





Abstract
Mild-to-moderate pulmonary hypertension is a common complication of chronic obstructive pulmonary disease (COPD); such a complication is associated with increased risks of exacerbation and decreased survival. Pulmonary hypertension usually worsens during exercise, sleep and exacerbation. Pulmonary vascular remodelling in COPD is the main cause of increase in pulmonary artery pressure and is thought to result from the combined effects of hypoxia, inflammation and loss of capillaries in severe emphysema.
A small proportion of COPD patients may present with “out-of-proportion” pulmonary hypertension, defined by a mean pulmonary artery pressure >35–40 mmHg (normal is no more than 20 mmHg) and a relatively preserved lung function (with low to normal arterial carbon dioxide tension) that cannot explain prominent dyspnoea and fatigue. The prevalence of out-of-proportion pulmonary hypertension in COPD is estimated to be very close to the prevalence of idiopathic pulmonary arterial hypertension.
Cor pulmonale, defined as right ventricular hypertrophy and dilatation secondary to pulmonary hypertension caused by respiratory disorders, is common. More studies are needed to define the contribution of cor pulmonale to decreased exercise capacity in COPD. These studies should include improved imaging techniques and biomarkers, such as the B-type natriuretic peptide and exercise testing protocols with gas exchange measurements.
The effects of drugs used in pulmonary arterial hypertension should be tested in chronic obstructive pulmonary disease patients with severe pulmonary hypertension. In the meantime, the treatment of cor pulmonale in chronic obstructive pulmonary disease continues to rest on supplemental oxygen and a variety of measures aimed at the relief of airway obstruction.
- Chronic obstructive pulmonary disease
- hypoxaemia
- inflammation
- oxygen therapy
- pulmonary hypertension
- vasodilator agents
SERIES “PULMONARY HYPERTENSION: BASIC CONCEPTS FOR PRACTICAL MANAGEMENT”
Edited by M.M. Hoeper and A.T. Dinh-Xuan
Number 6 in this Series
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality worldwide with an increasing prevalence during the past decades 1. One established complication of COPD is the development of pulmonary hypertension (PH). Typically, PH appears when airflow limitation is severe and is associated with chronic hypoxaemia, the main pathophysiological cause being chronic alveolar hypoxia, although new mechanisms have emerged recently. In older studies, mean pulmonary artery pressure (P̄pa) was significantly linked to the severity of COPD and was considered to be an important prognostic factor and part of the justification for long-term oxygen therapy (LTOT). Nowadays, in a time of LTOT, PH is a significant risk factor for hospitalisation 2 and is still associated with a shorter life expectancy 3. In most cases, PH is mild to moderate 4–6 but it may be severe and could be observed without major airflow limitation. This latter condition has been termed “out-of-proportion” PH. In a recent study 6, it has been reported that, unlike “usual” PH in COPD patients undergoing LTOT (the most common situation), out-of-proportion PH often leads rapidly to right heart failure and death. Given the increasing number of patients, the recognition of susceptibility factors for PH in this disease has important implications for a clear understanding of the natural history of COPD. A better diagnosis strategy for PH in COPD is also mandatory, as is new treatment, particularly in out-of-proportion PH. It must be emphasised that out-of-proportion PH does not match with any group of the last published classification of PH 7 and, thus, there is a need for a consensual definition of this condition.
PH is defined as P̄pa >20 mmHg and is placed in the heterogeneous group of PH associated with disorders of the respiratory system and/or hypoxaemia 7. The reason for setting such a threshold is that in healthy subjects P̄pa is always <20 mmHg at rest and, as stated above, a P̄pa >20 mmHg is associated with increased morbidity and mortality. However, in some recent studies PH was defined by P̄pa >25 mmHg 8, 9. These various definitions should be kept in mind when comparing studies, particularly in terms of prevalence of PH in populations of COPD. Although severe PH in COPD could be defined by P̄pa >35 mmHg in patients undergoing optimal treatment (including LTOT), it must be emphasised that this is not a consensual definition. Cor pulmonale is defined as right ventricular hypertrophy and dilatation or both, secondary to PH caused by respiratory disorders 10. This article is part of a review series on pulmonary hypertension 11–16.
EPIDEMIOLOGY OF PH IN COPD
Prevalence of PH in COPD
Determination of prevalence of PH in COPD has been hampered by difficulties in obtaining valid data from an adequate population-based sample of COPD. The main reason is that right heart catheterisation (RHC) cannot be performed on a large scale for ethical reasons and it is well known that echocardiography alone is subject to some error 17. Only studies of hospitalised subjects are available. Burrows et al. 18 reported 36 yrs ago that 50 patients with COPD and severe airflow limitation (forced expiratory volume in one second (FEV1)/vital capacity (VC) ratio of 37%) had an average P̄pa value of 26 mmHg. In a larger sample of 175 patients with a mean FEV1/VC ratio of 40%, Weitzenblum et al. 19 observed a prevalence of PH (defined as P̄pa >20 mmHg) of 35%.
The 120 patients with severe emphysema evaluated for participation in the National Emphysema Treatment Trial 20 had a mean±sd P̄pa of 26.3±5.2 mmHg. The 95% confidence interval (CI) of the true mean in such a population was 25.4–27.2 mmHg. These results obtained when LTOT was readily available confirmed that PH when present in patients with severe COPD is mild to moderate, but also extremely prevalent, since in this series of patients 91% had P̄pa >20 mmHg. Vizza et al. 21, in a cohort of 168 patients with COPD listed for lung transplantation, observed similar results in terms of P̄pa, with a 95% CI of 24.1–25.9 mmHg. Thabut et al. 8, investigating the two types of population, i.e. candidates for lung volume reduction surgery (LVRS) and candidates for lung transplantation, had comparable results. Mild (P̄pa 26–35 mmHg), moderate (36–45 mmHg) and severe (>45 mmHg) PH was present in 36.7, 9.8 and 3.7% of the 215 patients, respectively. In a large series of 998 patients with COPD 6 with less airway limitation and hypoxaemia than the two studies quoted above, the P̄pa was 20.3±8.1 mmHg. This latter study demonstrated that the prevalence of P̄pa >20 mmHg in hospitalised COPD patients is ∼50%. When considering patients listed for LVRS or lung transplantation the prevalence of PH would lie between 70–90%.
In the large population of patients with COPD, it is worthwhile to estimate the proportion of those with severe PH. In the study reported by Scharf et al. 20 considering pulmonary haemodynamics of patients with severe emphysema, only 5% of the population as a whole had P̄pa >35 mmHg. It should be made clear that this latter figure is underestimated since severe PH was a criterion of exclusion in the National Emphysema Treatment Trial 20. In the studies conducted in France by Thabut et al. 8 and by Chaouat et al. 6, 13.5% and 5.8% of the population had severe PH (P̄pa ≥35 mmHg), respectively. Interestingly, in these two studies P̄pa was positively skewed, indicating that a significant number of patients with COPD had severe PH (fig. 1⇓). Importantly, all the patients in both studies, even those with a high elevation of P̄pa, were in a stable state of the disease and had optimal treatment including LTOT.

