





A 29-yr-old African male was admitted with a 1-week history of chest pain, shortness of breath and haemoptysis. He had returned from Africa by plane 2 weeks previously. The patient denied fever, sweats or weight loss. He had no significant past medical history, was not taking any regular medication, and was a lifelong nonsmoker. He lived in the UK and was in full-time education.
Physical examination did not reveal any abnormalities. Laboratory investigations showed elevated inflammatory markers, including an erythrocyte sedimentation rate level of 59 mm·h−1 and a C-reactive protein level of 53 mg·L−1, normal haemoglobin at 139 g·L−1 and leukocytosis of 14.6×109·L−1 with a predominance of neutrophils. Chest radiograph was normal. Computed tomography (CT) pulmonary angiography confirmed the presence of filling defects within branches of the right lower lobe, left lingular and left lower lobe pulmonary arteries, with no radiological evidence of right heart strain. Small nodules of ≤7 mm were identified in both lungs (fig. 1⇓). Several small mediastinal nodes were also identified. The patient was anti-coagulated with warfarin for bilateral pulmonary thromboembolism.

Computed tomography pulmonary angiography. Arrows show small pulmonary nodules.
The patient had further episodes of atypical chest pain and haemoptysis over the following month. He was readmitted with signs of right heart failure and normocytic anaemia. A repeat chest radiograph showed a globular heart with small bilateral pleural effusions. Consequently, transthoracic echocardiogram (TTE) confirmed a moderate-sized pericardial effusion with right ventricular collapse. Pericardiocentesis was performed, draining 620 mL of haemorrhagic fluid with no microbiological growth and no abnormal cells on cytological examination.
An autoimmune screen, an HIV test and thrombophilia screens revealed no abnormalities. Bronchoscopic appearances were normal. Bronchial washings and endobronchial ultrasound-guided fine-needle aspiration of subcarinal nodes did not show malignant cells. Bone marrow examination demonstrated reactive hyperplasia and showed no evidence of malignancy or tuberculosis. Repeat thoracic CT scan did not show any significant change in the size of the nodules.
A repeat TTE was performed at 6 months (fig. 2⇓) and the patient underwent cardiac magnetic resonance imaging (MRI) perfusion study (fig. 3⇓). Video-assisted thoracoscopic lung biopsy was also performed (fig. 4⇓).

Trans-thoracic echocardiogram; parasternal short axis window at the level of the aortic valve.

Magnetic resonance image of the thorax.

