to nonhypoglycaemic patients (40.4% versus 14.5%; p<0.0001). A higher proportion of hypoglycaemic patients also had positive blood cultures compared to nonhypoglycaemic patients (29.8% versus 6.8 %; p<0.0001) (table 4⇓). There were no significant differences between the mild, moderate and severe hypoglycaemic groups.
Admission glucose level and correlation with systemic inflammatory response syndrome(SIRS) score and blood cultures
Influence of plasma glucose on outcome in patients without prior diagnosis of diabetes mellitus
At time of presentation, 10.1% of patients had a prior diagnosis of diabetes mellitus. Table 1⇑ shows the frequency of these patients in each group. Of the diabetic group, 28.3% were diet-controlled, 44.3% were taking oral hypoglycaemic agents alone, 25.5% were receiving subcutaneous insulin alone and 1.9% were on a combination of insulin and oral agents. Analysis of patients without prior diagnosis of diabetes mellitus revealed similar trends to the whole cohort, with hypoglycaemic patients showing increased 30-day mortality (28.8% versus 6.6%; p<0.0001), need for mechanical ventilation (32.7% versus 5.9%; p<0.0001) and inotropic support (23.1% versus 4.5%; p<0.0001) compared to nonhypoglycaemic patients.
Multivariable analysis
On multivariable logistic regression, adjusting for variables in the PSI, diabetes mellitus and prior statin use, admission hypoglycaemia (<4.4 mmol·L−1 or <79.0 mg·dL−1) was independently associated with increased 30-day mortality (OR 2.25, 95% CI 1.1–4.7; p = 0.03), increased requirement for mechanical ventilation (OR 3.8, 95% CI 1.9–7.5; p = 0.0002) and increased requirement for inotropic support (OR 2.9, 95% CI 1.4–6.3; p = 0.0006).
DISCUSSION
Our study has found that patients who are hypoglycaemic on admission with CAP have significantly increased rates of 30-day mortality, need for mechanical ventilation and need for inotropic support. This effect was seen independently of prior diabetes mellitus diagnosis and after adjustment for prior statin use and pneumonia severity (PSI criteria). We are not aware of any previous study that has examined the association of hypoglycaemia with outcome in CAP.
Previous studies in patients with septicaemia have shown that hypoglycaemia is a late manifestation of septic shock 3 and is also associated with a high mortality rate (43–90%) 1, 3, 12. In addition, interventional studies have shown that treating low blood glucose directly does not affect outcome in sepsis, suggesting that hypoglycaemia is a marker of adverse outcome rather than being directly responsible for increased mortality rates seen in these patients 13.
Although the direct pathophysiological relationship between hypoglycaemia and adverse outcome in CAP has not been characterised, studies into sepsis provide some insight. Animal studies have shown that endotoxin challenge induces hypoglycaemia in both dogs and rats 14, 15. Hepatic gluconeogenesis has been shown to be important in survival from septic shock and experimental models suggest that sepsis may induce hepatic dysfunction, leading to altered glucose homeostasis 16, 17. Poor perfusion, extensive anaerobic metabolism and increased peripheral glucose utilisation have also been proposed as causative pathophysiological factors involved in the hypoglycaemia observed in sepsis 3, 18. In addition, studies have shown the presence of relative adrenal insufficiency in a proportion of patients with septicaemia 19–22 and this finding has been shown to correlate with adverse outcome 23. This may further explain the underlying cause for hypoglycaemia in CAP and also its influence on outcome.
We postulate that in CAP, similar to septicaemia, hypoglycaemia on admission reflects a sub-group of patients with severe physiological disturbance and subsequent increased rates of 30-day mortality, need for mechanical ventilation and inotropic support. This is supported by our finding that a greater proportion of hypoglycaemic patients had severe sepsis or septic shock, as defined by SIRS criteria.
Our results show that hypoglycaemia on admission is a relatively infrequent finding in patients with CAP (present in only 5.4% of our cohort). However, if present, it represents an additional marker of severity in CAP and such patients should be identified early as being at increased risk of complications. This is further confirmed by our finding that patients with hypoglycaemia were more likely to be classified in higher risk groups on the basis of admission severity scoring (PSI and CURB65). However, hypoglycaemia was a marker of poor outcome, independent of severity.
Kaplan–Meier survival analysis of hypoglycaemic patients in our cohort indicated that the majority of deaths in this group occur early after admission (in the first 7 days). This reinforces the point that, in patients with CAP, admission hypoglycaemia should alert clinicians to a potential need for early aggressive management strategies.
Our findings also show that increasing levels of hypoglycaemia correlate with increasing risk of adverse outcome in CAP with severely hypoglycaemic patients (glucose <3.4 mmol·L−1 or <61.0 mg·dL−1) showing the highest rates of 30-day mortality. Similar trends were seen for the need for mechanical ventilation and inotropic support, although these end-points failed to reach statistical significance, probably due to the small numbers in the different subgroups of hypoglycaemia.
In conclusion, on multivariable analysis, adjusting for diabetes mellitus diagnosis, prior statin use and PSI criteria, admission hypoglycaemia was independently associated with increased risk of 30-day mortality, need for mechanical ventilation and inotropic support in patients presenting with CAP.
Support statement
J.D. Chalmers is supported by a Clinical Research Training Fellowship from the Medical Research Council (London, UK).
Statement of interest
None declared.
Footnotes
-
Earn CME accreditation by answering questions about this article. You will find these at the back of the printed copy of this issue or online at www.erj.ersjournals.com/misc/cmeinfo.dtl
- Received December 29, 2008.
- Accepted June 4, 2009.
- © ERS Journals Ltd
References










