





Abstract
The aim of the present study was to examine the natural evolution of primary snoring and obstructive sleep apnoea (OSA) in adult male patients.
Retrospective analysis was performed on 160 untreated patients with primary snoring and mild, moderate and severe OSA who had two polysomnographic recordings. The mean time between recordings (TBR) was 5.1±3 yrs.
The mean apnoea/hypopnoea index (AHI), body mass index (BMI), and lowest arterial oxygen saturation level during rapid eye movement (REM) and non-REM sleep showed a significant worsening effect. The change in AHI differed among the groups showing a similar significant increase in AHI for primary snoring, mild and moderate OSA and an insignificant decrease for severe OSA patients. Stepwise linear regression showed that only ΔBMI and time were significant predictors for AHI change. A model for the mean AHI change showed that ΔAHI = (4.33×ΔBMI) + (0.66×TBR). After adjusting for confounders, multiple regression analysis indicated that age and high BMI, but not AHI, were significant risk factors for developing hypertension and/or cardiovascular disease.
Patients with primary snoring and mild and moderate obstructive sleep apnoea had a similar increase in the apnoea/hypopnoea index over time, which depended mainly on weight gain and, to a lesser extent, on time.
- Apnoea/hypopnoea index
- body mass index
- natural evolution of disease
- obstructive sleep apnoea
- polysomnography
- snoring
The study by Lugaresi et al. 1 was the first to theorise that prolonged snoring for years, and even decades, antedated the appearance of overt obstructive sleep apnoea (OSA). However, owing to the sparse and conflicting data available to date, controversy arises as to whether OSA is a progressive disease. In total, 18 longitudinal studies have dealt with the evolution and risk factors associated with snoring and OSA syndrome 2–19. Several studies found that mild-to-moderate OSA has a tendency to worsen over time 2–11. Other clinical trials found that apnoea status is fairly stable over time 12, 14–19 or even improves 13. Of these 18 studies, nine include subjects from the general population and four of them comprise a large number of participants (between 282 and 2,968 subjects) and are relatively new studies. The other five are much older studies, include fewer participants and mostly comprise an elderly population. Of these 18 studies, nine assessed patients seeking treatment, but most of them are relatively old studies including a small number of participants (between 11 and 55), which did not allow meaningful subgroup comparisons. All but one study included both sexes 6. In some studies the time between the two polysomnographic (PSG) evaluations was relatively short 4, 5 or analysis was restricted to an older population (table 1⇓) 3, 12, 14, 16, 18.
Primary snoring and obstructive sleep apnoea: progressive or stable
The answer to the question of how to approach snoring and OSA has more than academic interest. A progressive nature of disease would dictate early and frequent follow-up visits for patients with primary snoring and mild OSA and treatment planning at an early stage 20; however, the opposite would hold true for a stable disease.
The present authors followed up 160 untreated adult males over a mean period of 5 yrs, aiming to study the natural evolution of snoring and OSA in primary snorers and in patients with mild, moderate and severe OSA. The risk factors that may play a role in the progression of these conditions was investigated.
MATERIALS AND METHODS
Patient selection
A retrospective, longitudinal case study of untreated adult males who had primary snoring and various degrees of OSA were followed at the Sleep Disorders Unit (Loewenstein Hospital Rehabilitation Center, Raanana, Israel), between 1989 and 2004. Only patients who had two overnight PSG for ≥4 h sleep each on separate occasions, ≥6 months apart were included. Patients using either continuous positive airway pressure (CPAP), bi-level positive airway pressure, an oral appliance or tennis ball technique and those who had nasal, oropharyngeal or bariatric surgery between recordings were excluded from the analysis. In addition, patients who had split-night examinations and patients with predominant central apnoeas, neuromuscular disorders or who were mentally retarded were excluded. After the exclusion criteria were applied, 160 patients were left and comprised the research group.