a and b) Haemotoxylin and eosin stained sections showing poorly differentiated malignant cells. c and d) Immunohistochemistry shows staining with vascular markers CD34 (c) and CD31 (d). Scale bars = 100 μm (a, c and d), and 50 μm (b).
BEFORE TURNING THE PAGE, INTERPRET THE TRANS-THORACIC ECHOCARDIOGRAM (FIG. 2⇑), CARDIAC MAGNETIC RESONANCE IMAGE (FIG. 3⇑) AND THE LUNG BIOPSY PATHOLOGY (FIG. 4⇑), AND SUGGEST A DIAGNOSIS.
Diagnosis: Right atrial angiosarcoma (figs 5⇓ and 6⇓) with multiple metastatic lung deposits and tumour emboli.
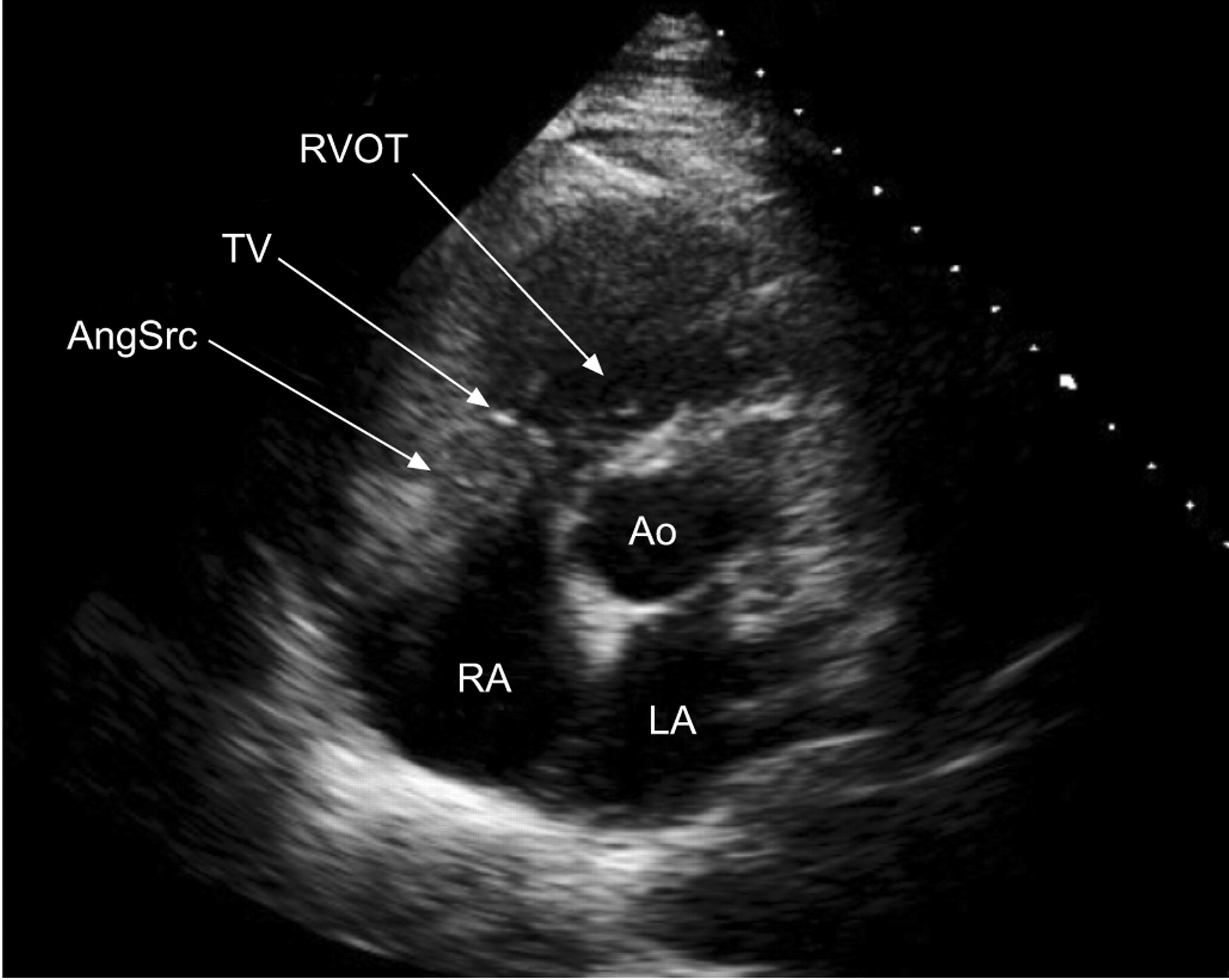
Trans-thoracic echocardiogram; parasternal short axis window at the level of the aortic valve. The tumour mass is seen infiltrating the posterior wall of the right atrium (RA) and abutting the tricuspid valve (TV). RVOT: right ventricular outflow tract; AngSrc: angiosarcoma; LA: left atrium; Ao: aortic valve.
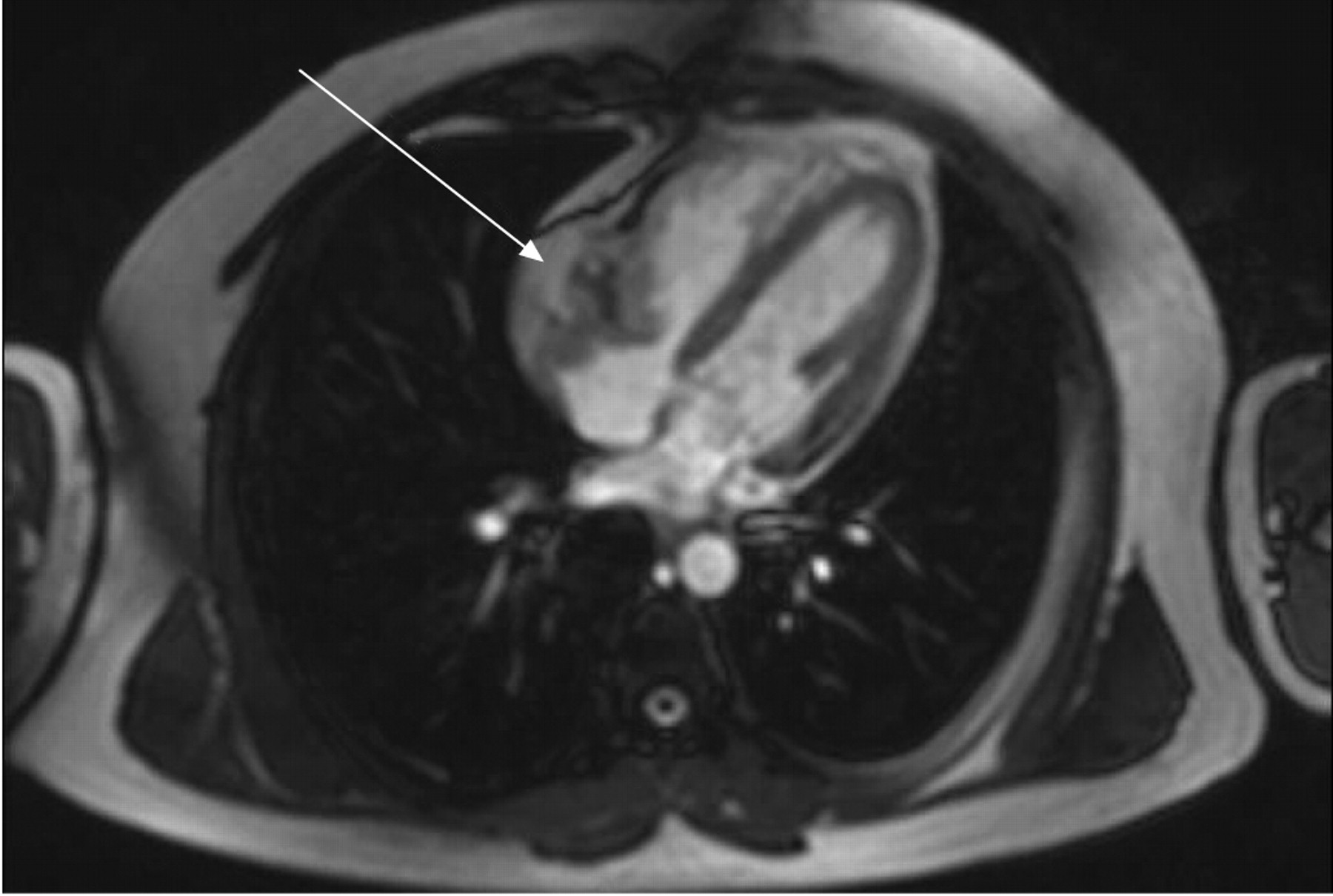
Magnetic resonance image of the thorax. The arrow shows the tumour arising from the right atrium.
CLINICAL COURSE
Following diagnosis, the patient was offered palliative chemotherapy. He opted to fly back to his home in Africa to receive treatment. Warfarin was discontinued in view of his haemorrhagic pericardial effusion and the likelihood that the pulmonary emboli were actually tumour emboli. Unfortunately, 2 months after returning to South Africa, the patient died of a stroke.
DISCUSSION
Primary cardiac tumours are rare, with an incidence of 0.007–0.019%. The most common malignant cardiac tumour is angiosarcoma, accounting for 37% of cases 1. Angiosarcomas are malignant neoplasms of endothelial cells varying from well-differentiated anastomosing vascular channels to undifferentiated tumour arranged as solid sheets of anaplastic cells. Immunohistochemical stains for CD31, CD34 and factor VIII-related protein confirm endothelial origin 2.
Cardiac angiosarcoma is two to three times more common in males than females, and tends to occur in the third to fifth decade 2. Patients often present late with locally advanced or metastatic disease. Historically, pathological diagnosis has been made at post mortem. The first ante-mortem diagnosis was made in 1959 by Crenshaw et al. 3.
