





Abstract
Asthma is a highly prevalent condition across Europe and numerous guidelines have been developed to optimise management. However, asthma can be neither cured nor prevented, treatment choices are limited and many patients have poorly controlled or uncontrolled asthma.
The Brussels Declaration on Asthma, sponsored by The Asthma, Allergy and Inflammation Research Charity, was developed to call attention to the shortfalls in asthma management and to urge European policy makers to recognise that asthma is a public health problem that should be a political priority.
The Declaration urges recognition and action on the following points: the systemic inflammatory component of asthma should be better understood and considered in assessments of treatment efficacy; current research must be communicated and responded to quickly; the European Medicines Agency guidance note on asthma should be updated; “real world” studies should be funded and results used to inform guidelines; variations in care across Europe should be addressed; people with asthma should participate in their own care; the impact of environmental factors should be understood; and targets should be set for improvement.
The present paper reviews the evidence supporting the need for change in asthma management and summarises the ten key points contained in the Brussels Declaration.
The prevalence of asthma has increased dramatically over the last 20 yrs 1 and ∼180,000 deaths annually are attributable to asthma worldwide. The disease has become particularly common in industrialised countries, where it has become the most common chronic disease among children 2. As a result of the high prevalence and ongoing changes to treatment guidelines, it has been difficult to make an accurate estimate of the current cost of asthma. In Europe, the annual cost was estimated at \#8364;17.7 billion in 2003 (\#8364;9.8 billion in lost productivity and \#8364;7.9 billion in direct medical costs) 3.
The increase in asthma prevalence over recent decades has been accompanied by an increase in atopic sensitisation and allergic conditions such as rhinitis and sinusitis, suggesting that there may be a systemic component to the inflammation associated with asthma 4–6. Despite the increasing evidence of the systemic inflammation model and the emerging data suggesting a role for inflammation in structural remodelling of the airways 7, 8, many patients remain reliant on medications that relieve symptoms or treat inflammation only within the lower airways 9, 10. The root causes of the inflammation associated with asthma have not been clarified and consequently its development cannot be prevented.
Although a great deal of work has been done to improve the understanding of asthma, knowledge in many areas remains suboptimal. Diagnosis can be difficult due to the number of different diseases with similar presentations and because there is no single measure or instrument that can provide definitive proof that asthma is present 11. Once the diagnosis is in place, many patients are inadequately informed and educated about the treatment goals and many fail to achieve asthma control 12, 13. In addition, currently available asthma medications that can help patients achieve control are being used suboptimally. Children represent a particular problem because few clinical trials address the efficacy and safety of asthma treatment in paediatric patients and the disease course in children is not well understood 14. As yet, asthma can neither be cured nor prevented and research is urgently needed to meet the considerable challenges that remain.
While discussing these shortfalls in asthma management at an asthma policy roundtable meeting at the European Parliament in January 2006, participants recommended holding a summit meeting 15 to make policy makers at the European level aware of the need for change in asthma management. The Brussels Declaration on Asthma, which was developed at the Summit and was sponsored by the Asthma, Allergy and Inflammation Research Charity, identifies these changes and urges European politicians, physicians, researchers and asthma patients to reach agreement on practical clinical and regulatory strategies that recognise current gaps in care, and recommend a wider range of treatment options (table 1⇓).
Ten key points established in the Brussels Declaration from the European Summit for Change in Asthma Management
The present paper reviews the evidence supporting changes in asthma management and provides a summary of the key points in the Brussels Declaration.
DIAGNOSTIC ISSUES
Before an asthma management plan can be recommended, patients must first be correctly diagnosed. Recent guidelines from the Global Initiative for Asthma (GINA), the US National Asthma Education and Prevention Program's Expert Panel 16, 17, and the British Thoracic Society (BTS)/Scottish Intercollegiate Guidelines Network (SIGN) guidelines 18 recommend assessment of symptoms and measurement of lung function 1. However, there is a poor relationship between the symptoms experienced by patients and objective lung function 19, and asthma is often misdiagnosed 20. In addition, lung function tests can be insensitive 21, 22 and are especially difficult to perform reliably in children 23. Thus, while lung function testing in asthma diagnosis is of great value, over-reliance on this as a diagnostic test can be misleading and may fail to provide adequate insight into the impact of asthma on daily living. Other tests, including methacholine challenge and sputum eosinophil counting, have been shown to be useful for discriminating between asthma and other diseases commonly confused with asthma, but it is not always appropriate to perform these tests 22, 24. Consequently, symptoms have become the key factor for asthma diagnosis, despite the fact that they tend to be nonspecific and are shared by a number of other diseases.