Mean pulmonary artery pressure (P̄pa) in a hospital-based cohort of 998 chronic obstructive pulmonary disease (COPD) patients with a mild to very severe airflow limitation. It can be seen that severe pulmonary hypertension is uncommon in COPD but does exist. Data taken from 6.
The other method by which the prevalence of PH in COPD can be estimated is to look at recent epidemiological studies devoted to COPD. The prevalence of COPD among adults in eight European cities has been estimated to be as high as 6.2% 22. Knowing that COPD is usually progressive, many patients will be at risk of PH in the near future 23. Furthermore, it must be considered that this population of COPD has lot of comorbidities that could raise the level of PH. Indeed, ischaemic heart disease, hypertensive cardiomyopathy, chronic heart failure and worsening of chronic respiratory failure due to obesity are frequently encountered 24. According to a prevalence of COPD of ∼5% in the adult population in most European countries, and that 6% of patients have severe or very severe disease, the number of patients in Europe with severe PH (1% of the severe and very severe COPD patients are likely to have P̄pa >40 mmHg 6) may be ∼7,500. When related to the adult French population, the figure would be 650, which is very close to a prevalence of 15 cases per million patients with pulmonary arterial hypertension (PAH) in the same country 25. In light of all these studies, it is highly probable that the number of COPD patients with PH is high, with a mild-to-moderate increase in P̄pa in most cases, but undoubtedly there are also a significant number of patients with severe PH.
Prognostic impact of PH in patients with COPD
Before the introduction of LTOT, it was shown that PH in COPD was an independent prognostic factor. Indeed, patients with similar airflow limitation had lower life expectancy when P̄pa was above the normal value 19, 26. Now, LTOT improves the survival of hypoxaemic COPD patients. It has been suspected, but not clearly demonstrated, that the increased life expectancy was due to the improvement of pulmonary haemodynamics. Interestingly, P̄pa remains an excellent prognostic factor in patients undergoing LTOT 3, 27, 28. In the most recent study 3, patients with P̄pa >25 mmHg had a significantly lower survival rate at 5 yrs compared with patients without PH (33 versus 66%; p<0.001; fig. 2a⇓). Importantly, P̄pa >18 mmHg was associated with an increased risk of severe exacerbation in COPD patients with moderate to severe airflow limitation (fig. 2b⇓) 2.

Prognostic impact of pulmonary hypertension. a) Chronic obstructive pulmonary disease (COPD) patients with a mean pulmonary artery pressure (P̄pa) ≥25 mmHg (– – – –) at the beginning of long-term oxygen therapy have a significantly (p<0.001) shorter life expectancy compared with patients with P̄pa <25 mmHg (––––). Reproduced from 3 with permission from the publisher. b) COPD patients with P̄pa >18 mmHg (•) in a stable state of the disease have an increased risk of hospitalisation for exacerbation compared with patients with P̄pa ≤18 mmHg (○). Reproduced from 2 with permission from the publisher.
PATHOLOGY
The structural basis of PH in COPD includes three potential mechanisms: remodelling, reduction in the total number of pulmonary vessels, and pulmonary thrombosis 29, 30. In fact, the only structural basis of PH that is well investigated in pathology is the remodelling of pulmonary arteries and arterioles. However, loss of pulmonary vessels has been shown in experimental models of emphysema and is likely to play an important role in human disease too.
The anatomic abnormalities of pulmonary vasculature in COPD have been documented from necropsy material from patients with severe disease 31, 32. These studies have shown a muscularisation of pulmonary arterioles. This part of the pre-capillary vascular bed, <80 μm in diameter, is without muscular layer in normal subjects. In transverse section, pulmonary arterioles in severe COPD patients have distinct media of circularly oriented smooth muscle bounded on its outer and inner aspects by elastic laminae. The muscularisation of pulmonary arterioles can extend to the periphery in pre-capillary vessels as little as 20 μm in diameter. This phenomenon is due to hypertrophy, proliferation and transformation of the phenotype of contractile cells called pericytes, which are precursors of smooth muscle cell, or transformation of intermediate cells. In larger pulmonary arteries (80–1,000 μm in diameter in humans) the media can be thickened or focally atrophied 31, 33, 34. Muscularisation also occurs in the post-capillary vessels of patients with COPD 35 with a more important amount of extracellular matrix in veins and venules than in pulmonary arteries.
Changes in intima are an important part of the remodelling of pulmonary arteries in patients with COPD. These changes have been observed in patients with end-stage COPD and also in mild disease. Intimal thickening is observed in muscular pulmonary arteries and in pulmonary arterioles 31, 32. However, pathological studies in COPD have not shown complex lesions, which are frequently encountered in patients with PAH 36, such as plexiform lesions (irregular mass of endothelial cells) or angiomatoid lesions, characteristic of severe PH.
It has been known for many years that pulmonary artery lesions appear not only in patients with end-stage COPD but also in patients with mild COPD, and even in smokers with normal lung function 32, 37, 38. Inhaled noxious particles and gases in smokers lead to an inflammatory process with an increased number of CD8+ T-lymphocytes in the wall of central and peripheral airways of smokers and patients with COPD 39, 40. Interestingly, the same infiltrate of inflammatory cells is present in pulmonary vascular lesions.
PATHOPHYSIOLOGY
P̄pa represents the sum of the pulmonary artery wedge pressure (Ppw) and of the driving pressure across the pulmonary circulation. The latter is the product of cardiac output and pulmonary vascular resistance (PVR). Accordingly, one can write: 
where CO is cardiac output. Thus, three variables can contribute to an elevation of P̄pa: Ppw, cardiac output and PVR.
In a large series of COPD patients, a relatively high proportion (19%) of COPD patients with increased Ppw at rest has been reported 41. However, most of these patients had an associated left heart disease. In the haemodynamic study of the National Emphysema Treatment Trial, 61.4% of the 120 patients investigated at entry to the study had an abnormally high Ppw (>12 mmHg) 20. One hypothesis is that the increase in intrathoracic pressure in emphysematous patients may induce an increase in Ppw. During exercise, an almost constant increase in Ppw in patients of the emphysema type has been observed. Since right atrial pressure, pulmonary artery pressure (Ppa) and intra-oesophageal pressure increased in the same proportion as Ppw, it was concluded 20 yrs ago that this increase in Ppw was due to dynamic hyperinflation 42. The increase in Ppw observed in some COPD patients could also be due to left ventricular diastolic dysfunction secondary to cardiovascular comorbidities or to the so-called ventricular interdependence. This latter mechanism can occur only when the right ventricle is significantly dilated.
Therefore, PH complicating COPD is mostly of the pre-capillary type. A post-capillary component can participate to the increase in Ppa, particularly during exercise and acute exacerbations.