In 90% of cases the tumour arises from the right atrium 4 and forms a well-defined intracavitory mass at risk of tumour embolisation, or else invades the pericardium leading to haemorrhagic pericardial effusion and tamponade 1. In the present case, both tumour embolisation and pericardial effusion occurred. The patient was at risk of thromboembolic disease due to his recent long-haul flight, but in the absence of risk factors, clinical suspicion of tumour emboli is required to make an early diagnosis. Pulmonary metastatic deposits are common 5.
The absence of cardiac signs in the patient described herein at first presentation is unusual but has been documented previously 5. Most patients present with right heart failure or cardiac tamponade. Atypical chest pains occur due to pericarditis in 75% of patients 5. Pericardial effusion may not recur following pericardiocentesis, as seen in the present case and others 6. Cytology of pericardial fluid demonstrates malignant cells in 80–90% of malignant pericardial effusion cases 7 but is frequently unhelpful in diagnosis of angiosarcoma 8.
In the present case, tumour was not initially identified at TTE, a situation acknowledged in other studies 6, 9. Cardiac magnetic resonance imaging provides three-dimensional images, enabling clinicians to evaluate tumour invasion into cardiac and adjacent mediastinal structures 10. Angiosarcomas have heterogeneous signal intensity, often with a “cauliflower” appearance. Diffuse pericardial infiltration may give rise to linear contrast material enhancement; a “sunray” appearance 11.
A multi-disciplinary approach to the treatment of patients with cardiac angiosarcoma has been advocated previously 1, 12. The high prevalence of metastatic disease often precludes curative surgery, and adjuvant chemotherapy has no proven role in the eradication of micro-metastatic disease 1. Adriamycin-based regimens are used but due to the rarity of the disease, no accepted treatment guidelines have been developed 2.
Primary cardiac tumours leading to pulmonary tumour emboli include atrial myxoma 13, papillary fibroelastoma 14, lipoma 15, rhabdomyosarcoma 16, osteosarcoma 17, liposarcoma 18 and lymphoma 19. Primary pulmonary artery undifferentiated sarcoma can present as chronic thromboembolic disease 20. Lung, breast or renal cell carcinoma are common secondary malignant cardiac tumours with propensity for pulmonary embolism 10.
Statement of interest
None declared.
- © ERS Journals Ltd











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}