Each patient completed a questionnaire for demographics, sleep habits and symptoms, and general medical condition data. Further data on years of snoring, smoking habits and concomitant diseases including hypertension (HT) and cardiovascular disease (CVD) were collected. Following initial PSG recordings, all patients were advised, when appropriate, to reduce weight and/or use CPAP, an oral device, or tennis ball technique, but either refused or had poor compliance. The request for a second PSG came from the referral physician who decided to ask for a re-evaluation based on the patient’s symptoms. The patients were not paid to undergo the second examination. The patients belong to the Clalit Health Care Services (Tel Aviv, Israel) which is the largest Health Maintenance Organization in Israel, providing medical services to ∼60% of the total Israeli population. Polysomnography is included in the medical services free of charge.
The study was approved by the local Institutional Review Board of the Sleep Disorders Unit (Loewenstein Hospital Rehabilitation Center).
Objective and subjective measurements
Complete PSG recordings were performed overnight. The recordings were performed using either Nihon Kohden polygraphs (models 4321 and 4414; Nihon Kohden, Tokyo, Japan) or the Rembrandt Manager System (Medcare, Amsterdam, the Netherlands) and included conventional parameters 21. The recordings were scored according to the standard criteria of Rechtschaffen and Kales 22. Apnoea was defined as an episode of complete breathing cessation of ≥10 s. Hypopnoea was defined as a reduction of >30% in oral/nasal airflow (oral/nasal thermistor) lasting ≥10 s, accompanied by arousal or by a decrease of ≥3% in arterial oxygen saturation (Sa,O2). Pressure cannulas were not used during the study period. Snoring sounds were recorded by a microphone located above the patient’s head at a distance of 1 m and connected to a sound level meter (SLM; model 2700; Quest Electronics, Oconomowoc, WI, USA). The study procedure used the dB A scale (A: weighting network that yields the response of the human ear), the 40–100 dB range and the fast response mode. This was a calibrated channel (40–80 dB) of the PSG in order to evaluate the intensity of each snore event. The output from the SLM was also recorded in parallel on a calibrated (40–80 dB) chart recorder at a paper speed of 10 cm·h−1. Subjective daytime sleepiness was assessed by using the Epworth Sleepiness Scale (ESS) 23.
Study definitions
The patients were stratified by apnoea/hypopnoea index (AHI) severity to primary snoring (AHI <5) and mild (AHI 5–15), moderate (AHI 15–30) and severe OSA (AHI >30). The snoring history was divided into four periods: <5 yrs, 5–10 yrs, 10–20 yrs and >20 yrs. An ESS score of >10 was considered as abnormal daytime sleepiness. Improvement or worsening of initial AHI was defined as an increase or decrease of ≥25% of AHI 5 after assuring that there were ≥10 events·h−1. A patient was defined as a nonsmoker if there was no history of cigarette smoking or smoking was stopped for ≥5 yrs.
Statistical analysis
As the Shapiro–Wilk test demonstrated that some of the parameters were not normally distributed, the nonparametric Wilcoxon signed rank test was used to compare the mean baseline (time 1; T1) AHI, body mass index (BMI; kg·m−2), ESS score (0–24), lowest Sa,O2during rapid eye movement (REM) and non-REM sleep, and maximum snoring sound levels (dB) in supine and lateral body positions with that of end of follow-up (time 2; T2). The nonparametric Kruskall–Wallis test was used to examine differences over time of the four AHI severity groups for a given demographic or sleep parameter (Δ indicates difference between T1 and T2). Stepwise linear regression was used to examine the correlations between ΔAHI as the dependent variable against ΔBMI, time between recordings (TBR), age, HT and/or CVD, and lowest Sa,O2levels during REM and non-REM sleep. Stepwise logistic regression analysis determined the independent risk factors for HT and/or CVD. Only variables that were significant were entered into the final multiple logistic regression model.
RESULTS
In total, 160 untreated adult males (mean age 51±11 yrs) underwent full PSG recordings on two occasions (mean TBR 5.1±3 yrs; median (range) 5 (0.5–15) yrs). The mean sleep efficiency was 85.6±8.9% for the first PSG and 85.5±8.1% for the follow-up evaluation.