There is also evidence of a lack of diagnostic rigour in primary care. A study in general practices in the UK reported that 56% of children and 45% of adults received some form of asthma treatment before a diagnosis was in place 25. In addition, results of lung function tests were recorded in <20% of people diagnosed with asthma, and the proportion was even lower in those who were immediately prescribed anti-asthma medications. There is also evidence that there is too much delay before the asthma diagnosis is finally made 26. Delays of ∼18 months in children and 5 yrs in adults have been reported 27.
INFLAMMATION: A KEY PATHOLOGY IN ASTHMA
In the past, asthma was considered to be a simple disease involving reversible airflow obstruction that could be treated with bronchodilators. It is now clear that the disease is considerably more complex, involving multiple inflammatory cascades and infiltration of inflammatory cells, often eosinophilic, into the airways 7. For example, on exposure to an inhaled allergen, an early phase reaction occurs characterised by rapid activation of mast cells and macrophages in the airways, which leads to contraction of bronchial smooth muscle, mucus secretion, narrowing of the airway lumen and airflow obstruction. This is followed by a late-phase reaction, which involves the release of pro-inflammatory mediators, recruitment of inflammatory cells into the airways and enhancement of bronchial hyperresponsiveness, and then further cycles of cell influx and mediator secretion 28. Further complexity occurs with other environmental exposures, such as with respiratory viruses and air pollutants 29.
The inflammatory changes associated with asthma do not appear to be confined to the lower airways. Asthma and allergic rhinitis affect the same tissues, involve common inflammatory mechanisms, cells and mediators and are frequently found together 4, 30, particularly in patients with allergic asthma 31. Since rhinitis often precedes the onset of asthma 32, it may be an early manifestation of an inflammatory process within a continuous airway 33 and extends beyond atopic disease 34. This link has also been demonstrated with the finding that eosinophilic inflammation is produced in the upper and lower airways after provocation of rhinitis patients with nasal allergens and following provocation of the lower airway by bronchial segmental allergen challenge 35. There is also mounting evidence that the inflammatory mediators from the airways are distributed systemically, resulting in far-reaching inflammatory effects in the skin, bone marrow and intestines 5. As a result, a new appreciation of asthma as a respiratory manifestation of systemic inflammatory processes is emerging 6.
In the long-term, inflammatory changes in the airways may lead to structural remodelling, which includes thickening of the airway wall caused by increased smooth muscle and mucus gland mass, thickening of basement membrane and increased production of connective tissue components 36. Remodelling may also be intrinsic to the origins of asthma, with a complex interplay occurring between structural, immune and inflammatory cells 8, 29. Although the severity of asthma is to some extent related to the degree of airway remodelling, the specific elements of these changes that contribute to the physical manifestations of asthma are not entirely clear. Some of these changes have been documented in patients even in the absence of overt symptoms 7, underlining the need for more robust tools for diagnosing and monitoring asthma 37.
Although inflammation can be treated with inhaled corticosteroids 38 or leukotriene receptor antagonists 39, it is still not clear why inflammation develops in the first place, why it interacts with smooth muscle to cause bronchospasm, or why it may escalate to produce structural remodelling in the airways. Recent reviews suggest that evidence that any current treatment can prevent or reduce airway remodelling is conflicting at best 9, 40, and there is an urgent need for research in this area. A better understanding of the root cause of inflammation should lead to the development of both curative treatments and effective prevention strategies.
UNDERSTANDING THE CAUSES OF POOR ASTHMA CONTROL
National and international asthma guidelines have set specific asthma treatment goals for clinicians and patients. Although the goals differ slightly between the various guidelines, the common aim is for patients to achieve and maintain control of their asthma. The most recent GINA guidelines state that to have asthma control, a patient must: 1) have symptoms only twice or less per week; 2) have no limitation of their daily activities; 3) use reliever medication twice or less per week; 4) have normal lung function; and 5) have no exacerbations (table 2⇓) 1.
