





Abstract
The diagnosis of tuberculous pleural effusion (TBPE) is frequently problematic. Several markers of TBPE in pleural fluid have been evaluated, with different results.
Pleural effusions from 96 patients were classified on the basis of definitive diagnosis as tuberculous (n = 39), neoplastic (n = 42) or parapneumonic (n = 15). Adenosine deaminase (ADA), ADA isoform ADA-2, interferon (IFN)-γ, CD3+/DR+ T-lymphocytes and interleukin (IL)-12 p40 were determined in all 96 effusions. The efficiency of IL-12 p40 for diagnosis of TBPEs was evaluated, in comparison with those of the other parameters, by comparing the areas under their receiver operating characteristics.
With the threshold value of 550 pg·mL−1, IL-12 p40 had a sensitivity of 92.3% (36 out of 39) and specificity of 70.2% (17 false positives). The misclassification rate of IL-12 p40 was significantly greater than those of ADA-2 and ADA. Among TBPEs, ADA correlated significantly with ADA-2, and IFN-γ with ADA and IL-12 p40.
Although tuberculous pleural effusions show values of interleukin-12 p40 that are significantly higher than neoplastic and parapneumonic fluids, this parameter is less efficient than adenosine deaminase, adenosine deaminase isoform 2 and interferon-γ. Its routine determination is, accordingly, not justified.
The diagnosis of tuberculous pleural effusion (TBPE), one of the most frequent causes of pleural effusion 1, is not infrequently problematic due to the unspecificity of the diagnostic tests used 2–5. Some determinations from pleural fluid (mycobacterial DNA detected by PCR 6–12, interferon (IFN)-γ 12–17, lysozyme 15, 18, 19 and adenosine deaminase (ADA) 2, 12, 15, 19–24) can be useful in these diagnostic processes.
It has become clear in recent years that, as part of the immune response to infection by Mycobacterium tuberculosis, interleukin (IL)-12 increases macrophage activation by upregulating the production of IFN-γ by natural killer (NK) cells 25, 26. This raises the possibility that IL-12 or its subunits may also be of diagnostic value. The current authors report the results of a study in which the efficiency of IL-12 p40 in discriminating between TBPE and pleural effusions of neoplastic or parapneumonic origin was evaluated in comparison with the previously characterised parameters.
MATERIAL AND METHODS
The current authors prospectively studied, during a 24-month period, 146 patients who were admitted to the Pulmonology Service of the Complejo Hospitalario Clínico Universitario de Santiago (Santiago de Compostela, Spain) with what proved to be TBPEs (24 males, 15 females), neoplastic pleural effusions (NPPEs; 22 males, 20 females; table 1⇓) or parapneumonic pleural effusions (PPPEs; 12 males, 3 females) according to previous established criteria 15. The Review Board on Human Studies at the Complejo Hospitalario Clínico Universitario de Santiago approved the protocol. Informed consent was obtained from all patients.
Types or locations of tumours associated with the 42 neoplastic pleural effusions
Sample collection and analyses
Pleural fluid samples were taken by thoracocentesis at admission before initiation of any treatment. Total cell counts were determined with a Siemens ADVIA 2120 haematology system (Siemens, Madrid, Spain). IL-12 p40 was determined (in pg·mL−1) in 96 effusions (39 tuberculous, 42 neoplastic and 15 parapneumonic) using a sandwich ELISA from AMS Biotechnology (Abingdon, UK). ADA, expressed in U·L−1, was determined by the method of Giusti 27, isoform ADA-2 was determined by inhibition with erythro-9-(2-hydroxy-3-nonyl)adenine 28, IFN-γ was determined (in pg·mL−1) using an ELISA kit (Intertest-γ; Genzyme, Madrid), and CD3+/DR+ T-lymphocyte (CD3+/DR+ T) counts (in cells·mm−3) were determined as previously described 29, 30.