The factors leading to an increased PVR in COPD are listed table 1⇓. These factors are numerous but alveolar hypoxia is predominant. In addition, recent reports have suggested that inflammation may contribute to pulmonary vascular remodelling in COPD. In severe emphysema P̄pa and PVR were weakly correlated with diffusing capacity of the lung for carbon monoxide (DL,CO), suggesting that, in patients with markedly predominant emphysema, loss of pulmonary capillaries may play a role in the development of PH 20, 43.
Confirmed and suspected factors leading to an increased pulmonary vascular resistance in chronic obstructive pulmonary disease(COPD)
Inflammation
It has been hypothesised that the development of structural and functional abnormalities of pulmonary arteries in COPD is related to inflammatory cells in the vascular wall 44. However, few studies have confirmed this hypothesis. Peinado et al. 40 have reported a relationship between the number of inflammatory cells infiltrating the wall of pulmonary arteries on the one hand, and the enlargement of the intimal layer and endothelial dysfunction on the other. It is important to note that pulmonary vascular remodelling in this context does not necessary induce PH. The remodelling may take place in an outward direction and, therefore, does not reduce the vascular lumen. However, it has been shown recently that systemic inflammation in COPD appears to increase the risk for developing PH in COPD. Indeed, C-reactive protein 45, as well as pro-inflammatory cytokines, interleukin (IL)-6 and monocyte chemoattractant protein-1 46, were correlated with the level of P̄pa in two recent studies. In one of these studies, one form of a functional polymorphism of the IL-6 gene accountable for a higher expression of the gene was associated with a higher risk for the development of PH in a population of patients with severe and very severe COPD 46. The issue of the role of inflammation in PH complicating COPD remains controversial 47; however, in vitro and animal models of pulmonary artery remodelling related to tobacco smoke studies support such a mechanism 48.
Hypoxic PH
Alveolar hypoxia is probably the most important factor leading to an increased PVR 49. Acute hypoxia induces in humans, as well as in almost all species of mammals, a rise of PVR and Ppa that is accounted for by hypoxic pulmonary vasoconstriction (HPV) 50. This vasoconstriction is localised in the resistance pulmonary arteries (<500 μm). Its precise mechanism has recently been better identified. In particular, there has been a marked improvement of the knowledge of the smooth muscle cell potassium channels involved in the regulation of the pulmonary vasomotor tone 51 and of the endothelium-derived mediators 48, 52.
In normal humans, the reactivity of the pulmonary circulation to acute hypoxia varies from one subject to another 53 and this interindividual variability is also found in COPD patients 54. This means that some patients are “responders” to acute hypoxia, exhibiting a marked increase in PVR and Ppa during hypoxic challenge, whereas others are “poor responders” or even “nonresponders” (fig. 3⇓) 54.

Changes in mean pulmonary artery pressure (P̄pa) as a function of changes in arterial oxygen saturation (Sa,O2) from inspiratory oxygen fraction (FI,O2) 0.21 to 0.13 or 0.15. •: level of Sa,O2 at FI,O2 of 0.21 >90%; ○: level of Sa,O2 at FI,O2 of 0.21 <90%. Although there is a statistical significant correlation between changes in P̄pa and changes in Sa,O2 (n = 26, r = −0.665, p<0.001), an important interindividual variability can be seen. Reproduced from 54 with permission from the publisher.
Although HPV is less active in patients with significant structural changes of small pulmonary arteries, as observed in patients with severe COPD, this response of the pulmonary vascular bed to alveolar hypoxia can have important consequences in many clinical situations. Indeed, HPV can be involved during acute exacerbations of COPD, sleep-related hypoxaemia and exercise. The acute HPV onsets and resolves rapidly and is mainly due to a contraction of small pulmonary artery smooth muscle cells 55–57.
Chronic effects of hypoxia on the pulmonary circulation are mainly known from animal models of hypoxia-induced PH and in vitro studies 48. There are changes in structure and function of all cells and extracellular matrix of the pulmonary vascular wall. For instance, chronic hypoxia increases the synthesis and release of endothelin from endothelial cells 52 and, therefore, amplifies and extends the acute effect of hypoxia on voltage-dependent potassium (KV) channels. Nitric oxide and prostacyclin, two potent vasodilators synthesised by endothelial cells, are affected by chronic hypoxia. This produces an imbalance in favour of an increase of pulmonary vascular tone and a proliferative state of cells of the vascular wall.
Numerous components of the cellular “machinery”, such as KV channels, G-protein-coupled receptors, 5-HT transporter, grow factors, pro-inflammatory cytokines and RhoA/Rho kinase signalling pathway contributes in complex interplays to the remodelling process of pulmonary arteries under chronic hypoxia 48, 58–62.
These observations suggest that pulmonary inflammation, systemic inflammation, chronic hypoxia, loss of pulmonary capillaries in severe emphysema and perhaps mechanical injury due to hyperinflation, in complex interactions, contribute to the development of PH in COPD (fig. 4⇓).

Confirmed and suspected mechanisms leading to pulmonary hypertension in chronic obstructive pulmonary disease, which, as shown, are influenced by genetic factors.
NATURAL HISTORY OF PH IN COPD
Exercising PH
In COPD, it has been noted that PH may first appear during exercise and during sleep. Kessler et al. 63 followed up 131 COPD patients with mean±sd FEV1 45±16% predicted and mild hypoxaemia (71±13 mmHg) during a mean time interval of 7±3 yrs. None of these patients had PH at baseline (P̄pa 15±3 mmHg). Among them, 76 had exercising PH defined by P̄pa ≥30 mmHg. In that study, patients having exercising Ppa at onset were more prone to develop resting PH with time. The other important finding of the study by Kessler et al. 63 is the slow progression of P̄pa with time (+0.4 mmHg·yr−1). It is also important to note that the change of P̄pa during the follow-up was correlated with the change of arterial oxygen tension (Pa,O2), the more Pa,O2 worsened the more P̄pa increased. The slow progression of P̄pa was also demonstrated in more advanced COPD patients with PH at rest in an earlier study 64.
In advanced COPD, patients with resting PH have a marked increase in Ppa during steady-state exercise 42, 65, 66: a COPD patient whose baseline P̄pa is modestly elevated (25–30 mmHg) may exhibit severe PH (50–60 mmHg) during moderate exercise (30–40 W). This is explained by the fact that PVR does not decrease during exercise in advanced COPD patients 65, 66, whereas it does in healthy subjects; as cardiac output is doubled for this level of exercise, P̄pa increases by ∼100%. From a practical viewpoint, this means that daily activities, such as climbing stairs, or even walking, can induce marked PH.