Asthma control according to Global Initiative for Asthma
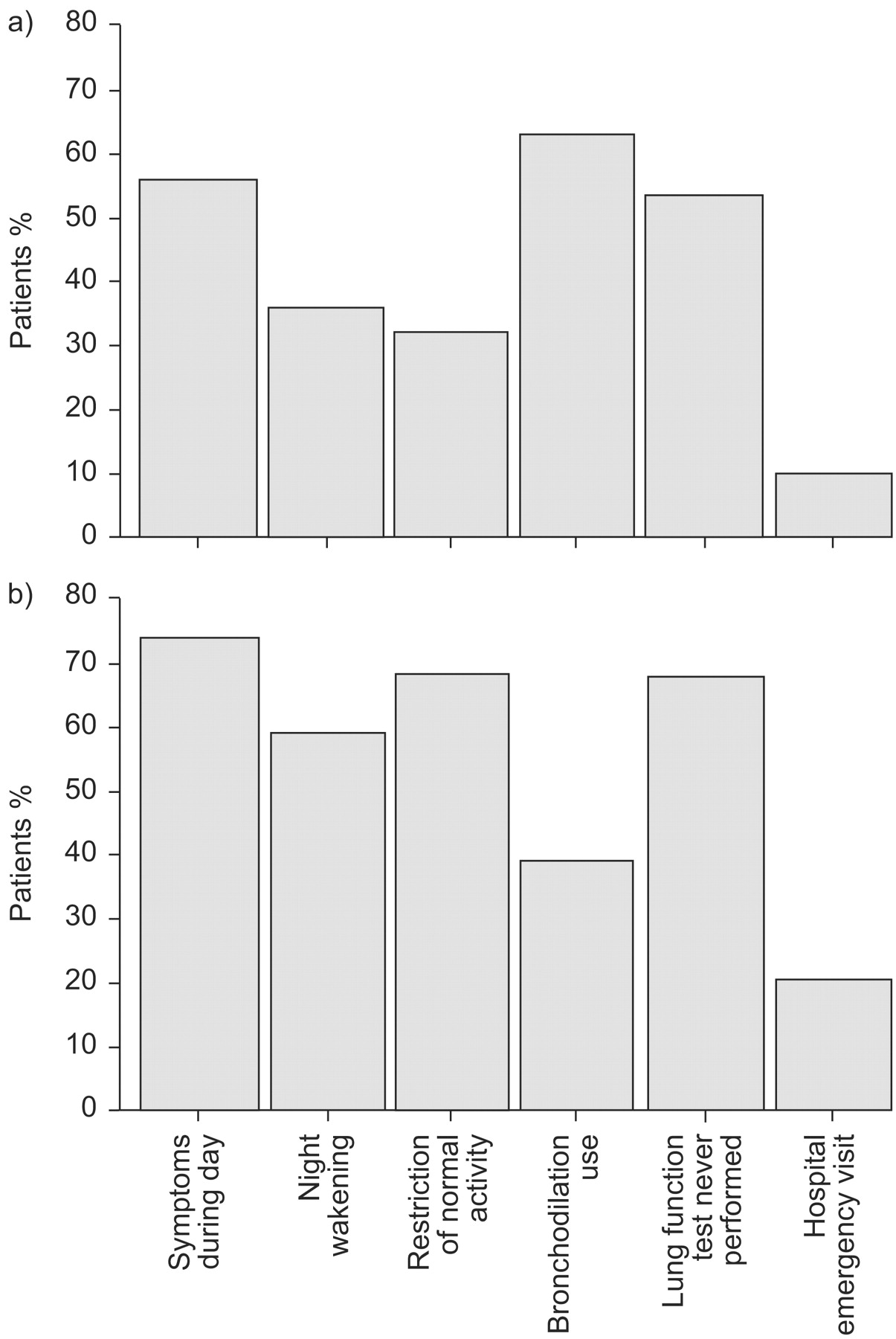
Despite the availability of these guidelines, many asthma patients remain uncontrolled. Clinicians may not be adequately connecting with patients and as a result the message of gaining control may not be communicated to patients. In Europe, studies suggest that levels of asthma control fall well short of GINA goals. The Asthma Insights and Reality in Europe (AIRE) study interviewed members of almost 3,000 households with asthma patients in France, Germany, Italy, the Netherlands, Spain, Sweden and the UK, and found that only 5.3% met the GINA criteria for asthma control 41. In addition, 18% of children and 11% of adults reported at least one emergency room visit, and 7% had required hospitalisation in the past 12 months. Additional AIRE studies conducted in Central and Eastern Europe, the USA and Asia suggest that suboptimal asthma control is a global phenomenon 12. All participating regions performed equally poorly on the different GINA goals and the frequency of hospital admissions and emergency visits were similarly high across regions (fig. 1⇓).