Statistical analysis
Kolmogorov–Smirnov tests were used to check distributional normality; non-normal distributions were subjected to log transforms. Groups were compared using a post hoc multiple comparison test (Bonferroni). The relative abilities of the various diagnostic parameters for pairwise discrimination between TBPEs and non-TBPEs were evaluated by comparing the areas under their receiver operating characteristics (ROCs) 31. The diagnostic performance of the various parameters, when used with the diagnostic thresholds afforded by the ROC analysis (see Results section), was evaluated in terms of sensitivity, specificity and positive and negative likelihood ratios (PLR and NLR, respectively). The PLR indicates how much more frequent positive test results occur in TBPEs, calculated as the proportion of positive test results in patients with TBPEs (sensitivity) divided by the proportion in non-TBPEs (1-specificity). The NLR indicates how much to decrease the probability of disease if the test is negative ((1-sensitivity)/specificity).
RESULTS
The distributions of the biochemical parameters in each group of pleural effusions are summarised in table 2⇓. For all these parameters, the median of the tuberculous group differed significantly from those of the neoplastic and parapneumonic groups in all cases, except comparison with PPPEs with regard to CD3+/DR+ T. The diagnostic thresholds afforded by the ROC analysis for IL-12 p40, ADA, ADA-2, IFN-γ and CD3+/DR+ T were 550 pg·mL−1, 54.3 U·L−1, 44.5 U·L−1, 169 pg·mL−1 and 80.3 cells·mm−3, respectively. However, the ROCs of the diagnostic parameters (fig. 1⇓) show that IL-12 separated TBPEs from NPPEs and PPPEs less well than ADA, ADA-2 and IFN-γ. The area under the IL-12 p40 ROC, 0.837, was significantly smaller than the areas of these other parameters. The area under the IL-12 p40 ROC did not differ significantly from the area under the CD3+/DR+ T ROC. The area under the ADA-2 ROC, 0.996, was significantly higher than the areas of the other parameters.