Peaks of PH during sleep
Some COPD patients who are normoxaemic or mildly hypoxaemic during the day develop moderate to severe hypoxaemia during sleep 67, 68. These episodes of hypoxaemia are due to alveolar hypoventilation which occurs mainly in rapid eye movement (REM) sleep. They coincide with transient increase in Ppa 69, 70. It has been hypothesised that intermittent episodes of PH during sleep in COPD could lead to permanent PH 71. However, the investigations performed in this area are rather controversial. Indeed, one group found that desaturations during sleep is a risk factor for developing permanent PH 72 and is associated with a worse prognosis 73, while another group found the opposite to be the case 74, 75.
Rise of PAP during exacerbation
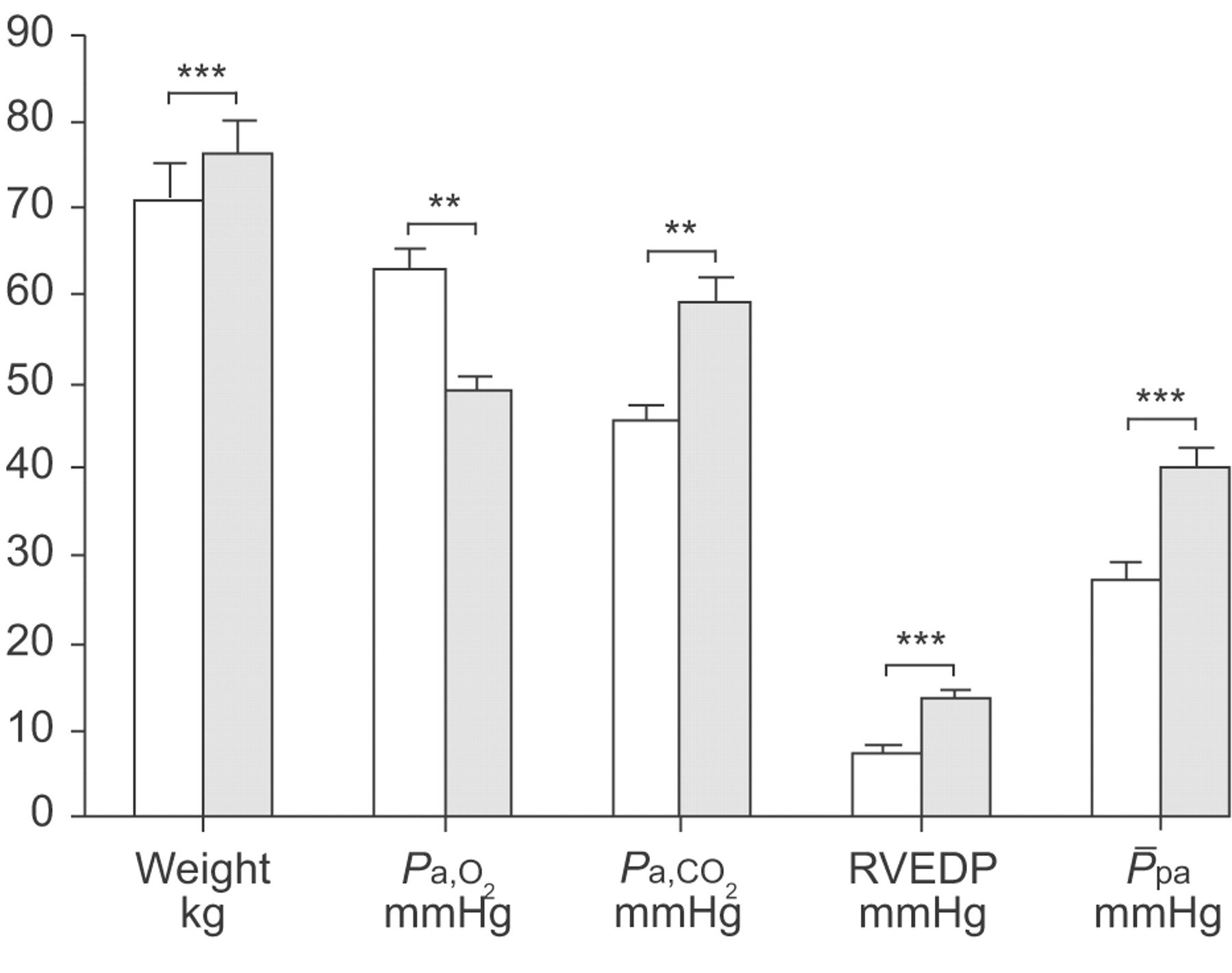
It has also been observed that some COPD patients have a pronounced increase in Ppa during acute respiratory failure. P̄pa may increase by as much as 20 mmHg and returns to its baseline value after the recovery of the exacerbation 76. Weitzenblum et al. 77 have investigated 16 COPD patients exhibiting marked peripheral oedema. Nine out of the 16 patients had an important increase in P̄pa compared with baseline values (fig. 5⇓) associated with haemodynamic signs of right heart failure (right ventricular end-diastolic pressure >12 mmHg). It is noteworthy that the change in P̄pa during the episode of peripheral oedema compared to a stable state of the disease was highly correlated with the change in Pa,O2 (r = −0.75, p = 0.02). Anand et al. 78 have observed similar behaviour of pulmonary haemodynamics and arterial blood gases under comparable circumstances. Frequent exacerbations of COPD can result in both more rapid declines in lung function and worse outcomes 79. It is also known that COPD patients with PH have an increased risk of having severe exacerbations 2. The occurrence of exacerbation is due to an interaction between the host on one hand and viruses, bacteria and environmental pollution on the other 79. The exact link between exacerbations and the natural history of permanent PH in COPD is not precisely known. It can be speculated that the repetition of exacerbation associated with transient increase in Ppa could lead to permanent PH, this latter state being classically associated with a worse prognosis 19.

Evolution of weight, arterial oxygen (Pa,O2) and carbon dioxide (Pa,CO2) tensions, right ventricular end-diastolic pressure (RVEDP) and mean pulmonary artery pressure (P̄pa) from baseline (□) to an episode of oedema due to right heart failure mostly associated with an acute exacerbation of the disease (░) in nine chronic obstructive pulmonary disease patients. Notably, the changes in P̄pa were significantly correlated with the changes in Pa,O2 (r = −0.75, p = 0.02). Data are presented as mean and sem. 1 mmHg = 0.133 kPa. **: p<0.01; ***: p<0.001. Data are taken from 77.
Pulmonary haemodynamics during a period of disease stability
During stable disease state, most patients with advanced COPD have mildly or moderately increased Ppa at rest. For instance, in a recent study investigating a large series of COPD patients during in a stable state of the disease, the average value of P̄pa was at the limit of the normal range (20±8 mmHg), although the airway limitation was of great magnitude (FEV1 33±11% pred) 6. This confirmed earlier reports establishing that when present in COPD, PH is mild or moderate and contrasts with the severity of PH in idiopathic PAH.