{kind=link}
Patients with uncontrolled asthma in AIRE studies 12. a) Western Europe; b) Central and Eastern Europe.
The reasons for poor control are complex and involve both clinical and behavioural factors, such as poor implementation of guidelines, inadequate use of available therapies, lack of adherence to therapeutic regimens, lack of patient engagement with their treatment plan, and disagreement between clinicians and patients on what constitutes asthma control 42. A small proportion of patients, ∼5%, have poor asthma control despite frequent use of inhaled corticosteroids (ICS). These patients typically have significant clinical comorbidity and/or true therapy resistance 43 and remain an important target for research. For the vast majority of asthma patients, however, good control should be achievable.
Surveys report undertreatment of asthma, even in patients with severe, persistent disease. In the AIRE study, patients with more severe asthma symptoms were not the more frequent users of preventive medication 12. In fact, people with persistent asthma had high use of quick-relief medications, suggesting poor overall control. Paradoxically, there is also evidence of widespread overtreatment with ICS. A survey including >30,000 asthma patients in the UK found that 27% of patients were receiving ICS doses of >800 mcg·day−1 beclomethasone or equivalent 44. Of these, 32% had not received a trial of add-on therapy as recommended in current treatment guidelines. Add-on therapy has the potential to improve outcomes and allow patients to remain on a lower dose of ICS. Among children, a similar study found a comparable pattern of high ICS doses and a low use of add-on therapy 45. As a result, many patients receiving regular maintenance therapy remain uncontrolled 46, reflecting a failure to either implement available treatment guidelines or translate them adequately at a public level 47.
The Italian Study on Asthma in Young Adults suggested that one of the reasons for poor asthma control is inadequate use of available asthma medications 48. Almost half of persistent asthmatics were using a medication regimen below their asthma severity level and 66% had not used their medication daily over the past 3 months. Good control of the disease was positively associated with an adequate dose of anti-inflammatory medication and good asthma control was achievable if GINA recommendations were followed. A review of epidemiological studies involving >20,000 asthmatic children worldwide reported high frequencies of sleep disturbances, emergency visits, school absence and limitations of physical activity due to asthma 49. It was suggested that low expectation on the level of achievable asthma control among parents and physicians was an important contributing factor. Parents did not seem to be adequately informed about the importance of controlling the underlying inflammation and were thus unaware of the consequences of failing to adhere to anti-inflammatory medications.
Nonadherence to treatment regimens is common among asthma patients, but its relationship with asthma outcomes is complex. Many patients have strong beliefs, which may be mistaken, about their need for medication and potential side-effects. Case–control studies suggest that patients who have had emergency room care and hospitalisation are less adherent than those who have not required hospital care 50. In contrast, population studies tend to show that there is no relationship between adherence and outcome, or that good adherence is related to a worse outcome 42. A recent study found that quality of life in patients with mild asthma was similar regardless of how patients took their medication 51. However, in patients with moderate-to-severe asthma, regular treatment led to a significantly better quality of life and fewer emergency care visits compared with patients who took their medication as needed or patients who initiated dose reduction.
Patient perception of asthma may differ from that of clinicians, leading to disagreement on what exactly constitutes asthma control. In the AIRE study, ∼50% of patients with severe persistent symptoms believed their asthma to be well controlled, despite high levels of healthcare use and relatively poor quality of life 41. Similarly, a study of patient perceptions in the UK, Germany and Spain found that 34% of asthma patients considered their asthma to be “very well controlled”, even though 38% of the group experienced night wakening, 6% required emergency care and 7% missed social activities during the previous 3 months 52. In addition, 46% had at least one symptom and had used a bronchodilator at least once during the previous week. In France, a survey of >1,500 asthma patients found that 70% of patients were inadequately controlled and 69% failed to recognise their poor control, instead believing that they were completely or well controlled 53. Breathlessness, use of rescue medication and impairment of daily activities were common. The study found that these issues were independent of patients' characteristics and asthma management, highlighting the need for patients to receive better asthma education so that they can become more engaged in their own treatment.