Receiver operating characteristics of the parameters studied, for diagnosis of tuberculous pleural effusion versus neoplastic or parapneumonic pleural effusion. –––: interleukin-12; ·····: adenosine deaminase (ADA); - - - -: ADA-2; – – – –: interferon-γ; ––··––··––: CD3+/DR+ T-lymphocytes.
Descriptive statistics of diagnostic parameters considered, for each type of pleural effusion
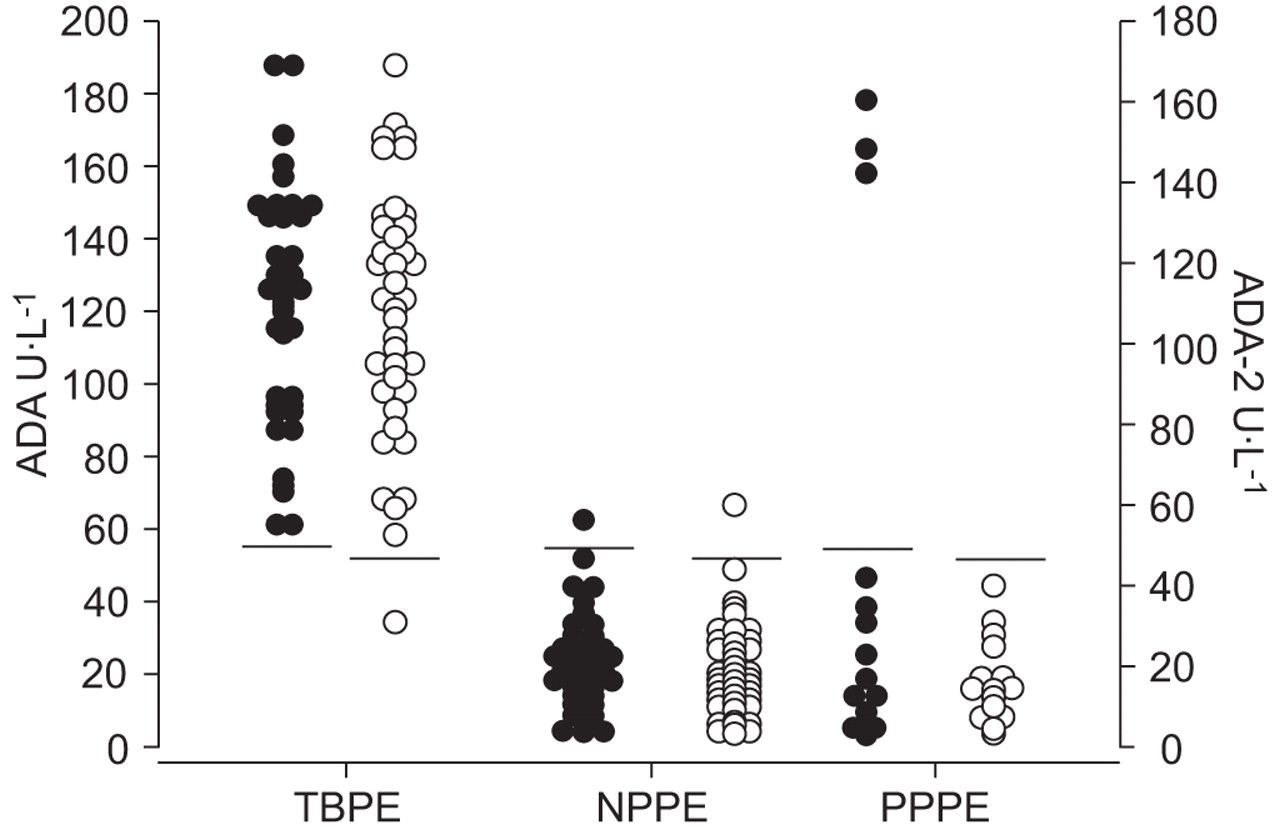
Figure 2⇓ shows the ADA and ADA-2 levels in each group of effusions. All TBPEs except one had values higher than the established diagnostic thresholds (54.3 U·L−1 for ADA and 44.5 U·L−1 for ADA-2). Sub-threshold levels of ADA and ADA-2 were found in 97.6% of NPPEs, while, among PPPEs, 80% had sub-threshold levels of ADA and 100% had sub-threshold levels of ADA-2. Figure 3⇓ shows IL-12 and IFN-γ levels in each group of effusions. IL-12 p40 was above the threshold (550 pg·mL−1) in 92.3% of TBPEs, 35.7% of NPPEs and 13.3% of PPPEs. IFN-γ was above the threshold (169 pg·mL−1) in 82.1% of TBPEs, 7.1% of NPPEs and 6.7%% of PPPEs. CD3+/DR+ T was above the threshold (80.3 cells·mm−3) in 82.1% of TBPEs, 31% of NPPEs and 46.6% of PPPEs.

Adenosine deaminase (ADA; •) and ADA-2 (○) levels in the pleural fluid of the three groups of patients studied (cut-off points of 54.3 and 44.5 U·L−1, respectively). TBPE: tuberculous pleural effusion; NPPE: neoplastic pleural effusion; PPPE: parapneumonic pleural effusion.

{kind=link}
{kind=link}
{kind=link}
Interleukin (IL)-12 p40 (•) and interferon (IFN)-γ (○) levels in the pleural fluid of the three groups of patients studied (cut-off points of 550 and 169 pg·mL−1, respectively). TBPE: tuberculous pleural effusion; NPPE: neoplastic pleural effusion; PPPE: parapneumonic pleural effusion.
Table 3⇓ lists the numbers of misclassifications by each parameter and group. From worst to best, CD3+/DR+ T misclassified 28.1% of effusions, IL-12 20.8%, IFN-γ 11.5%, ADA 5.2% and ADA-2 2.1%. The misclassification rates of ADA and ADA-2 did not differ significantly. The misclassification rate of ADA-2 was significantly lower than those of IFN-γ, IL-12 p40 and CD3+/DR+ T. The misclassification rate of IL-12 p40 did not differ significantly from that of CD3+/DR+ T and IFN-γ, but was significantly greater than those of ADA and ADA-2.