The most recent classification of PH was designed for associating entities with common pathophysiological and clinical features 7. Table 2⇓ compares the pulmonary haemodynamic data of COPD patients exhibiting PH 6, 19, a series of patients from the French registry of PAH 25 and a series of chronic thromboembolic PH from San Diego (CA, USA) 80. From these data it can be concluded that when PH occurs in COPD, PVR is moderately increased on the one hand, and right ventricular pre-load pressures and cardiac output are usually in the normal range on the other, contrasting with the large increase in PVR and haemodynamic signs of right ventricular dysfunction observed in patients with PAH and chronic thromboembolic PH.
Comparison of pulmonary haemodynamics in two series of chronic obstructive pulmonary disease(COPD) patients, and patients with idiopathic pulmonary arterial hypertension (iPAH) and chronic thromboembolic pulmonary hypertension (CTEPH)
Right ventricular dysfunction in COPD
Patients with stable COPD having moderate to severe airway limitation without hypoxaemia have preserved right ventricular systolic function at rest 81. Indeed, in a series of 25 patients with an FEV1 of 41±15% pred and a Pa,O2 82±10 mmHg (10.9±1.3 kPa), right ventricular ejection fraction measured by magnetic resonance imaging (MRI) method was 53±12%, and was similar in 26 normal controls (53±7%). In 158 patients with COPD evaluated for lung transplantation, the prevalence of right ventricular dysfunction was 59% 21. In 120 patients with severe emphysema Scharf et al. 20 found a mean right ventricular ejection fraction of 34±8%. The same study showed that P̄pa and Pa,O2 were the only covariates included in a multivariate regression analysis to predict right ventricular ejection fraction. These two covariates explained only 13% of the variance of right ventricular ejection fraction. It must be kept in mind that right ventricular ejection fraction is the result of complex interaction between pre-load, afterload and right ventricular contractility, and most published studies have not assessed all these interactions. The best manner in which to study right ventricular function is to determine the end-systolic pressure–volume relationship. Studies performed with this method have shown that decreased right ventricular contractility is observed only during acute exacerbation with the presence of marked peripheral oedema 82. Apart from acute exacerbation, indicators of right heart failure could be hardly observed in COPD patients even in the most advanced stage of the disease.
Severe and out-of-proportion PH
As aforementioned, PH in COPD is usually mild to moderate; however, owing to the high prevalence of COPD, it can be observed as an associated disease which could also impact on the pulmonary circulation in an additive manner. In a large series of COPD patients investigated during a period of disease stability, 27 had a P̄pa ≥40 mmHg and, among them, 16 had an associated disease explaining, in part, the severity of PH 6. Four had a left heart disease responsible for an increased Ppw and a decreased left ventricular ejection fraction. Two patients had chronic thromboembolic PH and six had an associated restrictive lung disease (mainly severe obesity plus obstructive sleep apnoeas), which also falls into the group of PH associated with hypoxaemic pulmonary disorders in the latest classification of PH 7. In these six latter patients, Pa,O2 was very low (44±4 mmHg; 5.9±0.5 kPa) with a further decrease during sleep and was associated with an increased arterial carbon dioxide tension. Consequently, it must be emphasised that hypoxaemic pulmonary disease could lead to the development of severe PH and right heart failure. Alveolar hypoxia due to alveolar hypoventilation must be a predominant cause of PH in such a circumstance. In the view of these results, it must be recommended that the presence of an associated disease should be investigated in COPD patients with severe PH, since treatable associated conditions covered up by COPD could be found. In the same study devoted to severe PH in COPD, 11 patients had COPD as the only cause of severe PH 6. These patients exhibit a distinctive pattern with less severe airflow limitation but more severe hypoxaemia, hypocapnia and decreased DL,CO (fig. 6⇓). Thabut et al. 8 have found similar characteristics in a group of 16 COPD patients 83. These two studies do not supply information of the natural history of the disease, but it is unlikely that severe PH was the result of the progression of COPD, knowing that airflow limitation was not severe 6, 8. Therefore, such a condition could be termed out-of-proportion PH and may be defined by P̄pa >35–40 mmHg and a mild-to-moderate airflow limitation. In the current authors' opinion, in a time of LTOT it is probably the sole situation in which right heart failure can be observed in COPD patients in a stable state of disease at some distance from an acute exacerbation. It must be clarified that the cause of hypoxaemia in this situation is a worsening of ventilation–perfusion mismatch and probably, in some patients, the development of a right-to-left shunt, and not alveolar hypoventilation due to severe airflow limitation.

Comparisons of vital capacity (VC), forced expiratory volume in one second (FEV1), FEV1/VC ratio, diffusion capacity for carbon monoxide (DL,CO), arterial oxygen (Pa,O2) and carbon dioxide (Pa,CO2) tensions and mean pulmonary artery pressure (P̄pa) between 16 chronic obstructive pulmonary disease (COPD) patients with no associated disease and a P̄pa ≥20 and <40 mmHg (□) and 11 COPD patients with no associated disease and a P̄pa >40 mmHg (░). It can be seen that in the group of patients with severe pulmonary hypertension (░), Pa,O2 and DL,CO was significantly lower, although airway obstruction was less severe. 1 mmHg = 0.133 kPa. **: p<0.01. Data are taken from 6.
Due to the severity and the scattered number of COPD patients with out-of-proportion PH, these patients should be referred to an expert centre of pulmonary vascular diseases to perform an RHC and to include them in registries and clinical trials.
DIAGNOSIS STRATEGY
Recognition of PH in COPD is often hampered by the clinical picture of the causal disease. Symptoms such as dyspnoea on exertion and fatigue are generally present in advanced COPD patients with or without PH; they are essentially the consequence of airflow limitation and hyperinflation rather than PH. However, one study has shown that patients with out-of-proportion PH in COPD have more severe dyspnoea on exertion in comparison with COPD patients, with more-severe airflow limitation but lower Ppa 6.
Physical signs that are observed in severe PH, and particularly in idiopathic PAH, such as a loud pulmonary component of the second heart sound and a pansystolic murmur owing to tricuspid regurgitation (TR), are rarely noticed in COPD patients with PH, except during severe exacerbations of the disease. This can be explained by the presence of mild-to-moderate PH in most of the patients and by the late occurrence (or no occurrence at all) of right heart failure. Peripheral oedema occurs rather late in the course of COPD and is not synonymous with right heart failure 78.
ECG may predict the presence of right ventricular hypertrophy, which is not exactly synonymous with PH. Most recognised ECG changes have a good specificity (>85%) but their sensitivity is poor (∼40%), particularly in patients with mild PH 84. Similarly, chest radiography is poorly sensitive in the diagnosis of PH in COPD. Nevertheless, these two conventional tests may be useful, on account of their simplicity and low cost, in raising suspicion of PH.
Prediction of Ppa from pulmonary function data
Spirometry is mandatory for the diagnosis of COPD; however, VC, FEV1 and FEV1/VC have no utility in the prediction of Ppa in COPD. This is not surprising, since PH itself has little effect on lung mechanics 85.