To address poor control, physicians need to focus on controlling asthma and not simply on adherence. Patients require routine individualised evaluation that can identify psychological and lifestyle factors that may contribute to inadequate asthma control and poor outcomes. Patient education that focuses on the benefits and risks of treatment is crucial, as is professional education that emphasises the importance of engaging the patient. Poor asthma outcome is associated with psychological morbidity and some patients may benefit from management of that morbidity. Treatment options may include lifestyle modification (exercise and diet) along with psychological interventions and drug therapy. Improving asthma outcomes in the real world requires careful evaluation of the needs of individual patients.
EFFICACY, EFFECTIVENESS AND REPRESENTATIVENESS IN ASTHMA TRIALS
According to GINA guidelines, the goal of asthma treatment is to achieve and maintain control of symptoms, prevent exacerbations and hospital visits, minimise use of rescue medications and maintain normal activity levels and pulmonary function 1. Therapy is designed to achieve these goals, but it remains unclear how control is best achieved. These issues will also be addressed in an upcoming American Thoracic Society (ATS)/European Respiratory Society (ERS) joint Task Force report on asthma control and exacerbations, which examines standardising end-points for clinical asthma trials.
Results from clinical trials (upon which guidelines are based) differ depending on the outcome measure examined. For example, it has been shown that lung function and use of rescue medication are similarly improved by either ICS or long-acting β-agonists (LABA), but that other end-points, such as inflammatory biomarkers, exacerbations and treatment failures, are significantly worse with LABA treatment 54. It has also been suggested that the addition of a LABA provides better asthma control than increasing the anti-inflammatory treatment. This is particularly relevant because of the fixed combination products that are now available. According to the Gaining Optimal Asthma Control (GOAL) study, use of a fixed ICS/LABA combination produced better outcomes than ICS alone in a variety of different subgroups of patients 55. However, patients in the trial were included only if they if they had a β2 reversibility of ∼15%, and the mean reversibility in the trial was ∼23%. Thus, these patients were preselected to be very good LABA responders. In contrast, the Oxis and Pulmicort Turbuhaler In the Management of Asthma (OPTIMA) trial reported that addition of a LABA improved lung function but resulted in more poorly controlled days compared with ICS alone 56. The results differ from the GOAL study because patients were selected on the basis of having symptomatic asthma and not on the basis of LABA responsiveness.
Although asthma guidelines recommend that treatment should be evidence based, it has become clear that patients included in clinical trials are different from patients in real practice. Clinical trial patients typically include those who: have asthma according to ATS criteria; have forced expiratory volume in one second of >50 and <85% of predicted; have historical reversibility of >12% in the last 12 months; and are nonsmokers with no significant comorbidity. When these and other standard criteria were applied to 334 patients with asthma in a study in Norwegian asthma clinics, only 11 (3.3%) of the patients would have been eligible for inclusion in a typical asthma clinical trial 57. A further systematic analysis shows that the major asthma randomised controlled trials on which the GINA guidelines are based may have limited external validity as they have been performed on highly selected patient populations and that most of the participants with current asthma on treatment in the community would not have been eligible for these trials 58. A good example is asthma therapy in patients who smoke who are almost always excluded from asthma trials. In such patients, corticosteroids have limited effects 59 and other approaches to treatment maybe more effective 60. Another example is the demand in many efficacy studies for 12–15% reversibility with a bronchodilator, yet many patients do not achieve this and are therefore excluded. By selecting patients on the basis of their response to a β2-adrenoceptor agonist for inclusion in trials will automatically lead to a bias in the subpopulation studied, especially in the knowledge that for this measure there are ethnic 61, age-related 62, 63 and genetic variations 64. Therefore, the current evidence base used in asthma management guidelines obtained largely from company-sponsored efficacy trials are far from ideal for recommending asthma therapy in the real-world setting.