Table 2⇓ shows the values of age, AHI, BMI, ESS, lowest Sa,O2in REM and non-REM sleep, and maximum snoring sound levels (dB) in supine and lateral body positions for T1 and T2. The significant increase in age is obvious. The Wilcoxon signed rank test shows a significant increase for AHI and BMI levels, and a significant decrease (worsening) in lowest Sa,O2in REM and non-REM sleep. There was also a significant increase in ESS score from T1 to T2. The snoring intensity in the supine body position did not change significantly; however, in the lateral position a significant increase was observed.
Demographic and sleep parameters data at baseline(T1) and at the end of the follow-up period (T2)
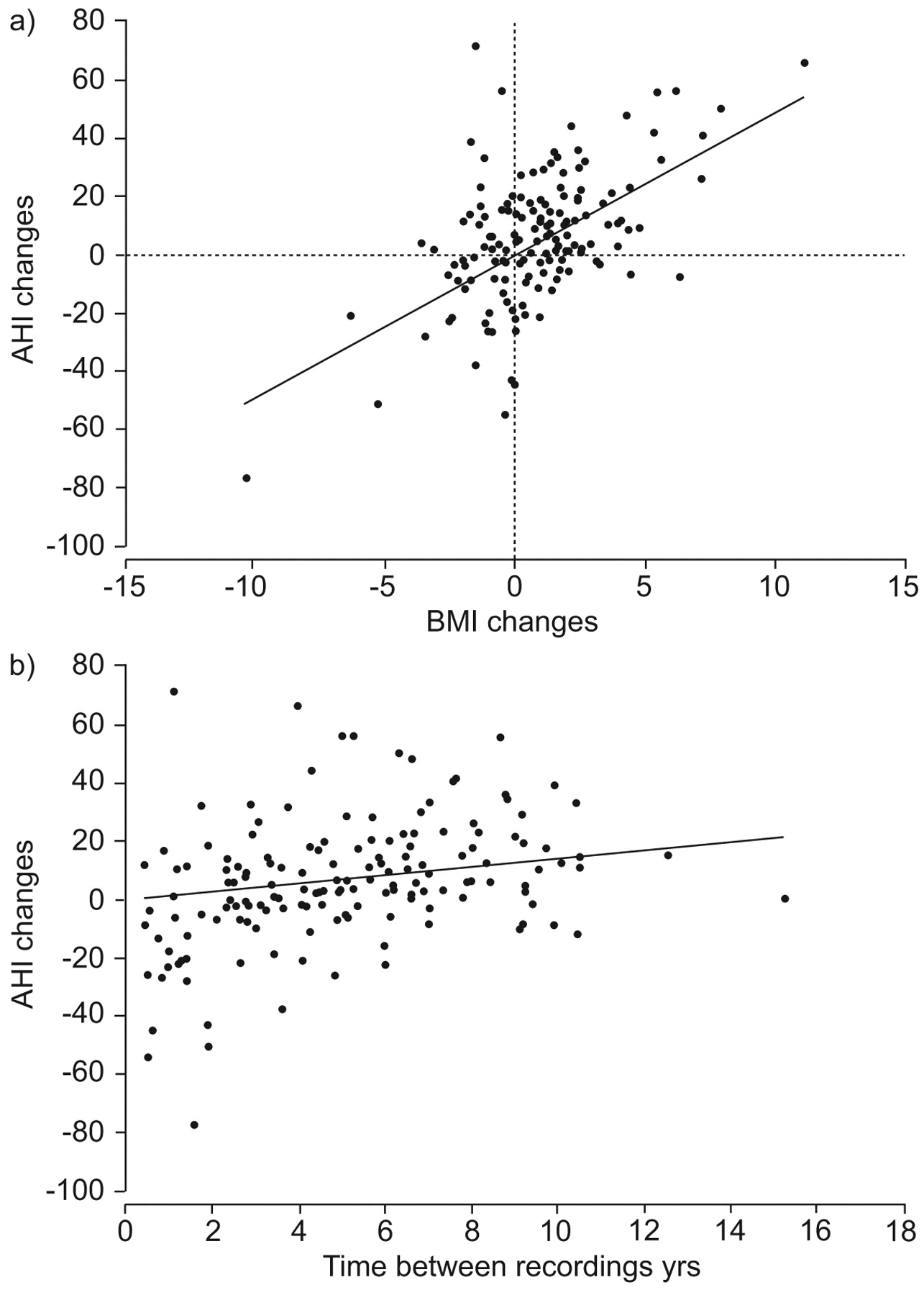
Primary snoring was diagnosed in 26 (16.3%) patients, mild OSA in 47 (29.4%), moderate OSA in 41 (25.6%), and severe OSA in 40 (25%) patients. The TBR was significantly different across these patient groups (6.2±2.6, 5.4±3.0, 4.9±3.0 and 4.3±3.1 yrs, respectively; p = 0.044). The ΔAHI differed significantly among the groups, showing two patterns (a significant increase for primary snoring, mild OSA and moderate OSA and an insignificant decrease for severe OSA; fig. 1⇓). The difference for ΔBMI was also significant among the groups (p = 0.011). While primary snoring and mild OSA patients had a significant worsening in BMI, moderate and severe OSA patients did not show significant increases in BMI (table 3⇓). The lowest Sa,O2 level in REM and non-REM sleep showed significant differences among the groups but no significant interaction with time was observed. A significant deterioration was observed for the lowest Sa,O2 level in REM sleep for patients with mild OSA and for the lowest Sa,O2 level in non-REM sleep for primary snorers and mild OSA patients. As for ΔAHI, patients with severe OSA showed an insignificant change in Sa,O2 for both REM sleep and non-REM sleep (table 3⇓). Although moderate OSA patients showed a significant increase in ESS score, the change in ESS score was not statistically significant across groups or across time. The significant correlations between ΔAHI and ΔBMI (r2 linear = 0.296) and ΔAHI and TBR (r2 linear = 0.082) are displayed in figure 2⇓.