Significant correlations between Pa,O2 or arterial oxygen saturation (Sa,O2) and Ppa have been regularly demonstrated and there have been attempts to predict the level of Ppa from arterial blood gases. A predictive equation of Ppa from Sa,O2 and pH was proposed >20 yrs ago 86. It later appeared that this formula was unreliable for predicting Ppa in individuals, because the margin of error was too great. This is not surprising, since correlations between Pa,O2 and Ppa are loose, with Pa,O2 explaining only 25% of the variance of Ppa.
Better results could perhaps be obtained by a multivariate analysis including arterial blood gases and pulmonary volumes 86: stepwise multiple regression analyses generally explained <50% of the total variance of Ppa. A qualitative diagnosis of PH is often possible, but the prediction of the level of Ppa is too imprecise. DL,CO is reduced in patients with severe PH; however, on this sole measurement PH cannot be predicted since the decrease in DL,CO can also result from lung emphysema.
Although there are important limitations of pulmonary function data in predicting PH, it must be mentioned that unusual patterns have been described in two studies that underlined out-of-proportion PH 6, 8. Indeed, in both studies, most patients with the highest P̄pa have relatively preserved lung mechanics, very low Pa,O2, a huge increase in alveolar-arterial oxygen tension difference and a tendency to have hypocapnia. One of these studies also showed that DL,CO was more reduced than usual in lung emphysema 6. Therefore, such a pattern of pulmonary function tests associated with severe dyspnoea should guide the clinician to suspect out-of-proportion PH.
Doppler echocardiography
Doppler echocardiography is by far the best method for the noninvasive diagnosis of PH 87, 88, which allows estimation of systolic Ppa from the measurement of the maximum velocity of the TR, using continuous wave Doppler echocardiography. With the same technique, in case of pulmonary regurgitation, it is possible to estimate the pulmonary artery diastolic pressure.
There are strong correlations between values obtained with the measurement of the maximum velocity of TR and those found on RHC 89. While a TR signal can be recorded in 90–100% of patients with clinical signs of right heart failure 90, the rate of success decreases in the absence of these signs 91. In COPD patients, recovery rates of TR signals of sufficient quality are lower, ranging 24–77% 92–94. In a recent study the bias of Doppler echocardiography in the measurement of systolic Ppa compared with RHC was 2.8 mmHg (95% CI −18.7–24.0 mmHg) 9, which is high when one takes into account the modest level of PH (P̄pa <35mmHg) in most COPD patients. Arcasoy et al. 17 have investigated a large series of patients (n = 374) who were candidates for lung transplantation, most of whom had COPD. The estimation of systolic Ppa by echocardiography was possible in only 44% of the patients (hyperinflation precluded optimal visualisation of the heart) and 52% of pressure estimations were found to be inaccurate (>10 mmHg difference compared with measured pressure obtained during RHC). It must be mentioned that it is possible to improve these low recovery rates of TR, mainly due to inflated chest, by the use of saline contrast enhancement.
Estimation of Ppa from Doppler pulmonary flow velocity curves has been reported 93, 95. Correlations between Ppa and the time to peak pulmonary blood velocity (acceleration time) are strong. Even if this method does not allow a precise measurement of Ppa in individuals, decreased acceleration time is a better evaluation of right ventricular afterload than P̄pa measured invasively.
The evaluation of right ventricular dysfunction with Doppler echocardiography has been performed in severe PH 96. Indeed, the Tei index 97 and tricuspid annular displacement 98 predict survival of patients with idiopathic PAH. To the current authors' knowledge, no recent study has been performed in order to determine the clinical value of these measurements of right ventricular dysfunction in COPD.
A good evaluation of pulmonary haemodynamics can be performed with Doppler echocardiography using, in association, several measurements, for example: maximal velocity of TR, pulmonary blood flow velocity and new indices of right ventricular dysfunction. Again, Doppler echocardiography is the best noninvasive method for PH diagnosis, even in COPD, and in spite of technical difficulty. Furthermore, when RHC is mandatory, as in severe PH 99, Doppler echocardiography complements it, since it provides different information 88.
B-type natriuretic peptide
B-type natriuretic peptide (BNP) release is due to increased wall stretch of atria and ventricles and may have a relatively good sensitivity and specificity for the identification of PH in COPD patients 100, 101. However, more and larger studies are needed to determine the benefit of BNP plasma level in the diagnosis procedure of PH in COPD.
Isotopic ventriculography and MRI
Isotopic right ventriculography is a technique used to assess right ventricular global function. Studies performed ∼20 yrs ago have shown significant correlation between right ventricular ejection fraction measured with isotopic ventriculography and Ppa 102, 103. However, this method does not allow diagnosis of PH, owing to the important overlap of this measurement in COPD patients in a stable disease state, compared with normal subjects 102. Therefore, isotopic right ventriculogram adds little information compared to echocardiography, and this method is costly.
MRI allows the measurement of volumes and blood flow in the thorax. New generation devices are not hindered by cardiac motion. At present, it is probably the best method for the measurement of right ventricular ejection fraction and right ventricular mass 81, 104, but its role in the diagnosis strategy of PH in COPD must be determined.
Other tests
Ventilation–perfusion scans and spiral computed tomographic angiography may be useful in patients with severe PH in order to exclude chronic pulmonary thromboembolism. Similarly, COPD associated with sleep apnoeas may lead to severe PH 105. Subsequently, when PH is severe, sleep study may be useful.
Assessment of functional capacity can be performed with a physician-supervised cardiopulmonary exercise test (CPET). Severe PH and particularly out-of-proportion PH in these patients may be associated with a typical “heart failure profile”. This profile is distinguished by increased ventilatory equivalents, decreased maximum oxygen consumption, early anaerobic threshold, failure of stroke volume and oxygen pulse to increase, and altered chronotropic responses, without demonstrable ventilatory limitation, as defined by maximum ventilation reaching maximum voluntary ventilation 106–109. The benefit of studies on CPET is that PH may be an uncommon cause of decreased exercise capacity in COPD patients, particularly in patients with out-of-proportion PH. More data is needed to identify those patients with COPD, probably with more severe PH, who present with a predominantly cardiovascular limitation to exercise capacity.
The 6-min walk distance is generally used as a reproducible, easy and low-cost surrogate to a complete CPET. However, in COPD, the 6-min walk test may be less sensitive to clinical changes than reported in heart failure and in PAH, with an average of 54 m needed to be associated with a perceivable change in clinical condition 110. This is probably due to the fact that exercise capacity would be less exclusively dependent on maximum cardiac output than in heart failure and in PAH. Only one study, which included 45 patients with COPD, has shown that patients with P̄pa >35 mmHg have a 6-min walk distance significantly lower than patients with lower P̄pa. More studies are needed to determine the usefulness of exercise testing for the diagnosis of clinically significant PH in COPD.