Every clinical trial should be judged by its ability to translate to a larger real-life population. Since current clinical trials are limited in this respect, there is a clear need for pragmatic real-world effectiveness trials that include typical patients seen by physicians in daily clinical practice. There is also a need for a wider range of outcomes to be examined, such as inflammation or quality of life. It may also be useful to examine composite outcome measures, which may better reflect the complexity of asthma.
PAEDIACTRIC ASTHMA
The dramatic increase in the prevalence of asthma seen recently is primarily due to the increase in childhood asthma. In Europe, asthma is now the major chronic illness of childhood; up to 20% of children are affected and asthma is the most common reason for hospitalising children 65.
Children are a heterogeneous group that differ developmentally, physiologically and psychologically from adults. The ongoing growth and maturation of organs affects both the disease course of asthma and the efficacy of medications. Consequently, asthma is a different disease in children than in adults and medications suitable for adults may not be successful in children 63, 66. Nevertheless, more than half of all asthma drugs prescribed for children have not been adequately tested in a paediatric population and the doses given to children are approximated from adult doses. In the absence of specific paediatric studies, children may be inadequately treated and exposed to unwanted adverse events.
Current treatment guidelines do not contain enough information on paediatric asthma, and the information that is provided is not being followed. Prescribing trends among children show that a combination of ICS and β-agonist therapy has become the mainstay of treatment in children, despite a complete lack of evidence in this population 14. High, unlicensed doses of ICS are frequently prescribed for children and the fact that ICS can affect growth 67 is not reflected in the labelling. A similar situation exists for inhaled β-agonists 68. In addition, the metered-dose inhalers and dry powder inhalers used to deliver asthma medications were developed for use in adults but are used in children despite important differences in efficiency, drug distribution and the ability of the child to use them successfully 69.
There is a clear need for clinical trials that examine the efficacy and safety of asthma medications in children. Since asthma differs throughout childhood, these trials should examine preschool children, school-age children and adolescents separately. It has been suggested that it may not be ethical to test medications in children 70. However, the current off-label use of medications that lack an evidence base in children and may produce unwanted adverse events may also be unethical. Furthermore, children will be carefully monitored in a clinical trial setting and should be protected by legislation that ensures ethical treatment. A sound evidence base in children is likely to lead to reduced hospital days, fewer deaths and increased quality of life.
The European Regulation on Medicines for Paediatric Use came into force in January 2007 71. This new regulation encourages the development of medicines for paediatric patients by offering incentives in the form of patent extensions and market exclusivity to pharmaceutical companies that study these medicines and produce paediatric formulations. The regulation requires the European Medicines Agency to develop a European network for paediatric clinical trials; community research programmes will provide funding for research into off-patent medications. The overall aim of the regulation is to improve the health of children in the European Union (EU).
NEW AVENUES FOR RESEARCH
The new European Regulation on Paediatric Medicines is an important step that should stimulate new clinical trials in children with asthma. However, a great deal of work remains to be done in understanding the aetiology and pathology of asthma, and the disease course in infants and small children. The development of atopy and asthma is linked to both genetic and environmental conditions and research is needed to understand these interactions and the link to systemic outcomes. It has become clear that wheeze tends to persist in atopic children, and early sensitisation to perennial allergens has been associated with a loss of lung function at school age 72. The development of asthma is also related to pollution, lifestyle, housing, allergy, infection and diet. However, it remains unclear why these environmental factors cause asthma in one individual but not in another. Atopy also appears to have a genetic component, since children with two atopic parents have a greatly increased risk of becoming sensitised and developing wheeze. However, the genetic components of asthma and atopy are complex 73, and the nature of the relationship between genes and environment remains unclear.
Some environmental factors appear to be protective, such as exposure to bacterial cell wall products, which is inversely related to the development of seasonal allergic rhinoconjunctivitis or immunoglobulin E responses that may lead to chronic airway diseases 74. In addition, microbial infections have been associated with a lower risk of allergic sensitisation 75. It has been suggested that this finding is related to a disconnection between humans and the microbial soil 76, a theory that has been illustrated by the different rates of sensitisation to allergens seen in populations living in geographically adjacent areas with fundamental differences in living conditions and lifestyles 77. Populations that do not appear to become sensitised should be studied more closely to ascertain whether there is a common denominator.
There is still no cure for asthma and there have been few new treatment innovations. In particular, there are currently no medications that can alter the natural history of the disease. Work is needed to identify the underlying causes of asthma, understand the complex genetic and environmental influences, and develop appropriate new treatment strategies. The real challenge for the future will be to develop strategies that prevent young children from ever developing asthma.