The changes in apnoea/hypopnoea index (AHI) over time in 160 untreated patients (mean interval between time 1 and time 2 was 5.1±3 yrs) divided into four groups according to diagnosis at time 1. Primary snoring (·······; AHI <5), mild obstructive sleep apnoea (- - - -; AHI 5–15) and moderate obstructive sleep apnoea (– – –; AHI 15–30) patients had a similar significant increase in AHI, while severe obstructive sleep apnoea patients (––––; AHI >30) showed an insignificant decrease in AHI. Data are presented as mean±se.
{kind=link}
{kind=link}
a) The relationship between the change in apnoea/hypopnoea index (AHI) and the change in body mass index (BMI) for the 160 untreated patients who had two complete polysomnographic evaluations during a mean period of ∼5 yrs. y = 4.9307x; r2 = 0.258; p <0.001. b) The relationship between the change in AHI and time between recordings for the 160 untreated patients who had two complete polysomnographic evaluations during a mean period of ∼5 yrs. y = 1.4368x; r2 = 0.0815; p<0.001.
Change in sleep parameters over time for the four patient groups at baseline(T1) and at the end of the follow-up period (T2)
Stepwise linear regression analysis showed that ΔBMI and TBR were significant predictors for AHI change (95% confidence interval (CI) 2.72–4.92, p<0.001; 95% CI 0.6–2.66, p = 0.002, respectively; r2 = 0.331), whereas baseline age, BMI, HT and/or CVD, and lowest Sa,O2in REM and non-REM sleep were not. Adjusting for these confounding factors, a model for the mean ΔAHI showed that: ΔAHI = (4.33×ΔBMI) + (0.66×TBR); r2 = 0.322.
A cut-off point of 25% 8 was used to define improvement or worsening of initial AHI (table 4⇓). In total, 23 (14.4%) patients improved their initial AHI score, 74 (46.2%) remained stable and 63 (39.4%) patients worsened. No significant differences were found between these three groups in terms of age and BMI. Patients who showed a worsening effect had a significantly lower AHI at T1 and patients who improved had a significantly higher AHI at T1.