RHC
RHC is the gold standard for the diagnosis of PH 87, 99. It allows the direct measurement of pressures in the right atrium, the right ventricle, the pulmonary artery and in the wedge position to estimate left heart filling pressures. RHC is generally carried out using a Swan–Ganz catheter type.
RHC has two main drawbacks: first, it is an invasive procedure including some risks. It needs hospitalisation which may be inconvenient for patients. The second drawback is the inherent methodological limitation of this technique: the fluid-filled Swan-Ganz catheter is incapable of measuring instantaneous pressures and does not give information about the natural pulsing of the pulmonary circulation 88, 111. More importantly, there is no evidenced-based study demonstrating the clinical value of RHC in advanced COPD. At present, invasive measurement of Ppa is of little help for assessment of domiciliary oxygen therapy. Therefore, RHC cannot be used routinely in COPD patients.
The collective body of evidence described above shows that the diagnosis of PH in COPD is not easy and there is not a unique and simple test to confirm or exclude PH. More importantly, at present it is not known whether the recognition of PH in COPD has a clinical impact in the management of patients with COPD, except during the pre-operative evaluation of patients who are candidates for lung transplantation or LVRS. However, the present authors suspect that an unrecognised and untreated severe PH or out-of-proportion PH could have a harmful effect. Indeed, the current authors believe that RHC can help to differentiate diastolic (left) heart failure in COPD and pre-capillary out-of-proportion PH; subsequently it is of use to consider RHC to prescribe the more appropriate treatment. A diagnosis strategy for PH in COPD patients is shown in figure 7⇓.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proposal for a diagnostic strategy for the identification of “out-of-proportion” pulmonary hypertension (PH) in chronic obstructive pulmonary disease. An important elevation of systolic pulmonary artery pressure and a normal left ventricular ejection fraction without an associated disease should encourage a right heart catheterisation. CRF: chronic respiratory failure; DL,CO: diffusion capacity for carbon monoxide; HRCT: high-resolution computed tomography; CT: computed tomography.
TREATMENT
The treatment of PH in COPD is based on oxygen therapy. An important question is: is it necessary to treat PH in COPD with methods other than oxygen therapy? It is known that PH is mild to moderate in most patients with COPD and the necessity of treating this hypertension can be questioned. The main argument in favour of treatment is that PH, even when modest, may worsen, particularly during acute exacerbations, and these acute increases in Ppa may contribute to the development of right heart failure 4, 5. Table 3⇓ summarises all methods of treatments of PH in COPD. The treatment of right heart failure during an exacerbation will not be reviewed.
Methods of treatment of pulmonary hypertension in chronic obstructive pulmonary disease
LTOT
Alveolar hypoxia is considered to be a determinant of the elevation of PVR and Ppa in COPD patients. One of the aims of LTOT is the improvement of PH induced by chronic alveolar hypoxia.
The well-known Nocturnal Oxygen Therapy Trial (NOTT) 112 and Medical Research Council (MRC) 113 studies were not mainly devoted to the pulmonary haemodynamic evolution under LTOT, but pulmonary haemodynamic data were available at the onset in all patients and follow-up RHC was performed in a relatively high number of patients. In the MRC study, 42 patients who survived >500 days from the onset of the study were catheterised again after at ≥1 yr of follow-up 113. P̄pa was stable in the subgroup of 21 patients administered LTOT, whereas it increased significantly (+2.8 mmHg·yr−1) in the control group of 21 patients. In the NOTT study, haemodynamic data at the onset and after 6 months of LTOT were available in 117 patients 114. Continuous (≥18 h·day−1) LTOT decreased slightly but significantly resting (mean -3 mmHg) and exercising P̄pa (mean -6 mmHg) and PVR, whereas nocturnal oxygen therapy (10–12 h·day−1) did not.
Weitzenblum et al. 115 have compared the pulmonary haemodynamic evolution before and after onset of oxygen therapy, with 16 patients acting as their own controls. A reversal of the progression of PH was observed under LTOT; P̄pa was not normalised but returned to its baseline level a mean of 6 yrs earlier. When changes in P̄pa were expressed as changes per year, the difference was also significant, with an increase of 1.5 mmHg·yr−1 before the onset of LTOT versus a decrease of 2.1 mmHg·yr−1 after the initiation of LTOT (p<0.01).
More recently, Zielinski et al. 116 investigated COPD patients under LTOT (15 h·day−1). In 12 patients who completed 6 yrs of LTOT, P̄pa fell from 25±7 to 21±4 mmHg after 2 yrs but slightly increased to 26±6 mmHg after 6 yrs. On average there was a long-term stabilisation of PH on LTOT.
The best haemodynamic results have been obtained in the continuous oxygen group of the NOTT study 114 and in a study reported by Weitzenblum et al. 115, that is in the studies where the daily duration of oxygen therapy was the longest (17–18 h of oxygen per day). Accordingly, continuous oxygen therapy is recommended.
In summary, LTOT stabilises, or at least attenuates, and sometimes reverses, the progression of PH, but Ppa seldom returns to normal. The longer the daily duration of LTOT, the better the pulmonary haemodynamic results.
Nocturnal oxygen therapy in patients with isolated sleep-related hypoxaemia
COPD patients who are hypoxaemic while awake will also be hypoxaemic during sleep. In most COPD patients, hypoxaemia does, in fact, worsen during sleep and especially during REM sleep, as mentioned above. It follows that it is particularly important to oxygenate these patients during sleep. It is sometimes recommended to add 1 L·min−1 oxygen flow to the daytime resting prescription 132.
Some COPD patients do not have significant hypoxaemia when awake (Pa,O2 >60 mmHg; >8.0 kPa) but are hypoxaemic during sleep with a mean nocturnal transcutaneous Sa,O2 <88–90%. It has been hypothesised that sleep-related hypoxaemia, occurring in COPD patients without significant daytime hypoxaemia, could lead to permanent (daytime) PH 71. If this was the case, prescription of nocturnal oxygen therapy to these patients would be justified. In fact, this hypothesis has not yet been demonstrated 117.
Two controlled studies 117, 118 have investigated the effects of nocturnal oxygen therapy administered to COPD patients exhibiting sleep-related hypoxaemia, but without significant daytime hypoxaemia. Fletcher et al. 118 have compared 19 desaturators receiving nocturnal oxygen to 19 comparable desaturators treated with room air. In fact, only 16 patients could complete the 3-yr study: P̄pa increased by a mean value of 3.9 mmHg in the control group (n = 9) and decreased by 3.7 mmHg in patients (n = 7) treated with nocturnal oxygen (p<0.02). Fletcher et al. 118 concluded that nocturnal oxygen therapy had favourable effects on pulmonary haemodynamics. A more recent European multicentric study has compared the evolution of Ppa in 41 nocturnal desaturators randomly allocated to nocturnal oxygen and 35 similar patients receiving no nocturnal oxygen 117. The duration of the study was 2 yrs. A total of 24 patients in the nocturnal oxygen group and 22 in the control group completed the study. Nocturnal oxygen therapy did not modify the evolution of pulmonary haemodynamics, which was the same in the two groups.