ASTHMA: A PUBLIC HEALTH ISSUE
There are significant disparities in asthma management practices and asthma control between European countries. In one large study involving asthma patients in France, Germany, Italy, the Netherlands, Spain, Sweden and the UK, access to medical care was found to vary widely between countries, as did the frequency of lung function testing and use of written asthma management plans. In addition, there were statistically significant differences in emergency room visits and hospitalisations from country to country 78. The authors of that study concluded that education and public health resources are needed to increase awareness about the severity of asthma and to ensure proper treatment.
Public health initiatives are required to encourage asthma education for both patients and healthcare providers. Patient education should emphasise the need for regular anti-inflammatory therapy but should also highlight that patients need to be in control of their own asthma management. Healthcare providers must recognise the individual nature of asthma and the need to target poor outcomes by identifying the factors responsible. Key public health issues that should be targeted at the EU level include smoking cessation, dietary improvement and obesity reduction, and pollution control. Smokers are typically excluded from clinical trials and it has now been shown clinically that they often fail to respond to ICS treatment 79. Maternal diet during pregnancy, particularly vitamin deficiency, appears to influence the likelihood that the child will develop asthma 80 and asthma patients who are obese are more likely to be uncontrolled 81. The effect of pollution on asthma is clear and has been widely reported 82.
The successful implementation of a public health approach to asthma has been exemplified by the Finnish Asthma Programme, which showed that early diagnosis, active treatment and guided self-management combined with patient education, and reductions in tobacco smoking and environmental tobacco smoke can improve asthma outcomes and reduce cost 83. There is a clear opportunity to make asthma a public health priority and implement such programmes across Europe.
CONCLUSION
The new understanding of asthma as a systemic inflammatory disease is not reflected in current guidelines or management strategies, and few available treatments address the wider systemic inflammation. Instead, current diagnosis and management focus on improving function in the central airways. Consequently, treatment choices are limited, patients with asthma do not receive individualised care and many have uncontrolled asthma.
The Brussels Declaration on Asthma calls for important clinical and regulatory changes to be made to the diagnosis and management of asthma and highlights the need for new research. These changes should reflect the latest scientific understanding of the disease and should ensure that patients receive optimum treatment. Action on all points of the declaration is essential to ensure a better outcome for asthma patients across Europe.
Support statement
Costs and expenses to hold a summit meeting and develop the Brussels Declaration were covered by the AAIR Charity.
Statement of interest
Statements of interest for H. Bisgaard, L. Bjermer, T. Haahtela, J. Haughney, R. Horne, A. McIvor, S. Palkonen, D.B. Price and M. Thomas, and for the study itself can be found at www.erj.ersjournals.com/misc/statements.shtmlThe Brussels Declaration on Asthma was initiated by participants at a Policy Roundtable on Asthma held at the European Parliament in January 2006, hosted by Member of the European Parliament L. Lynne and the International Primary Care Respiratory Group. The authors would like to acknowledge the work of S-E. Myrseth in contributing to the compilation and production of the present paper.
Acknowledgments
The Brussels Declaration on Asthma was initiated by participants at a Policy Roundtable on Asthma held at the European Parliament in January 2006, hosted by Member of the European Parliament L. Lynne and the International Primary Care Respiratory Group. The authors would like to acknowledge the work of S-E. Myrseth in contributing to the compilation and production of the present paper.
- Received April 7, 2008.
- Accepted August 5, 2008.
- © ERS Journals Ltd
References











Jump To
- Article
- Abstract
- DIAGNOSTIC ISSUES
- INFLAMMATION: A KEY PATHOLOGY IN ASTHMA
- UNDERSTANDING THE CAUSES OF POOR ASTHMA CONTROL
- EFFICACY, EFFECTIVENESS AND REPRESENTATIVENESS IN ASTHMA TRIALS
- PAEDIACTRIC ASTHMA
- NEW AVENUES FOR RESEARCH
- ASTHMA: A PUBLIC HEALTH ISSUE
- CONCLUSION
- Support statement
- Statement of interest
- Acknowledgments
- References
- Figures & Data
- Info & Metrics