Age, body mass index(BMI) and apnoea/hypopnoea index (AHI) of patients who improved, did not change, or worsened between baseline (T1) and follow-up (T2)
Table 5⇓ shows that the incidence of HT and/or CVD increased from 54 (33.8%) patients at T1 to 65 (40.6%) patients at T2. Table 5⇓ also shows that 11 (10.4%) out of 106 patients who had no HT at T1 developed this complication during T2. In nine (81.8%) patients, there was an increase in BMI and AHI at T2 (data not shown).
Number of patients with hypertension(HT) and cardiovascular disease (CVD) at baseline (T1) and end of follow-up (T2)
Analysis by age, BMI, AHI at T2, duration of snoring, and smoking habits as independent risk factors for HT and/or CVD showed that age, BMI and AHI were positively associated with HT and/or CVD (60.4±11.6 versus 52.8±10.2, p = 0.017; 31.0±4.7 versus 29.2±4.6, p = 0.026; and 31.8±22.7 versus 25.7±23.8, p = 0.038; respectively), whereas duration of snoring (p = 0.094) and smoking habits (p = 0.395) were not. Using the significant variables identified and adjusting for confounding factors, multiple regression analysis indicated that only age and higher levels of BMI remained significant risk factors for developing HT and/or CVD (table 6⇓).
Risk factors for developing hypertension(HT) and/or cardiovascular disease (CVD)
DISCUSSION
The main finding of the present study is that the outcome of untreated primary snorers and OSA patients in the adult male study population is dependent mainly on weight increase and, to a lesser degree, on time. Of these two factors, weight increase exceeds the latter by almost seven-fold, having a major role in AHI progression. Age, HT and lowest Sa,O2in REM and non-REM sleep were not significant predictors for AHI progression.
Provided that ΔBMI and TBR are known, the current authors’ model for calculating ΔAHI, (4.33 ×ΔBMI) + (0.66×TBR), may serve as a useful tool in sleep healthcare medicine for male patients aged ∼50 yrs, who are the vast majority of male patients seeking treatment for snoring and OSA at the sleep disorder units. It may be deduced from the model that with a stable body weight, it takes ≥6 yrs before the impact of TBR on ΔAHI perhaps becomes apparent (increased in four units in ΔAHI). However, increasing weight in one BMI unit during 1 yr, the AHI will increase in five units. Previous studies have also shown the role of time in disease progression in the absence of concomitant weight increase 5, 24, and for some cases it is possible that AHI could be a risk factor for an increase in the BMI.
The number of patients included in the present study exceeds that of all previous studies available to date on the natural evolution of primary snoring and OSA for patients seeking treatment (table 1⇑), allowing the present authors to establish a more meaningful statistical analysis for the four subsets of disease severity.
A significant increase in AHI and BMI over time was shown in the 160 males with primary snoring and various degrees of OSA. Nevertheless, while snorers and those with mild and moderate OSA had an increase in AHI that correlated with the increase in BMI, patients with severe OSA had a nonsignificant decrease in AHI suggesting a ceiling effect for OSA severity.
The correlation between ΔAHI and ΔBMI is demonstrated in several studies of patients seeking treatment. In patients aged >70 yrs, Ancoli-Israel et al. 18 showed that changes in AHI were associated with changes in BMI and, similarly to the present findings, this was independent of age. Furthermore, Sforza et al. 15 did not observe significant changes in apnoea frequency or nocturnal hypoxaemia in untreated OSA patients in the absence of changes in BMI. Likewise, no AHI changes were detected in untreated OSA patients who remained stable in weight, but those who reduced their weight had a significant decrease in AHI severity 15.
Similar to previous studies 5–7, using a cut-off point of 25% for defining improvement or worsening of initial AHI 5, the current authors showed no significant differences in the age of patients who improved, remained stable or deteriorated (p = 0.478). Another study found a tendency for younger patients to deteriorate 15.
The association between sleep-disordered breathing and HT is well established 25. In total, 42 (26.9%) of the study patients were initially diagnosed with HT. During the follow-up period, 10.4% of normotensive patients developed this complication, demonstrating a more than two-fold increase in the incidence of HT than the expected incidence of newly diagnosed HT in the general population over a similar period 26. Similar to a previous study 27, the current authors found that age and high levels of BMI were significant predictors of HT and/or CVD while the progression in AHI itself was not the main factor in the development of CVD. Certainly, other cardiovascular risk factors not assessed in the present study, such as dyslipidaemia, insulin resistance or endothelial dysfunction, may have also participated in the development of cardiovascular morbidity.