The present data, related to the evolution of pulmonary haemodynamics, are not sufficient for justifying the use of nocturnal oxygen in COPD patients who do not qualify for conventional oxygen therapy according to current criteria 1, 132.
Medical treatments dedicated to PAH
Treatments of PAH have shown a dramatic change in the past few years 133. Synthetic prostacyclin (epoprostenol), prostacyclin analogues, endothelin-1 receptor antagonists and phosphodiesterase-5 inhibitors were tested in randomised controlled trials, leading to the approval of several drugs in each class. It is tempting to use these drugs in PH complicating COPD. Unfortunately, only a few studies 109, 119 have been published in this field (long-term effect) and they were, for the most part, uncontrolled. A recent report has shown that one endothelin-1 receptor antagonist had deleterious effects on gas exchanges in a randomised trial performed in COPD patients 120. Therefore, it is strongly recommended to not treat COPD patients with drugs dedicated to PAH outside trials. More randomised controlled studies are required in this area.
Other medical treatments
Experience with vasodilators has come from the treatment of idiopathic PAH. This is based on the belief that pulmonary vasoconstriction is an important component of PH, although this may not be true in most patients. The acute effects of some drugs, such as calcium channel blockers and urapidil, have been somewhat favourable 55, 121 but there have been very few long-term studies, and their results have been disappointing and have shown deleterious effects on gas exchanges 122. Only two studies of angiotensin inhibitors testing a long-term effect (>30 days) on PH in COPD patients have been performed 123, 124. Both studies showed no significant difference in terms of pulmonary haemodynamic variables. Calcium channel blockers, α1-antagonists and angiotensin inhibitors should not be used to treat PH in COPD.
Inhaled nitric oxide is a selective and potent pulmonary vasodilator. It may improve pulmonary haemodynamics and hypoxaemia in COPD 134, but some studies have shown that it worsens ventilation–perfusion mismatch and hypoxaemia 4, 135. There has been one long-term study, that of Vonbank et al. 125 in 40 COPD patients already on LTOT. Patients were randomly assigned to receive either oxygen alone or “pulsed” inhalation of nitric oxide with oxygen over a period of 3 months. The addition of nitric oxide allowed a significant improvement in Ppa, PVR and cardiac output. These results are promising but the technological and toxicological problems related to the prolonged use of inhaled nitric oxide are far from being solved, and clearly further studies in this field are required.
Exercise and respiratory training designated as pulmonary rehabilitation in COPD has a positive impact. It improves exercise capacity and quality of life and reduces dyspnoea on exertion with a high level of evidence 126. Conversely, in severe PH it is believed that physical activities have a negative impact and may favour a worsening of the disease 99. However, the recent American Thoracic Society/European Respiratory Society statement on pulmonary rehabilitation suggests that severe PH is not a contraindication to exercise training 126. Pulmonary rehabilitation has been performed in patients with PAH or severe chronic thromboembolic PH and has shown beneficial results 136. Thus, exercise and respiratory training can be accomplished in COPD patients with PH. It is probably wise to refer patients with severe PH to an expert centre in order to start and monitor pulmonary rehabilitation.
LVRS and lung transplantation
Patients with advanced emphysema may benefit from LVRS 137. Generally, COPD with severe PH (Ppa ≥35 mmHg) are not candidates for LVRS and should rather be considered for lung transplantation. LVRS could have favourable pulmonary haemodynamic effects, since it improves pulmonary function and arterial blood gases. Conversely, it could have deleterious effects, since it may cause a reduction of the pulmonary vascular tree.
There have been few studies on pulmonary haemodynamics before and after LVRS 127–129. LVRS may have adverse effects on pulmonary haemodynamics owing to the reduction of the vascular bed after the resection of lung tissue. Early studies have shown conflicting results, with increases in Ppa after LVRS in one study 130 but not in others 127, 128. A recent study as part of the National Emphysema Treatment Trial has shown no significant differences in terms of P̄pa and PVR, 6 months after medical treatment or LVRS 129.
Lung transplantation is performed in selected COPD patients with end-stage disease. Bjortuft et al. 131 have investigated a group of 24 patients, including 19 with COPD, who underwent single lung transplantation. The majority (15 out of 24) of patients had mild-to-moderate PH at the onset and in these patients P̄pa mean±sem significantly decreased from 28±1 mmHg to 18±1 mmHg after transplantation; there was a similar decrease in PVR. These results were maintained after 2 yrs of follow-up. Therefore, COPD patients with PH normalise pulmonary haemodynamics after single lung transplantation. Lung transplantation may be considered in all patients with severe PH aged <65 yrs and without comorbidities.
CONCLUSION
Chronic obstructive pulmonary disease is a frequent cause of pulmonary hypertension in the population of patients with chronic respiratory failure. Pulmonary hypertension is usually mild to moderate and, nowadays, most of these patients in industrialised countries are undergoing long-term oxygen therapy which stabilises, attenuates, or sometimes reverses the progression of pulmonary hypertension. Conversely, few patients, in spite of long-term oxygen therapy, have severe pulmonary hypertension. In these latter patients a cause of pulmonary hypertension other than chronic obstructive pulmonary disease, which may be treatable, should be sought. When no other causes of pulmonary hypertension are detectable, these patients frequently exhibit a distinctive clinical pattern which shares similarities with other pulmonary vasculopthies, such as idiopathic pulmonary arterial hypertension, a condition termed “out-of-proportion” pulmonary hypertension. The potential impact of drugs indicated in pulmonary arterial hypertension need to be tested in randomised controlled trials in patients with out-of-proportion pulmonary hypertension.
Statement of interest
Statements of interest for A. Chaouat and R. Naeije can be found at www.erj.ersjournals.com/misc/statements.shtml
Footnotes
-
Previous articles in this series: No. 1: Dupuis J, Hoeper MM. Endothelin receptor antagonists in pulmonary arterial hypertension. Eur Respir J 2008; 31: 407–415. No. 2: Gomberg-Maitland M, Olschewski H. Prostacyclin therapies for the treatment of pulmonary arterial hypertension. Eur Respir J 2008; 31: 891–901. No. 3: Behr J, Ryu JH. Pulmonary hypertension in interstitial lung disease. Eur Respir J 2008; 31: 1357–1367. No. 4: Wilkins MR, Wharton J, Grimminger F, Ghofrani HA. Phosphodiesterase inhibitors for the treatment of pulmonary hypertension. Eur Respir J 2008; 32: 198–209. No. 5: Warwick G, Thomas PS, Yates DH. Biomarkers in pulmonary hypertension. Eur Respir J 2008; 32: 503–512.
- Received February 1, 2008.
- Accepted May 29, 2008.
- © ERS Journals Ltd
References