Numbers of misclassified effusions of each group, for each diagnostic parameter studied
Table 4⇓ lists other performance parameters, emphasising that IL-12 p40 had a sensitivity of 92.3%, a specificity of 70.2%, a PLR of 3.10 and an NLR of 0.11. Between the studied parameters, no significant differences were found with respect to the sensitivity. The specificity of IL-12 p40 was significantly lower than ADA, ADA-2 and IFN-γ, while ADA-2 showed no significant differences with respect to ADA and IFN-γ. Table 5⇓ lists correlations among the various parameters in the TBPE group.
Performance measures for diagnosis of tuberculous pleural effusions by each diagnostic parameter with the stated thresholds
Coefficients of correlation between the parameters studied in the tuberculous pleural effusion group
DISCUSSION
The results of the present study appear to confirm that IL-12 p40 levels in the TBPEs are significantly higher than in the NPPEs and the PPPEs, but are less efficient than the established markers ADA, ADA-2 and IFN-γ.
IL-12 is a cytokine composed of two polypeptide subunits, p40 and p35, that are encoded by distinct genes and are linked covalently by disulphide bridges in the active heterodimer, p70. IL-12 stimulates the production of IFN-γ by NK cells, and thereby indirectly promotes the activation of macrophages. It is, therefore, believed to play an important role in the immune response to intracellular pathogens such as M. tuberculosis. Previous studies have in fact found, like the present study, that IL-12 p40 levels are significantly higher in TBPEs than in NPPEs and other pleural effusions 32–36, and have reported areas under the IL-12 p40 ROC similar to the 0.837 observed in the current study 33; but this value is significantly less than the areas under the ROCs of IFN-γ, ADA and ADA-2.
The current results confirm that most TBPEs are identifiable by their high IL-12 p40 levels (sensitivity 92.3%), but their specificity is poor (70.2%). In a previous study using a diagnostic threshold of 560 pg·mL−1, a similar sensitivity but a higher specificity (85.4%) was found 34, the difference probably being mainly due to this previous study having included transudates, which only rarely have IL-12 p40 levels above the threshold. The current authors believe that the specificity obtained when excluding transudates from the study is the more relevant result for clinical practice, because the aetiological diagnosis of transudates is generally unproblematic; it is to distinguish among TBPEs, NPPEs and PPPEs that tests are needed. The overall misclassification rate of IL-12 p40 in the present study was 20.8%, a figure that is significantly larger than the misclassification rates of ADA (5.2%) and ADA-2 (2.1%).
Other studies have reported IL-12 p40 to have a specificity of 96.9% and a PLR of 17.45 but less sensitivity (54.5%) 35. The immediate cause of the wide discrepancy between these values and those of the current study is the previous study having used a diagnostic threshold more than twice as high (1,296 pg·mL−1) as that of the current study. That this was the optimal threshold for their sample is in turn probably attributable mainly to that sample having included no PPPEs and three times as many NPPEs as TBPEs, an aetiological distribution very different from that of the current study, as well the small size of their sample (43 effusions) and a different method to determine IL-12 p40.
The yield of the rest of the parameters was similar to previous studies 37. Although the overall misclassification rate of ADA-2 (2.1%) did not differ significantly from that of ADA (5.2%), it did have a significantly larger area under its ROC.
IFN-γ was positively correlated with IL-12 p40, in keeping with current accounts of the role of IL-12 in inducing IFN-γ production during infection by M. tuberculosis. As expected, ADA-2 was closely correlated with ADA among TBPEs.
In conclusion, the observed elevation of interleukin-12 p40 levels in tuberculous pleural effusions is consistent with interleukin-12 playing a role in the immune response to infection by Mycobacterium tuberculosis. The correlation between interleukin-12 p40 and interferon-γ in these effusions is in line with current knowledge about the relationship between them. However, interleukin-12 p40 is less efficient in this role than adenosine deaminase, adenosine deaminase isoform 2 or interferon-γ, and its routine determination is, accordingly, not recommended.
Statement of interest
None declared.
- Received June 5, 2008.
- Accepted November 10, 2008.
- © ERS Journals Ltd
References