The present study has several limitations. A retrospective design is of one the known limitations of studies covering the natural history of snoring and OSA. However, it allowed a better insight into the long-term trends of this syndrome in a relatively large group of untreated patients who had at least two PSG evaluations. A second limitation is that the patients consisted of a seek-treatment group and, regardless of the mode of referral, they were assessed mainly because their sleep symptoms and/or daytime somnolence either continued or worsened. This may have induced a selection bias, as patients with severe or progressive symptoms are more eager to be re-examined. Nevertheless, it may have been balanced by the fact that most of the severe OSA patients are being successfully treated with CPAP, underwent surgery or use other devices and were all excluded from the analysis. Moreover, in the current study population, there were a similar number of patients with mild, moderate and severe OSA that had two PSG evaluations.
Using a cut-off point of 25% for defining improvement or worsening of initial AHI, although used in a previous study 5, is arbitrary and could be affected by the night-to-night AHI variability. In addition, since mild-to-moderate OSA patients are mainly influenced by the sleep posture, it is possible that part of the increase in AHI severity is related to an increase in time spent in the supine posture in the second PSG 21. However, since only a significant increase in lateral AHI (19.4±19.6 versus 28.9±25.7; p<0.01) was seen, without a significant change in supine AHI (58.8±32.4 versus 59.4±27.4) from T1 to T2, this does not appear to be the case.
Unfortunately, the current authors did not quantify the various reasons for seeking a repeated PSG evaluation in the study patients, which could have provided valuable clinical information. However, based on clinical experience, the main two reasons for a re-evaluation were a suspected worsening of snoring and/or OSA and a subjective worsening in daytime sleepiness. In some cases, the trigger for a re-evaluation came after reading a related article in a newspaper or magazine, after watching or listening to a television or radio programme, or after the recommendations of a friend using CPAP successfully.
How do these data compare to data obtained from the general population? The crucial role of weight gain on the progression of snoring and OSA shown in the present study in seeking-treatment patients is very similar to most of the previous studies that have investigated the evolution of snoring and OSA in the general population. Population studies of the Wisconsin Sleep Cohort 7, the Cleveland Family Study 9 or from the Sleep Heart Health Study 10 all found that weight gain is a crucial predictor of longitudinal changes in the incidence and severity of sleep-disordered breathing. Although this association between increase in weight and the worsening in sleep-disordered breathing has modifications according to sex, age, race and ethnicity, it is clear that excess weight is a critical contributor to the incidence and progression of this sleep related breathing disorder. Thus, the results of the largest untreated clinical population of seeking-treatment patients suffering from snoring and OSA agree completely with the results of the largest population study 10, and support the notion that avoiding weight gain for the prevention of and encouraging weight loss for the treatment of this clinical entity are imperative purposes for public health.
In summary, in a follow-up study of 160 untreated snorers and obstructive sleep apnoea adult male patients over a mean period of 5 yrs, it was found that patients with primary snoring and mild and moderate obstructive sleep apnoea had a similar significant increase in apnoea/hypopnoea index over time. However, patients with severe obstructive sleep apnoea had an insignificant change in apnoea/hypopnoea index suggesting a ceiling effect. The progression in apnoea/hypopnoea index is mainly dependent on weight gain and, to a lesser degree, on time. Of these two factors, weight increase exceeds the latter by almost seven-fold, having a major role in apnoea/hypopnoea index progression. Provided that change in body mass index and time between recordings are known, the current authors model for calculating change in apnoea/hypopnoea index may represent a useful tool in sleep healthcare medicine for male patients aged ∼50 yrs, who are the vast majority of male patients seeking treatment for snoring and obstructive sleep apnoea.
Statement of interest
None declared.
- Received January 28, 2008.
- Accepted October 14, 2008.
- © ERS Journals Ltd
References










